 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
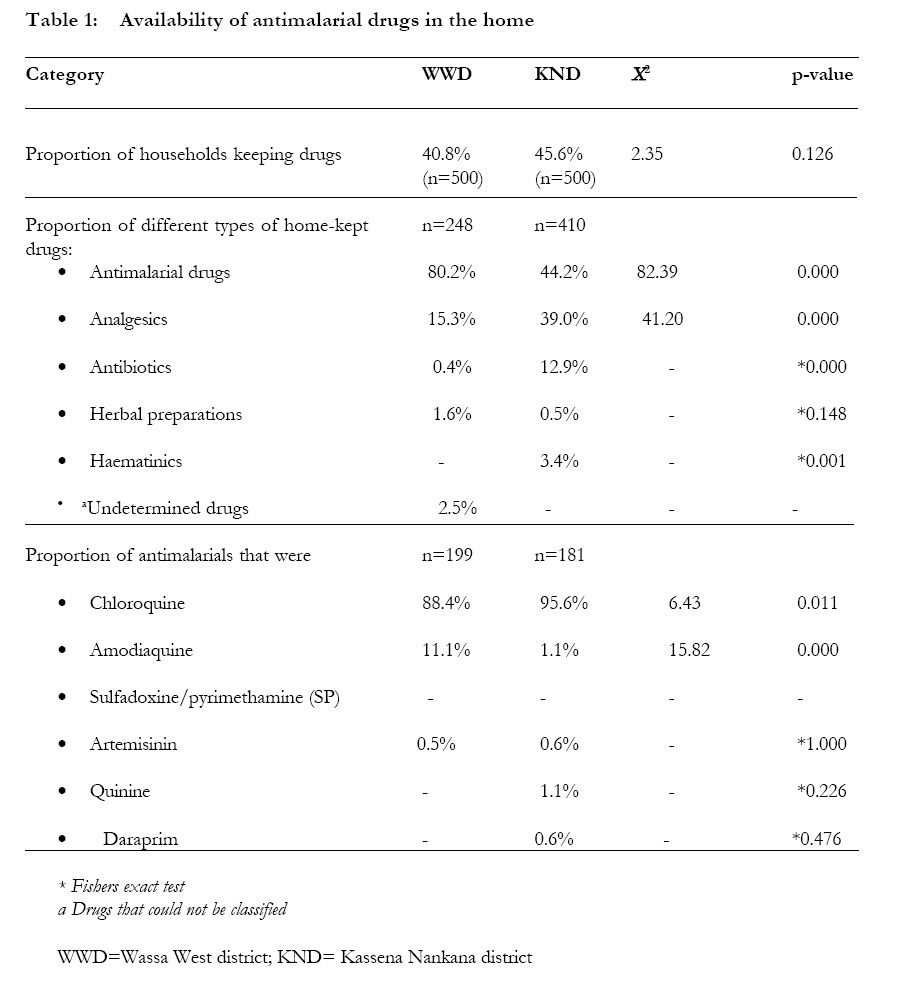
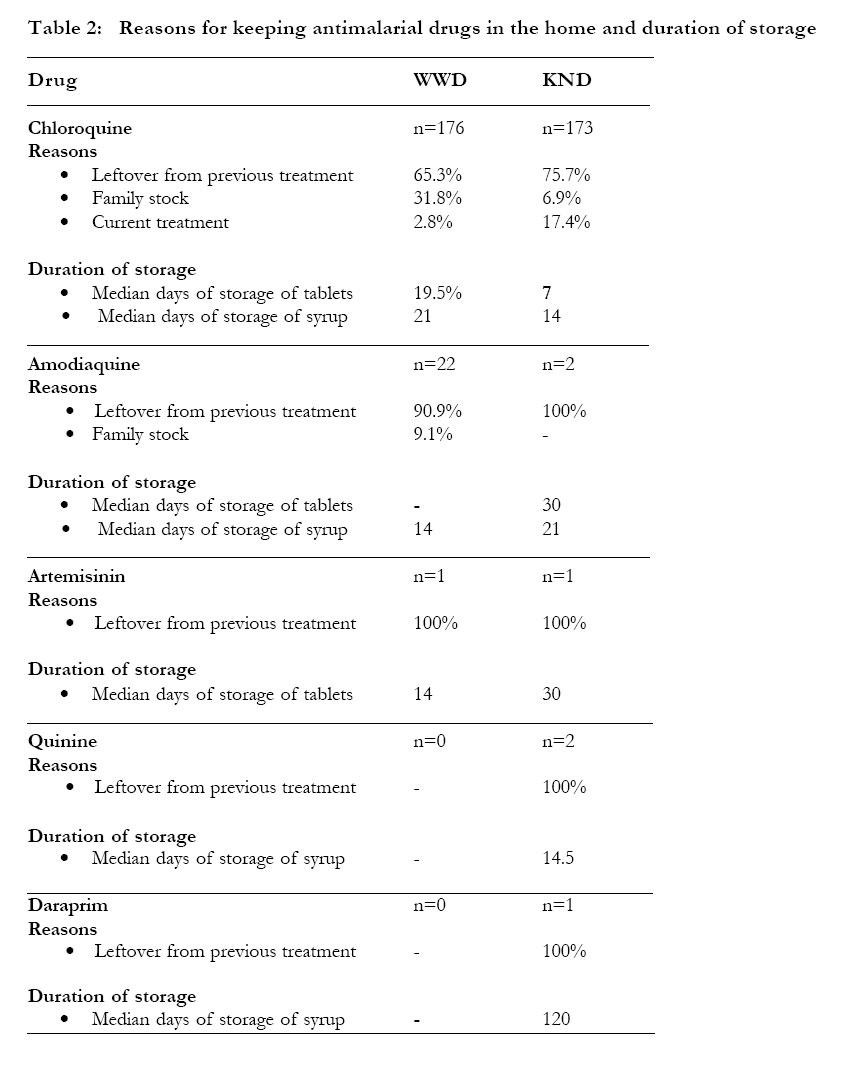
African Health Sciences, Vol. 4, No. 3, December, 2004, pp. 171-177 Antimalarial drug use among caregivers in Ghana Benjamin K. Abuaku 1, Kwadwo A. Koram1*and Fred N. Binka 2 1 Noguchi Memorial Institute for Medical Research, University of Ghana, Legon, Ghana Code Number: hs04031 ABSTRACT Background: Chloroquine remains the first line antimalarial drug in Ghana. However, the emergence of Plasmodium falciparum resistance to chloroquine is a major obstacle to the national control strategy of case management. This study provides information on some of the reasons underlying chloroquine treatment failure in the country. INTRODUCTION Malaria remains a major public health problem in Africa. It has been estimated that out of the over one million deaths caused by malaria worldwide, 90% occur in sub-Saharan Africa. Malaria is also directly responsible for 20% (one in five) of childhood deaths in Africa, and indirectly contributes to illness and deaths from respiratory infections, diarrhoeal diseases and malnutrition1 . Malaria is endemic in Ghana, and it is estimated to account for 40% of all out patientattendance and over 25% of under-five mortality. The current control strategy in Ghana has case management based on prompt recognition and adequate treatment as its main focus, using chloroquine as the first line drug2 . Studies in Africa have shown that the initial treatment of malaria/fevers often takes place at home without consulting trained professionals3, 4, 5, 6 . Although home-or community-based treatment has the potential of positively impacting on malaria control, in terms of prompt recognition and treatment to prevent complications and also reduce childhood mortality, there can be problems with antimalarial drug use, particularly where there is inadequate training of people in the use of the particular drug. This study to assess the patterns of antimalarial drug use among caregivers was undertaken to complement data on studies of the efficacy of chloroquine for the treatment of uncomplicated malaria in Ghana. The objectives of the study were to determine availability of antimalarial drugs at the household level; to assess theduration and reasons for keeping antimalarial drugs in the home; to determine appropriateness of treatment given to patients who were suspected to have malaria in the home; and to assess caregivers’ knowledge of chloroquine doses for children and adults. The study was conducted to provide information that will contribute to understanding the reasons underlying treatment failures in the country and also to identify ways of improving appropriate use of antimalarial drugs by caregivers at the household level. METHODS Study areas The study was conducted in the Wassa West and the Kassena Nankana districts, two of the six sentinel districts involved in chloroquine efficacy studies in Ghana between 1998 and 2001. The Wassa West district is located between latitudes 4o00/ and 5o40/ North of the equator and between longitudes 1o45/ and 2o10/ west of the zero meridian with a population of 226,449 (Ghana Statistical Service data). The vegetation is mainly secondary rain forest with an annual rainfall of 1878mm. Malaria is hyperendemic and is the primary cause of child morbidity and mortality7. Therapeutic efficacy of chloroquine in the treatment of uncomplicated Plasmodium falciparum malaria in the district is estimated to be 67.3% 8. Kassena-Nankana district lies within the Guinea savanna woodlands between latitudes 10o30/ and 11o00/ north of the equator and between longitudes 1o00/ and 1o30/ west of the zero meridian with a population9 of 140,000. The Kassena-Nankana. Mean annual rainfall is 900 mm. Malaria is holoendemic and is the leading cause of morbidity and mortality10,11. Therapeutic efficacy of chloroquine in the treatment of uncomplicated Plasmodium falciparum malaria in the district is estimated to be 76.9% 8. Study design The study was descriptive involving a questionnaire survey to determine the extent of self-administration with antimalarial drugs in homes and the pattern of drug use. Structured questionnaires were administered to 500 caregivers in each district. There were inventories of home-kept antimalarials by direct observation. The study received approval from the Institutional Review Board (IRB) of the Noguchi Memorial Institute for Medical Research (NMIMR), University of Ghana. Written consents was obtained from household heads and caregivers. Sampling Caregivers of children under 10 years were selected using a multi-stage sampling method. Ten communities from a list of communities contributing data to the chloroquine efficacy studies were selected by simple random sampling. Subsequently, 50 households were systematically selected in each community and caregivers of children under 10 years identified and interviewed. Data processing and analysis Data collected were entered into a computer using Epi Info 6 (version 6.0b) and edited record after record to ensure accuracy. Statistical Package for Social Sciences (SPSS version 10 for windows) was then used to do descriptive and analytic cross tabulations. five percentof caregivers interviewed were re-interviewed by field supervisors to ensure quality of data collected. Chi-square (C2) test was used to test differences in proportions between the districts for the commonly used antimalarial drugs. RESULTS Socio-demographic and economic characteristics of caregivers The ages of caregivers in the two districts ranged between 16 and 75 years for Wassa West with a median age of 31 years, and 15 to 68 years for the Kassena Nankana district with median age of 30 years. The greater proportions of caregivers (98.4% for Wassa West and 99.2% for Kassena Nankana) were females; 85.6% and 88.4% were married in the Wassa West and the Kassena Nankana districts respectively. Approximately 83% of caregivers in the Wassa West district and 56% in the Kassena Nankana district had had some formal education (p=0.000). The mean sizes of households were 5.3 and 5.7 in the Wassa West and the Kassena Nankana districts respectively. Home-kept drugs among caregivers Inventory on home-kept drugs showed that 204 (40.8%) households in the Wassa West district kept a cumulative total of 248 drugs at home whereas 228 (45.6%) households in the Kassena Nankana district kept a cumulative total of 410 drugs at home. The proportions of drugs kept in homes in the 2 districts are shown in table 1. The antimalarial drug commonly kept in homes in both districts was chloroquine, and the formulation was usually syrup; 92.6% in the Wassa West district and 65.9% in the Kassena Nankana district. Reasons for keeping antimalarial drugs in the home and duration of storage
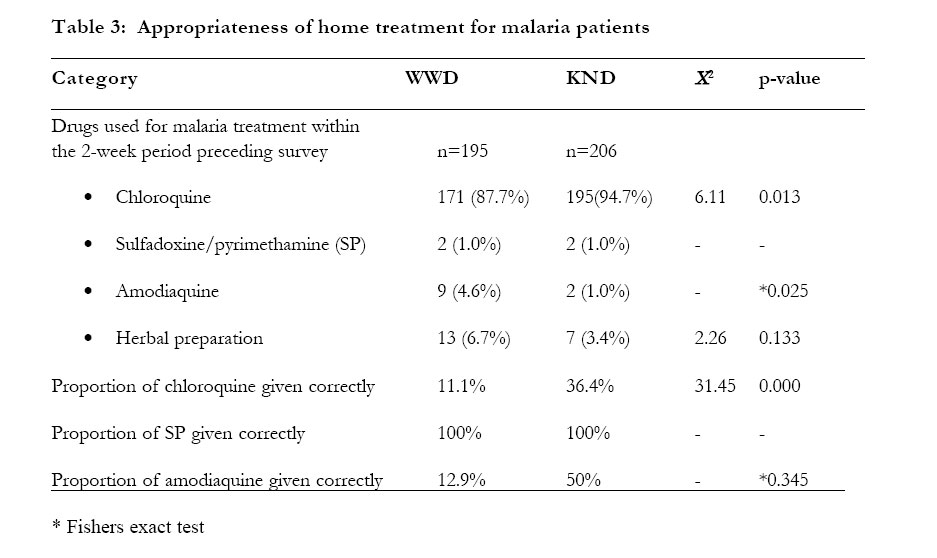
The main reason given by caregivers in both districts for storing the antimalarial drugs found in their homes was “leftovers from previous treatment” (table 2). Among home-kept antimalarial drugs, chloroquine syrups were stored for longer periods in both districts compared to tablets (21 days versus 19.5 days in the Wassa West district and 14 days versus 7 days in the Kassena Nankana district). Appropriateness of home treatment for malaria patients A total of 195 and 206 people in the Wassa West district and the Kassena Nankana district, respectively, had received malaria treatment within the 2-week period preceding the surveys. Caregiver’s descriptions of treatment given were classified as appropriate or inappropriate based on the standard treatment guideline of the Ministry of Health (2000). These descriptions were 11.1% - 50.0% appropriate for chloroquine and amodiaquine but 100% appropriate for sulfadoxine/pyrimethamine in both districts (table 3). Caregivers’ knowledge of child and adult chloroquine doses When caregivers were asked to give the chloroquine treatment regimen for malaria for any of their children under 10 years, 21 out of 488 (4.3%) proved knowledge of the right regimen in the Wassa West district as against 34 out of 500 (6.8%) in the Kassena Nankana district. The difference in proportions was not statistically significant; p< 0.0872. However, fewer respondents in the Wassa West district knew the correct adult treatment dose compared with respondents in the Kassena Nankana district (24% versus 59.2%); p<0.0001. The differences within the Wassa West and Kassena Nankana districts were highly significant in terms of proportions of appropriateness of caregivers description of chloroquine treatment regimen for malaria in children under 10 years compared with the description for adults; 4.3% versus 24% in the Wassa West district and 6.8% versus 59.2% in theKassena Nankana district (p < 0.0001 in both cases). DISCUSSION The study has shown that a significantly higher proportion of home-kept drugs were antimalarials in the Wassa West district compared to the Kassena Nankana district (80.2% versus 44.2%; p=0.000). This pattern was expected due to the fact that malaria was hyperendemic in the Wassa West district and holoendemic in the Kassena Nankana district. There was therefore a higher tendency to use antimalarials in the Wassa West district. However, the antimalarial drug commonly kept in homes in the 2 districts was chloroquine (88.4% in the Wassa West district and 95.6% in the Kassena Nankana district), which is relatively affordable and is the recommended drug of choice for the treatment of malaria in the country. The study also showed that the majority of the antimalarial drugs found in homes were those saved from previous treatment. For instance, the proportions of chloroquine saved from previous treatment were between 64.4% and 76.3% for syrups and 69.2% and 74.6% for tablets in the 2 districts. These proportions are higher than the findings of Vundule and Harakurwa that 27% of study participants in Zimbabwe stopped taking chloroquine when they recovered and saved the remaining tablets12 . Though higher proportions of antimalarial drugs kept in the home were leftovers after previous treatment, it is not known whether the leftover drugs were used for subsequent episodes of malaria. If the drugs were used, then there could be problems with their efficacy (particularly with syrups) because of the probable decline of potency as a result of the long storage periods of between 14 and 21 days, and this could lead to treatment failures that will impact negatively on malaria morbidity and mortality. The issue of keeping tablets from previous treatment could be a sign of treatment non-adherence in the 2 districts. This might promote progression of drug resistance that results from use of sub-optimal doses of drug13 . The study showed that although greater proportions of people who were home-treated for malaria within the 2-week period preceding the surveys received chloroquine, caregivers’ descriptions of doses were mostly inappropriate (88.9% in the Wassa West district and 63.6% in Kassena Nankana district). However, the proportion of caregivers giving correct doses of chloroquine was significantly higher in the Kassena Nankana district (36.4% vs. 11.1%). This pattern of chloroquine use could probably be one of the factors influencing high treatment failure observed in Wassa West by Koram8. Several studies in malaria endemic areas have also reported inappropriate use of antimalarial drugs in the home. The proportion of respondents in these surveys reporting inappropriate use of chloroquine has ranged between 60% and 80% 14,15. Thus the findings of this study do not vary much from previously reported data and compare well with regional data from Nigeria16and Senegal 17. Generally, caregivers’ descriptions of chloroquine regimen for patients were more appropriate in adult cases than in child cases in both districts. The higher proportions of caregivers describing the correct dose of chloroquine for adults compares well with the observation in Zambia18. The study has also shown the ease with which sulfadoxine/pyrimethamine is administered as single dose therapy by respondents. This is evidenced by the finding that caregivers’ descriptions of treatment given to family members who had received sulfadoxine/ pyrimethamine for their malaria treatment within the 2 week period preceding the survey was 100% appropriate in both districts. Furthermore, there was no stock of sulfadoxine/pyrimethamine in any of the homes visited in the 2 districts. These findings suggest that single-dose therapies might increase compliance of clients. In conclusion, this study has shown that the main drug used in the treatment of malaria in homes in the 2 districts is still chloroquine, which is the first line antimalaria drug in Ghana. However, descriptions of child doses by caregivers were mostly inappropriate. The issue of inappropriate estimation of treatment doses for chloroquine, particularly in children, by caregivers raises a potential problem that need to be addressed. Distribution of pre-packaged antimalarials for the various child age groups could enhance the knowledge and compliance of caregivers as demonstrated by Ansah19 and Gomes 20. ACKNOWLEDGEMENT We thank field staff, supervisors, data entry clerks and the District Health Management Teams for their suport. This study was funded by the Multilateral Initiative on Malaria (MIM)/WHO Special Program for research & Training in Tropical Diseases (TDR) grant ID 980034. REFERENCES
Copyright © 2004 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs04031t3.jpg] [hs04031t1.jpg] [hs04031t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}