 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 4, No. 3, December, 2004, pp. 178-181 Structural findings at hysterosalpingography in patients with infertility at two private clinics in Kampala, Uganda Elsie Kiguli-Malwadde* and Rosemary K. Byanyima Department of Radiology, Mulago Hospital and Makerere University Medical School, Kampala, Uganda
Code Number: hs04032 ABSTRACT
Introduction: Hysterosalpingography (HSG) is still a commonly used investigation in the evaluation of the female genital tract and the main indication for HSG is infertility. Keywords: Hysterosalpingography, Infertility. INTRODUCTION Hysterosalpingography is the most widely used and readily available radiological investigation for infertile women in Uganda, apart from ultrasound scanning. From Mulago Hospital, which is the main referral hospital in Uganda, records show that infertility ranks high on the list of indications for attendance of gynecological out patient clinics. It is documented that 15% of all women experience primary or secondary infertility at one point in time in their reproductive life. Tubal causes of infertility account for 35% to 40% of cases of infertility 1 . HSG is still the most commonly used technique for evaluation of tubal blockage in Uganda. Other techniques for assessing structural causes of female infertility like sonohysterography(Hycosy), laparascopy and hysteroscopy are increasingly used elsewhere. Despite the advantage of being radiation free, they lack the clear tubal resolution and definition that conventional x-ray HSG offers. MATERIALS AND METHODS A retrospective review of records of 289 consecutive patients who underwent HSG at two private clinics in Kampala during the period July 1997 and December 2000 was done. These patients were referred for this examination from various private clinics and hospitals around Kampala. The clinical data and radiological findings were entered into a pre-coded data sheet. The HSGs were performed between the 7th and 10th day of the menstrual cycle. Water-soluble contrast media was introduced using a cannula placed in the cervical canal under aseptic conditions. Films were taken with the patient in the supine anteroposterior projection and oblique views were done when necessary. The Spot films demonstrated the cervical canal, uterine cavity, fallopian tubes and peritoneal spill. On average 10-15 mls of contrast medium were administered for each patient and in rare cases up to30 mls. RESULTS Demographic and clinical data: Two hundred eighty-nine (289) patients’ records were reviewed. The age ranged from 18 to 42 years with a mean age of 29 years as shown in table 1. Table 1: Age distribution of patients
One hundred sixteen patients had primary infertility while 173 had secondary infertility. All patients were of low parity ranging from 0 to 5; 16.7 % of them had had abortions before. Findings at hysterosalpingography
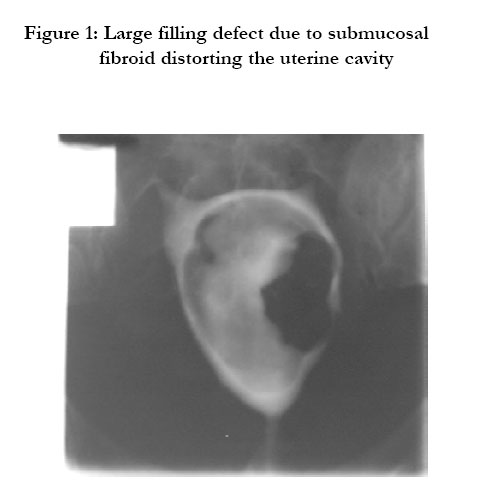
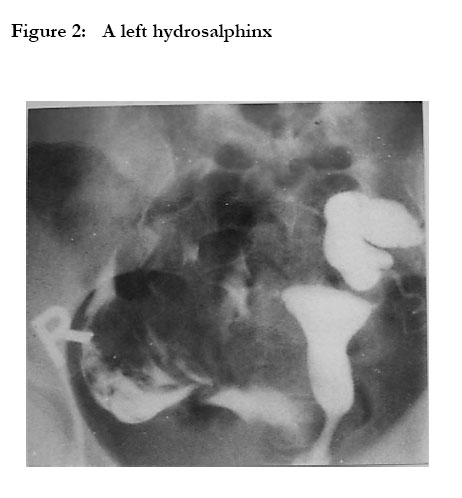
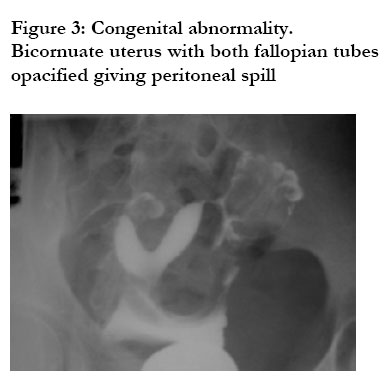
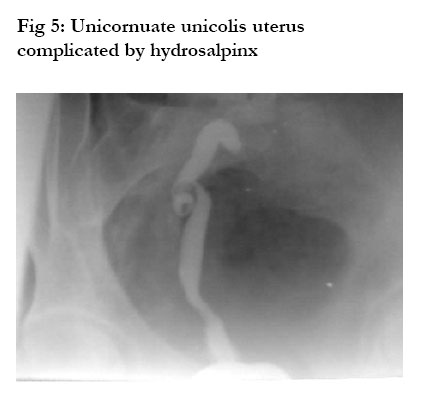
Normal findings at HSG were found in 16.6% of the patients. Uterine filling defects were seen in 18.3% of patients, these could have been due to uterine myomas, endometrial polyps or adhesions. The cervical canal was abnormal in 31.5% of the patients, reported as dilated or having filling defects. features suggestive of endosalphingitis were found in 17.3% of patients. bilateral tubal blockage was seen in 32.9% while 6% had unilateral tubal blockage. Only 4.2% had had surgical tubal ligation. Loculated spill was noted in 28% being bilateral in 24.4%. Fimbrial-end adhesions were found in 17.3% of patients. Hydrosalphinx were seen in 12.8% while 30% had signs of pelvic peritoneal adhesions. Congenital abnormalities were found in 1.6% of patients. DISCUSSION The main indication for HSG is infertility. The incidence of infertility, primary or secondary varies in different parts of the world. In this study, the incidence of secondary infertility was higher than that of primary infertility. This is similar to the finding by Obejide in Ibadan, Nigeria 3. However this differs from reports from other studies where it has been noted that primary infertility is commoner 3,4,5. The high rate of secondary infertility and the fact that there was a high rate of tubal related abnormalities could be due to post abortal sepsis and puerperal sepsis. This could be because of un-availability or inaccessibility of medical facilities so that many women deliver under poor sanitary conditions or have unsafe abortions and poorly managed spontaneous abortions. Tubal related factors were found in72.9% of the patients, which is similar to what was reported in Kenya5 and in Tanzania6. WHO reported that tubal occlusion and acquired tubal abnormalities accounted for 85% of infertility in Africa.7 This being a retrospective study the clinical data obtained was limited making it difficulty to establish if these patients had ever had pelvic inflammatory disease. The greatest number of patients fell under the age group of 25 – 29years. This is not surprising because its the peak of the female reproductive stage. Hysterosalpingography is still widely used in the investigation of infertility, recurrent abortions and for follow-up after tubal surgery. Other investigations such as sonohysterogrophy, laparascopy and hysteroscopy are being increasingly advocated for but not yet readily available in Uganda; thus HSG is still widely used. The infertility clinic in Mulago Hospital runs once a week and registers 20 – 30 patients a day of whom 50% are new patients. Most of these patients end up having an HSG. Though sonohysterography has been reported to be as sensitive as HSG in imaging uterine pathology, it has not yet been used in Uganda 8. Normal findings were seen in 16.6% indicating that the cause of their infertility was not physical. One thing to note is that many women with infertility are investigated without investigating their spouses so it could be that their spouses might be infertile. Most patients were found to have tubal related problems, most of these findings are thought to be secondary to pelvic inflammatory disease which indicates that pelvic inflammatory disease is still common in Uganda and is a common cause of infertility. A few patients had had tubal ligation and wanted it reversed. This suggests that they had not had proper counseling and guidance before the procedure. At both private clinics antispasmodics were not routinely used, this implying that some of the corneal tubal blockage could have been due to spasms. However even if this was so it would not reduce the number of patients with tubal blockage significantly. The commonest structural cause of infertility in Uganda as per this study is tubal blockage and is commoner inpatients with secondary infertility. Factors associated with this are not yet established and a study to elucidate them is recommended. REFERENCES
Copyright © 2004 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs04032f5.jpg] [hs04032f3.jpg] [hs04032f2.jpg] [hs04032f1.jpg] [hs04032t1.jpg] [hs04032f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}