 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
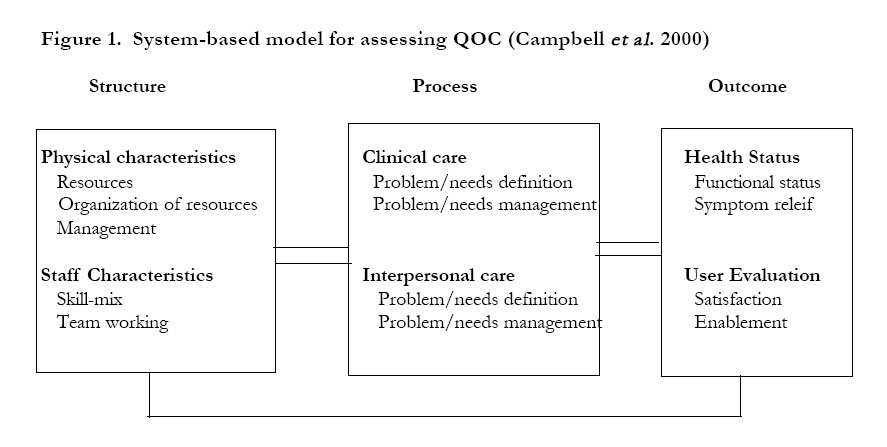
African Health Sciences, Vol. 4, No. 3, December, 2004, pp. 160-170 Quality of care provided to febrile children presenting in rural private clinics on the Kenyan coast T. O Abuya1, C. S Molynuex 2, A.S.S Orago3, S Were4, V Marsh5 1 Kenyatta University-Centre for Complementary Medicine and Biotechnology Code Number: hs04030 ABSTRACT Background: Private sector health facilities are diverse in nature, and offer widely varying quality of care (QOC). Key words: Quality of care, febrile illness, malaria, private practitioners, private clinics INTRODUCTIONPrevailing world systems of health care are complex and heterogeneous. They involve a wide range of services, including public and private health providers1. Current global health policies include strategies to support over-stretched public health sector resources and increase geographic access to effective treatment2 . These strategies include the development of public-private partnerships and optimising the care currently offered by private health providers. Strengthening the role of private health providers presents a challenging stewardship task to governments, and requires both more information and better decision-making tools to support the efficient use of scarce resources 3 . Interventions to improve the quality of care provided through private health providers should be based on context specific situation analyses, including practitioner, user and regulatory authority perspectives. Private sector health facilities are diverse in nature, and offer widely varying quality of care. Overall, private sector providers are popular sources of treatment, illustrated by estimates that 40-60% of all antimalarial drugs are distributed through this sector4, 5 . They provide health care for clients from a wide socio-economic background and for a broad spectrum of medical conditions, such as malaria, tuberculosis and sexually transmitted diseases 6, 7 . In addition, this group of providers are themselves a heterogeneous group, ranging from qualified private medical practitioners to untrained informal providers 4, 8. However, the existing information on the quality of care offered in the private health sector in developing countries is patchy, and few sustained interventions to promote quality of care have been implemented or evaluated 9, 10, 11 The available data on quality of care in the private sector are complex to assess, with varying emphasis on different aspects of quality of care. Some studies have shown that services in the private sector are more prompt and convenient than the public sector 12, 13 . Others have indicated deficiencies in process and structural components of quality of care 12, 14, 15, 16, 17, 18 . The paucity of consistent data on private provider characteristics, quality of diagnosis and treatment and levels of patient adherence to advice undermine efforts to develop useful interventions to build public-private partnerships and optimise quality of care 8, 19 . By 1998, 49% of all health facilities in Kenya were privately owned, and 29% of them owned by for-profit providers 20 . The Kenya Health Sector Strategic Policy (KHSSP) emphasises the need to create an enabling environment for private sector providers, but limited country information exists on the sector 20, 21 . This is especially the case for rural areas of Kenya, where access to health services is limited and private practitioners could make a valuable contribution to improving health in communities. Compounding the need for work in QOC is the increasing burden of diseases such as malaria. It is a leading cause of morbidity and mortality. At least 1 million people die of malaria each year, primarily children under five years of age in sub Saharan Africa 22 . In Kenya, an estimated 72 children in this age group die as a result of malaria infection every day 23 . The KHSSP confirms the strategic importance of malaria control nationally, placing it alongside HIV/AIDS, TB, the expanded programme for immunization (EPI), environmentaldiseases and the integrated management of childhood illnesses (IMCI) as a priority area for support 20, 24 . This study therefore aimed to describe the nature and practices of typical private health providers in a rural area of Kenya, focusing on the quality of care provided for children with febrile illnesses. We also aimed to describe users’ and district health managers’ perspectives on quality of care offered in private clinics and the potential for optimising private practitioner services. Assessing quality of care in the private health sector The search for ways of assessing quality of health care has continued for almost a century, but no universally accepted method of measuring quality of care exists 25, 26 . A method commonly used, incorporates three key domains of structure, process and outcome (Fig 1) 27 . Structural components describe the physical resources, such as buildings and equipment, as well as characteristics of personnel and the geographic situation. Areas of process concern the clinical and interpersonal care provided by a practitioner. The outcome domain addresses the consequences of care given. Outcome components often receive less attention than structure and process dimensions in quality of care assessments METHODS Study area The study was carried out in a rural area of Kilifi District on the Kenyan coast. The district has a population of 544,303 28. The study area contained the rural areas of an administrative division within Kilifi district, with a population of 70,000 people living in 309 km2. The formal health sector facilities serving this area were two dispensaries and 10 small private clinics. The district general hospital is situated in Kilifi town, approximately 20 km from the centre of the study area. Detailed reports of the demography, malaria endemicity, climate and anthropology of the study area have been published elsewhere 29, 30. Study DesignThe study was descriptive, combining quantitative and qualitative methods. Study participants were private practitioners, private clinic users and members of the district health management team. Non-profit making facilities, such as mission hospitals, non-governmental organisations (NGOs) and urban facilities were excluded. A map of the private clinics in the study area was constructed based on the information from the district public health office and data from a recent demographic surveillance survey. Practitioners from all 10 private clinics in the area were approached to participate in the study. However, 2 practitioners were not traceable and one refused to participate. Practitioners from the remaining 7 clinics, and caretakers of febrile children aged 6 months to 10 years attending these clinics, were recruited to the study. Data collection methodsData collection questionnaires and observation checklists were adapted from one standardised tool developed to study quality of care in health facilities and a study carried out in Pakistan. 31,32. Survey of structural featuresPrivate clinics were visited to assess the building type, equipment, facilities, standards of hygiene, characteristics of personnel and drugs stocked, using a structured questionnaire. Direct observations of consultationsWe observed consultations between practitioners and users attending with febrile children to assess clinical and interpersonal aspects of quality of care. The observations covered history-taking and examination practices, types of investigations performed, prescribing practices, information given and communication skills. Trained field workers conducted observations using pre-tested structured checklists. Inter-observer variation was minimised during training by repeated assessments with paired observations and discussion of findings. Observations were conducted continuously over a period of 14 days in each clinic, to reduce the behavioural bias associated with observational methods. The observation records were assessed for quality of care by experienced paediatricians using national guide-lines. Adequacy of clinical care was based on the quality of history taking, examination, and diagnosis, prescribing practices and follow up and referral practices. Information given by the practitioner on the diagnosis, symptom relief, and disease outcome and future prevention of illness was also assessed. Prescribing practices were compared with the recommendations made in the national malaria treatment guidelines. These recommendations include the presumptive treatment of childhood fevers as malaria, in keeping with WHO and IMCI policy. Interpersonal care during the consultation was assessed by observations on specific areas of the practitioner’s behaviour. These were attitudes shown at the time of introduction, adequacy of time spent, care taken in listening and efforts made to assess patient understanding. User interviews: exit survey and follow up interviews at home
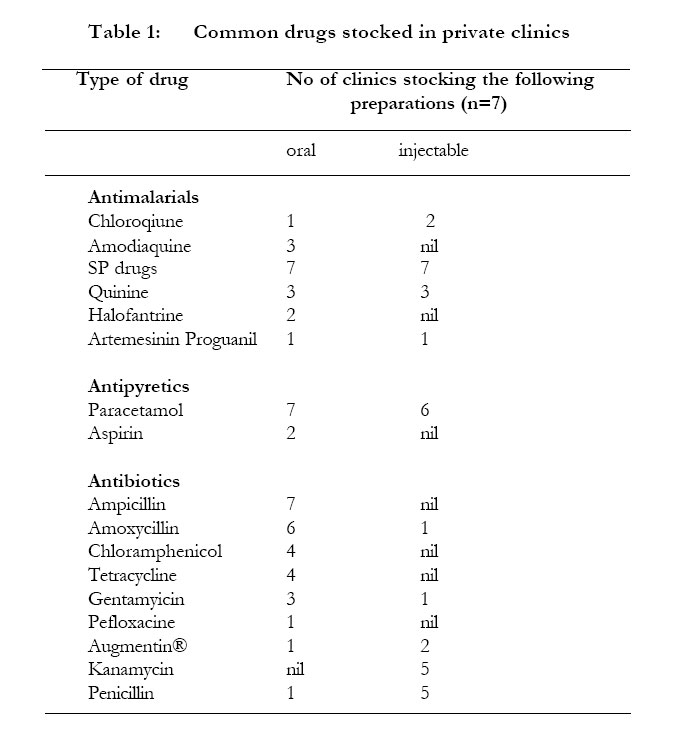
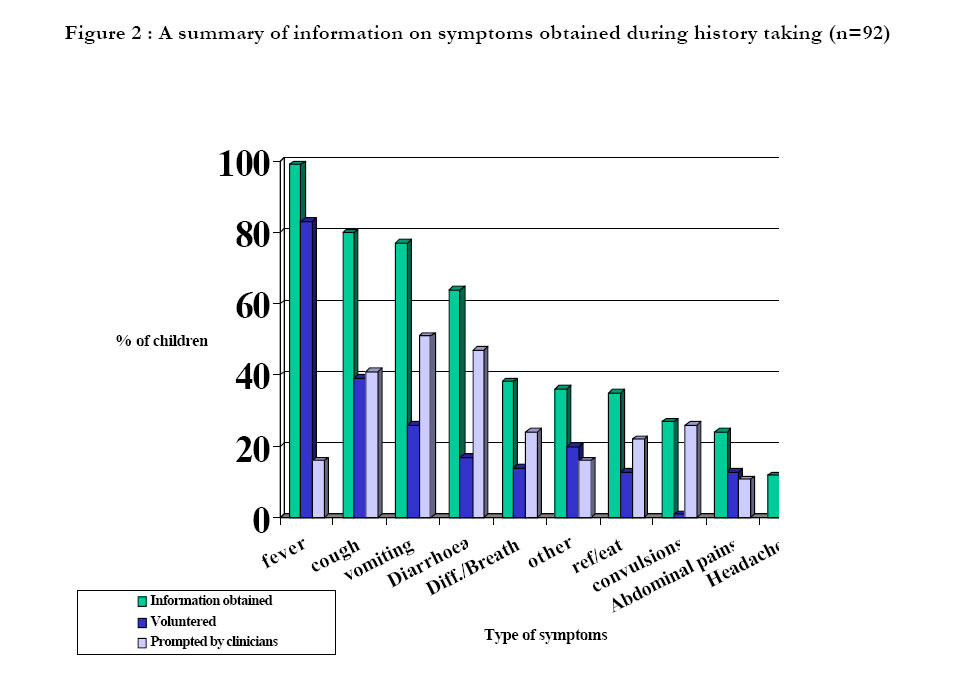
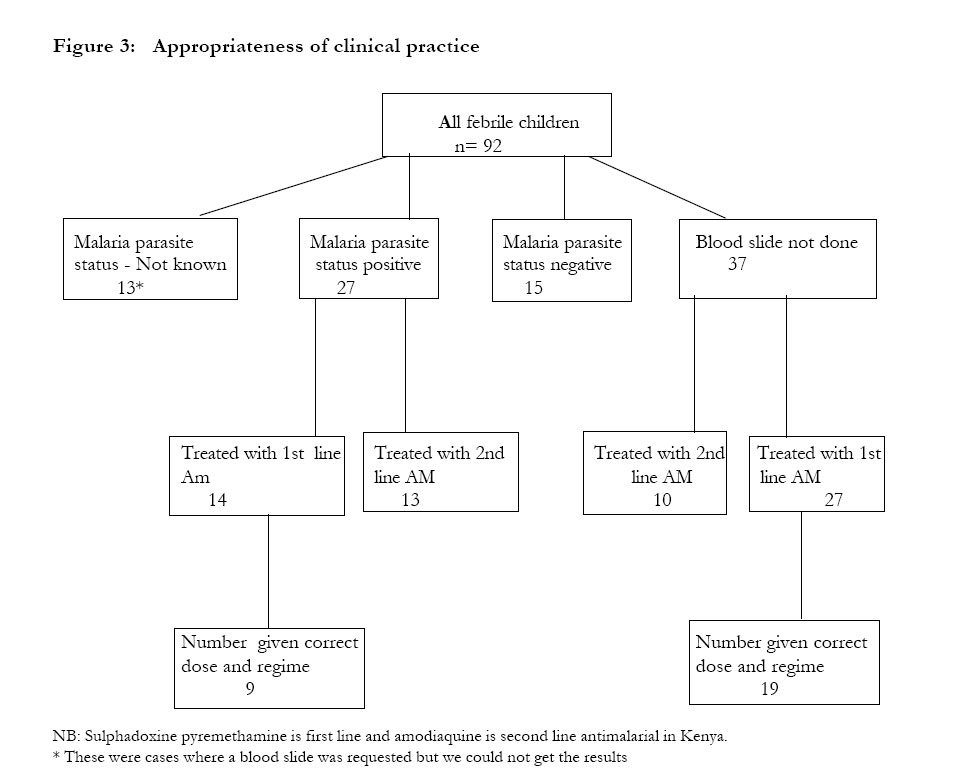
Following observation of a consultation, the fieldworker interviewed the caretaker outside the facility to confirm the identity of drugs given, establish immediate recall of drug use information and examine drug labelling or written instructions. Consent for home visits at an unspecified time was also sought. Home visits were conducted during the following two weeks to assess adherence to advice, discuss reasons for drug use practices and assess perceptions of outcome. All our study participants were from the demographic surveillance area of the research center where active census is carried out every six months. This made it possible for our experienced field staff to use census maps to locate the homes. In-depth interviewsIn-depth interviews were conducted with seven private practitioners and three members of the district health management team. Areas for discussion with district health managers were attitudes towards private practitioners, existing linkages and future potential strategies for improving quality of care. Discussions with practitioners focused on their attitudes towards increased private-public sector interaction and preferred approaches to improving quality of care in their own practices. Data analysisQuantitative data were coded and entered using Fox pro (version 3.5). Frequencies and percentages of variables were measured with 95% confidence interval using Epi Info (version 4). RESULTS Structural components Characteristics of staff in private clinics The majority of the clinics in this study were owned and run by single-handed trained medical practitioners. These were either clinical officers (a paramedical cadre with 3 years of tertiary level clinical training) or nurses, operating from rented premises. Occasionally, a government health worker was contracted in when the owner was unable to attend. These occasional practitioners were also either registered clinical officers or state-enrolled nurses, although, on one occasion, a trainee clinical officer temporarily provided services. Most of the private practitioners were aged between 30 and 50 years, and had worked within the government services for 10 years after training, as required by law, before setting up their own full-time private practices. One private practitioner had established his clinic after official retirement from public service at 60 years. Half of the clinics employed full-time laboratory technicians and one employed a full-time nurse aide. All the clinics employed one person to provide administrative, secretarial and cleaning support. Buildings and equipment in private clinics The majority of premises maintained adequate standards of hygiene (6/7). In one clinic, hygiene was graded as inadequate because large amounts of used cotton wool were consistently present on floors amongst other reasons. Three clinics were supplied with electricity. One received piped water and six operated with stored water in containers, often stored outside the consultation room. Thermometers and stethoscopes were present in all clinics, and a sphygmomanometer in most. All the clinics stocked plastic disposable syringes and sterile gauze but there were no separate disposal facilities for used needles or contaminated materials in four clinics. Four clinics had working microscopes and three had weighing scales. Two clinics stocked tetanus vaccine and offered family planning services. Most clinics were open between 08.30 and 17.00 hours. In three clinics where the practitioner lived nearby, services were available outside these hours. Common drugs stocked in private clinics Table 1 shows the drugs stocked in the study clinics. The most common antimalarial drugs stocked belong to the sulphadoxine-pyrimethamine (SP) group. Others were amodiaquine preparations, quinine and chloroquine. Drugs such as artemesinin, proguanil and halofantrine were rarely stocked. Process components History taking, examination practices and diagnoses made Figure 2 shows the history taking practices and diagnoses made in 92 observed consultations. Practitioners obtained information on the presence of fever in almost all cases (99%), although caretakers usually volunteered this. However, information on danger signs, such as difficulty in breathing and convulsions, was not usually sought (38% and 27% respectively). The most common examination procedures were temperature measurement (89%) and stethoscope examination (83%). Temperature was most commonly measured using a mercury thermometer in the axilla (77%), although this was done by touch in a minority (23%). Practitioners palpated the abdomen in 71% of cases, assessed pallor by examining the conjunctiva in 80% children, and counted the respiratory rate, using a watch, in 32%. Very few children were weighed (4%) or assessed for severe weakness (1%). 88 children (74%) were diagnosed to have clinical malaria. Awareness of the importance of malaria amongst practitioners was high, as illustrated by one practitioner’s comment: “If you cannot diagnose a malaria case from this area then you have no business working here.” Standards of clinical practice The diagnoses made by practitioners were usually consistent with the history obtained (62%), and inconsistent in a fewer consultations (3%). However, history taking was found to be incomplete in 27%, and a further 7 records could not be assessed through illegibility. Figure 3 summarises the diagnostic and prescribing skills important to malaria case management. An important finding was the high proportion of febrile children receiving either first line (64%) or second line (36%) recommended antimalarial drugs. However, many of those given first line drugs were prescribed inappropriate doses or regimes (57%). For SP drugs, the majority of incorrect dosages were under-treatments, while the commonest incorrect regimes were divided doses over one day, or repeat single treatments after an interval of one week. The commonest inappropriate amodioquine prescription was for a single dose, in contrast to the recommended three-day regime. A further inconsistency noted was the regular prescribing of an antimalarial drug to children with negative slides. 78% prescriptions contained an antibiotic and 67% an antipyretic drug. Prescriptions contained an average of 3.4 different drug types (IQR 2.50-4.00), and these were mostly dispensed within the facility. 59 (64%) prescriptions contained at least one injection, with an average of 2.17 injections per prescription (IQR range 1.00-3.00). Paracetamol (17%), crystalline penicillin (15%) and chloroquine (12%) were the most common injections given. User, provider and DHMT perspectives on quality of care in private clinics Factors underlying use of private clinics and adherence to adviceClients reported that the main advantages offered by private clinics over government clinics are better geographic access, more reliable supplies of drugs and more rapid treatment. Additionally, private clinics were perceived to provide reliable services. This finding was supported by high reported rates of adherence to advice, with 88% adherence to antimalarial drug use, 86% to antipyretic drug use and 75% to all injections prescribed. Reported reasons for non-adherence included the perception that an improvement in condition indicates treatment is no longer needed, misunderstandings about the advice given or advice being forgotten. Providers often believed that traditional beliefs and practices lay behind non-adherence to their advice, with clients moving between different health care systems where recovery does not occur quickly. “…If parents are strong believers in mburughas (traditional healers), they will consult one when my prescription fails to heal the patient quickly, then he or she will come back to me for the course prescribed.” Existing linkages between public and private health sectors
Both private practitioners and district health managers expressed the view that existing linkages between the public and private health sectors within the district are haphazard and inadequate. The main existing linkage is through the registration system. All clinics are registered through the district medical officer of health after an initial inspection of the premises. No further visits would normally be paid unless problems are reported. There are no mechanisms for monitoring or supervision of activities, or for on-going training. Two clinics operate immunization services using government owned refrigerators and EPI vaccines. A further linkage is the background of most private practitioners, since all had been trained and worked in the government sector prior to setting up in private practice. Recommendations for change District managers’ recommendations focused primarily on the need for more systematic regulation, monitoring and supervision activities, such as:
Recommendations from private practitioners were mainly in the area of increased training and financial support. These included:
DISCUSSION
This study examined two aspects of private clinical practice in a rural malaria endemic setting; the quality of care offered to febrile children and stakeholder perspectives on the sector, including possible strategies for change. Several QOC components were found to be adequate, including structural features and many aspects of clinical and interpersonal care. Important shortcomings were the failure to ask for malaria danger signs, frequent use of inadequate dosages and regimes of antimalarial drugs, unnecessary use of many different drugs (polypharmacy) and a high and inappropriate use of injections. On the other hand, important strengths were the educational background of practitioners, good levels of drugs stocked and equipment provided, and generally adequate diagnostic abilities. Perhaps as important is that clients generally expressed positive attitudes towards private practitioners and all stakeholders supported increasing the role of private practitioners in malaria control in the district. However, district health managers placed greater emphasis on the need for increased regulation, while private practitioners perceived more need for in-service training. We acknowledge that it may be difficult to generalise from the findings of this study, since they have been derived from observations in a small number of facilities without a comparison group such as public facilities or other private facilities from a different setting. However, the findings have been consistent between clinics, the clinics studied represent the majority of such facilities in a population of 70,000 people, and were judged to be typical rural clinics by the district health management team. One private practitioner approached refused to participate, and we do not know how this clinic might vary from those included in the study. Further caution is needed in interpreting the results of the observational work, since it is accepted that overt observation may lead to changes in practices in the group under observation. However, this is a standard methodology, it has been shown to be more accurate than record review and we have compensated to some extent by conducting continuous observations in each clinic over a period of 14 days 33, 34 As previously stated, descriptive studies on quality of care in private practice have illustrated great diversity. Some studies describe similarities, such as the preponderance of well-trained practitioners and adequate structural facilities, while others describe marked differences 15 17 32 35. Inappropriate prescribing patterns have also been commonly reported for this group, particularly the high rate of injections 15,17,35,36. However, this latter phenomenon is also frequently encountered in the public health sector, and few studies have compared the rate of inappropriate practices in private and public health facilities. Where this has been done, it often appears that the shortcomings in private practices may also be seen in their public counterparts. For example, studies in rural China and Nigeria found no difference in the quality of care in private and public facilities, and no increase in the likelihood of receiving appropriate treatment through a public clinic 25. The diversity of findings indicates the importance of context specific situation analyses for planning interventions to optimize quality of care. In our study clinics for example, PPs appeared to prescribe recommended antimalarials in accordance with national malaria guidelines and exhibited a high level of awareness on the need for presumptive treatment of malaria (see Fig 3). These findings indicate their potential role in prompt treatment of malaria in endemic areas. However, a summary of appropriateness of treatment given indicates an element of ‘overtreatment’ suggesting the potential for wastage of household resources that would otherwise be used efficiently. This was evidenced further by use of injections some of which are dangerous (chloroquine) and others unnecessary (paracetamols). Generally PPs exhibited good interpersonal care as indicated by careful listening and giving enough time for carers to explain their problems. Perhaps this explains high compliance rates and the client’s positive perception towards PPs. Their popularity may be associated with their ability to adjust treatment to the client’s purchasing power. Since carers are often unable to assess technical care, they resort to judging quality through more familiar modalities such as interpersonal care. Such imbalances result in patients being exposed to inadequate care over which they have little influence 37. Strategies for change and conclusions
A wide range of approaches are needed while working with the private sector 37. This study provides suggestions that fit well with recommendations that have been made in malaria endemic countries and interventions that have been tried elsewhere. In an attempt to improve care there is need for balance of support (training, incentives, loans) and regulation (inspection, fines, closures). Structural problems may be addressed through regulatory and participatory measures, and through financial support to help providers access essential diagnostic facilities. Even though there are no specialized institutions that finance health providers 21governments could consider providing subsidies or incentives. Updates on current treatment guidelines are needed to improve clinical care. These guidelines require adaptation to reflect contextual realities and their distribution should be accompanied by PPs training. Such approaches have been used in India with PPs and Kenya with shopkeepers and observed to have an impact on levels of practice 16,38. In addition, strategies to monitor and involve institutional support on updated standard guidelines are important. Such institutions could be professional bodies, public facilities and other health development partners. Finally other recommendations may include organizing periodic fora to discuss clinical cases through workshops and seminars, where peer discussions can be held between PPs and government providers. Such approaches have been used in Indonesia and recorded reduced inappropriate use of injections 11. The data obtained from this study provide constructive information to district level managers who have the role of maintaining quality of health services. Rural PPs are potentially well placed for treatment of febrile cases in remote settings away from government clinics. There are no reasons to believe that these clinics are different to others in similar areas of Kenya, although further studies examining QOC in different settings would be instructive. Evident benefits are their accessibility and potentially client sensitive services. Interventions should be planned to address the weaknesses demonstrated in the system as part of district-wide malaria control planning. Such approaches will support the over-stretched public health sector in providing early adequate health care to communities, and impact on health in communities as well as the economic resources of households and the public health sector. The study identifies the need to consider involvement of the for-profit providers in the implementation of the IMCI guidelines in Kenya. REFERENCES
Copyright © 2004 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs04030t1.jpg] [hs04030f2.jpg] [hs04030f3.jpg] [hs04030f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}