 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
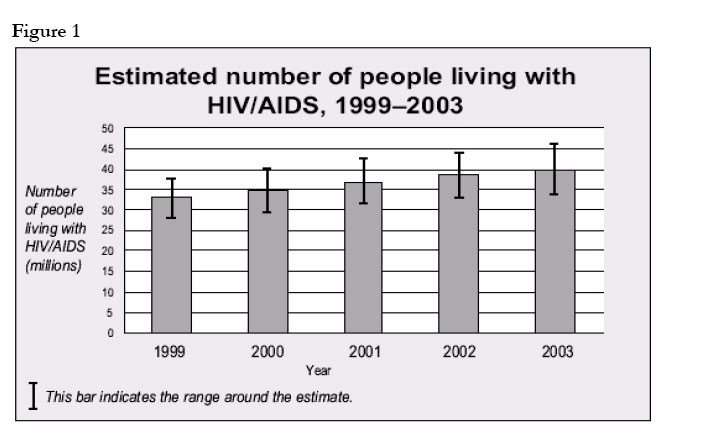
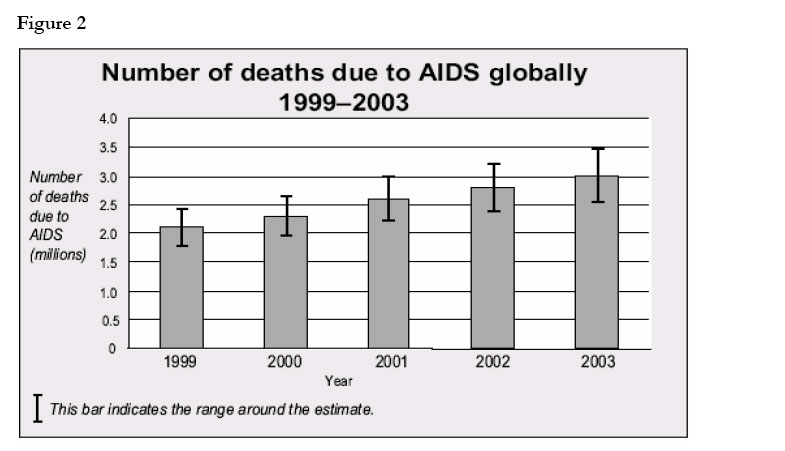
African Health Sciences, Vol. 4, No. 3, December, 2004, pp. 202-205 What’s in a label? Learning from the HIV-TB deadly symbiosis Rachel Klein* Tufts University, Community Health and Spanish Major, Columbia University Mailman School of Public Health, 50 Haven, Avenue, Box #266, Columbia University Code Number: hs04040 The World Health Organization (WHO) announced in September of 2003 that HIV / AIDS should be labeled “global health emergency” rather than just a pandemic. Might the severity of the label cause more harm than good? This essay attempts to tackle this question by considering what has been learnt from previous such declarations, specifically with respect to Tuberculosis, a close companion of HIV/AIDS. The label of “emergency” is necessary for any disease that fits the description; however, when two diseases are as closely linked as are HIV/AIDS and tuberculosis, shouldn’t the term be applied to them collectively? In 1981, shortly after the first reports of AIDS in the United States among gay men and injecting drug users, it became evident that the disease was also present among other populations. The identification of a variant of the virus, HIV-2, in African populations, further increased the heterogeneity of what quickly emerged as a “global pandemic” 1. A “pandemic” is defined as a widespread disease outbreak affecting the population of an extensive area of the world 2. The term “pandemic” was a necessary and advantageous step made by the CDC and the WHO to give HIV/ AIDS the public attention and both medical and humanitarian funding required to stem its advance. Two decades into its existence and despite concerted efforts and funding to combat the deadly virus, the HIV/AIDS pandemic has continued to worsen. “In two short decades, HIV/AIDS has become the premiere disease of mass destruction,” stated Dr. Jack Chow, the assistant director-general of WHO, and that “the death odometer is spinning at 8,000 lives a day and acceleratin”3 - see figures 1 and 2, for increasing trends in HIV/AIDS infections and deaths. It has been argued that, “International agencies have not placed sufficient priority on the prevention of HI V in complex emergencies… and the prevention of important, though less visible causes of morbidity and mortality (HIV and STD’ s) have not received adequate attention in populations affected by emergencies,,4. His bleak outlook and unpromising future prompted the WHO to amend the HIV/AIDS label from a pandemic to an emergency in the fall of 2003. A “complex humanitarian emergency” is defined as a “relatively acute situation that affects large civilian populations and usually involves a combination of war, food shortages and population displacement, all of which result in significant excess mortality”5. The WHO and other humanitarian aid agencies are hopeful that the “global emergency” label, combined with the additional spotlight and funding that accompany this heightened nomenclature, will help reduce and hopefully eliminate HIV / AIDS in the long run. In order to urgently address the emergency, the WHO6 is now committed to the “3 by 5” plan by setting out to provide lifesaving anti-retroviral therapy treatment to 3 million people in low resource countries by the end of the year 2005. Critics of the WHO’s optimistic outlook argue that handling and referring to HIV / AIDS as a solitary emergency is the root of the problem, simply because those infected with HIV experience a breakdown of their immune systems, leaving them extremely vulnerable and susceptible to many opportunistic infections. The most prevalent opportunistic infection observed among HIV-infected patients in low resource countries is tuberculosis. Tuberculosis (TB) kills approximately 2 million people each year, making it one of the world’s leading infectious disease causes of death among young people and adults. Due to a combination of economic decline, the breakdown of basic health care systems, insufficient application of TB control measures, the spread of HIV/AIDS, and the emergence of drug-resistant TB, it is on the rise in many developing and low resource countries? In 1993, the WHO took an unprecedented step and declared TB a “global emergency,” so great was the concern about the growing TB epidemic6. Since the WHO’s declaration in 1993, the TB emergency has regrettably grown much larger and funding has been “severely neglected’’7. Although TB treatment and prevention alone are relatively inexpensive, “affordable lifesaving health interventions for infectious diseases are neglected in favour of large and expensive projects” 6 such as the global AIDS emergency. If only efforts were made to combine and combat both HIV and TB together, there would be reason for optimism. Critics of the WHO’s optimistic outlook on curing the HIV/AIDS emergency alone argue that “the coming wave of mortality and epidemics worsened by HIV, including tuberculosis, will sooner or later force a change in policy, but we need to make it sooner rather than later”8. It has been widely acknowledged that “HIV and TB form a lethal combination, each, speeding the other’s progress” 6. HIV weakens the immune system and once infected with HIV, a person is many times more likely to become infected with TB than someone who is HIV-negative. TB is one of the leading cause of death for those who are HIV-positive and the highly contagious infections accounts for roughly 11 per cent of AIDS deaths worldwide7. A joint program, therefore, is a necessity because presently “although TB is one of the leading causes of death of people living with HIV/ AIDS, the relationship between HIV and TB is rarely addressed by the AIDS community6. The term “criminal neglect” ha s been used to describe the situation in Africa, in which millions of innocent lives are being lost unnecessarily despite the existence of joint, effective prevention strategies and life-saving treatments. Therefore, the deadly symbiosis of HI V and TB requires a massive joint effort at all levels in order to avert a possible disaster in the future. A combined effort among HIV and TB aid programs would be exemplary in proving that by working together toward a common goal, far greater results are possible. Such cooperation would be a positive example for those involved in remedying other epidemics and emergencies. “Analysing why and how a particular crisis attracts the donor attention, while another one remains outside the spotlight, can provide only partial answers. In fact, focusing only on one emergency, and overlooking the fact that some emergencies become noisy at the expense of others remaining silent, one risks not to see the wood for the trees. In our globalised world, crises are interconnected...9 It is apparent that the combination of TB and HIV will have a large impact on how both are viewed, treated, and funded in the future. At the Third Working Group Meeting of the TB/HIV in June of 2003, it was recognized that collaboration amongst the two is key, and the introduction of a TB/HIV “Working Group” can serve as a bridge between the two communities. “TB and HIV programmes must work together to accelerate an effective joint response to the epidemic of HIV -associated TB in all affected countries. . . We are dealing with two diseases, one patient, one community” 6. It was suggested that the following basic steps become standard global practice: all those newly diagnosed with HIV must be screened for TB and all those diagnosed with TB must be offered HIV testing and counseling. The TB/HIV programs are willing to help collaborate with the. WHO3" by 5" plan by being committed to the goal. TB and HIV collaboration has already begun in several low resource countries, such as South Africa, Malawi and Zambia. ProTEST, (Promoting HIV TESTing) which began in 1998, has demonstrated already that the TB/HIV partnership improves health services through capacity building and access to a wider range of preventive care services for people living with HIV and TB. As of June, 2003, ProTEST had helped to successfully avert more than 14,000 HIV infections7 The five key components that TB/HIV action plans should include are the establishment of a nationallevel TB/HIV coordination committee, the establishment of HIV surveillance among patients with TB, the option of HI V testing and counseling for all patients with TB, the establishment of screening for TB for all patients infected with HIV and, finally, the strengthening of HIV care and prevention with DOTS to combat and treat TB. DOTS is the WHO-recommended treatment strategy for detection and cure of TB. DOTS has proven to be a very effective treatment with cure rates up to 95 per cent and has been ranked by the World Bank as one of the “most cost-effective interventions” 6. Ten years after the WHO declared TB a “global emergency” in 1993, the WHO reported that over 10 million TB patients have been successfully treated under DOTS. Of those, more than 90% live in low resource countries where the disease causes the most suffering, economic instability and death. It is true that the growth incidence rate of TB has slowed to 0.4% per year; however the epidemic is still growing6. The Executive Director of UNAIDS, Dr. Peter Piot, was quoted as saying that “TB and HIV have become intertwined epidemics, increasing their devastating impact on communities world-wide” 6. The ProTEST projects have demonstrated “how TB and HIV workers can collaborate effectively to strengthen DOTS, to reduce the number of cases of HIV, to find cases of TB earlier and to provide preventive therapy” and have proved to be an “excellent platform” for the future. In conclusion, we must recognize that the language used to characterize global health issues has a major impact upon how these crucial, medical and social issues are handled, both nationally and internationally. One may argue that words are just words; however, nomenclature can and does affect actions and has proven to be a powerful force, producing change, beneficially and, at times, detrimentally. Farmer questions, “can declarations change the world?” and his response is: “they can if they lead to action commensurate with the problem”8. The “problem” we are facing with the worldwide spread of HIV and TB is one of dual nature, one that unless treated in a combined, constructive manner will continue to worsen. The first step in successfully combating the HIV/AIDS global health emergency is the recognition of its close link with TB, followed by building bridges of prevention and care between the two in order to bridge the existing gap and help rid the world of two of its most deadly diseases. REFERENCES
Copyright © 2004 - Makerere Medical School, Uganda
The following images related to this document are available:Photo images[hs04040f2.jpg] [hs04040f1.jpg] |
| |||||||||

{kind=link}
{kind=link}