 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 5, No. 1, March, 2005, pp. 4-13 ORIGINAL ARTICLES Promotion of handwashing as a measure of quality of care and prevention of hospital- acquired infections in Eritrea: the Keren study Rigbe Samuel1 , Astier M. Almedom2 , Giotom Hagos3 , Stephanie Albin2 , Alice Mutungi4 Correspondence to: Astier M. Almedom Tufts University, Boston, USA. astier-m.almedom@tufts.edu
Code Number: hs05003 ABSTRACTA complex interplay of cognitive, socio-economic and technical factors
may determine hand-washing practice among hospital- based health workers,
particularly doctors, regardless of the location of the country or hospital
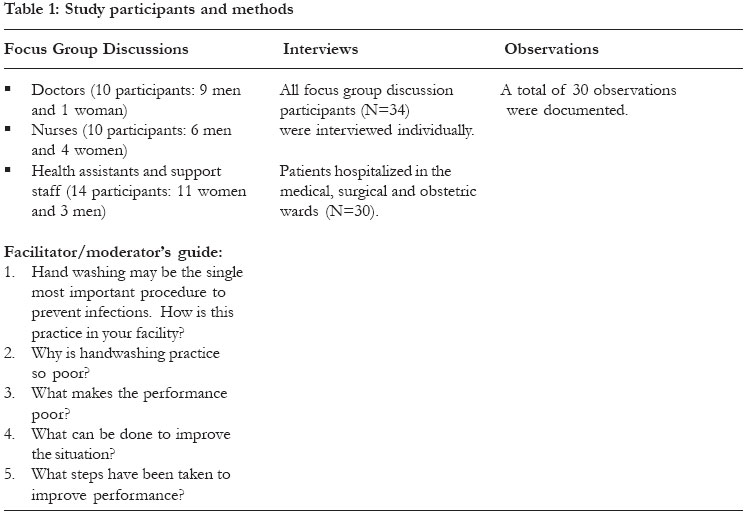
they work in. INTRODUCTION The Hungarian physician Ignác Fülöp Semmelweis (1818-1865) was first to demonstrate that the simple act of hand washing could save lives, especially when health workers do it routinely and thoroughly. Unfortunately, hospital acquired infections (HAI) continue to plague both western industrialized and non-western resource poor countries, often for lack of observance of this simple hygiene practice – but why? As a young doctor working in a small Vienna hospital, Semmelweis suspected a ‘cause and effect’ relationship between two observations of his own: one, doctors and medical students were going straight from the autopsy room to the delivery room to perform internal examinations on expectant mothers without washing their hands; and two, many of the women were dropping dead from puerperal fever caused by infection with Streptococcus pyogenes bacteria. Semmelweis’ seniors believed that “childbed fever” was caused by “ backlog of clotted breast milk”, when in actual fact the women were being infected by “cadaver particles” introduced by the doctors and medical students’ own hands.1 To prove his point, Semmelweis instated compulsory hand washing in choride solution for every medical attendant before they touched the women; and lo and behold, the rates of “childbed fever” and subsequent maternal mortality in that hospital fell dramatically. Unfortunately, Semmelweis’ superiors did not change their minds and reward him for his life saving discovery. His work remained unrecognized until long after his death; and his lessons still remain unheeded in hospitals around the world even today. 2-6 Doctors and other health workers put themselves and their patients in danger when they fail to observe routine hygiene practices. Among the deadliest pathogens encountered in hospitals are methicillin-resistant Staphylococcus aurens (MRSA), multi-resistant strains of Klebsiella and Pseudomonas4,7, respiratory syncytial virus (RSV) which poses very high risk to sick infants and young children in intensive care units (ICU) as well as to the health workers attending to them8; acinetobacter baumannii infections that are prevalent in adult and general ICUs9; as well as more recently discovered viral infections such as SARS.10 Such infections can invade the skin, urinary tract, lower respiratory tract, and surgical wounds.11-13 As was the case in Semmelweis’ lifetime, promotion of the simple, effective and inexpensive practice of handwashing continues to be hindered by ignorance, arrogance and/or carelessness on the part of health workers, however high ranking, educated and skilled. Infection prevention guidelines are issued, re-issued, revised and updated regularly; and cognitive (educational and empowering), technical (step-by-step practical training on how to wash hands) and novel ideas of incentives and rewards for health workers are repeatedly put forward,7,14-24 and yet the problem remains unsolved. Reportedly among the worst offenders are doctors working in ICUs, emergency departments (ED), and post anesthesia care units (PACU) where patients are most vulnerable.25,26 At least one self-report of a modern-day doctor in an English hospital obstetrics and gynaecology unit admitting to this offence and trying to justify it in terms of lack of time and belief that hand washing has little or no value27 also generated heated debate in the electronic “Rapid Response” forum of the British Medical Journal initiated by the “Handwashing Liaison Group’s” editorial.5 However, it is important to note that a great many highly qualified and skilled hospital doctors, nurses and other health workers do work hard to prevent and control HAI, despite the constant constraints of time and other resources (human and material) in both rich and poor countries. Nevertheless the question remains: how can we prevent and control (if not eradicate) avoidable fatal infections acquired in the very places where our patients go to regain their health, and not to be maimed or killed? Attitudinal and behavioural problems are often at issue, more than the lack of material resources, education or knowledge per se. Research evidence suggests that some health workers are worse than others in this regard: while registered nurses and nurse practitioners who generally have more contact with patients champion the cause of infection prevention by washing their hands thoroughly between patient contact, physicians and specialist consultants often fail to do the same, setting a bad example for younger doctors and medical students.25, 28 Regardless of the methodological and analytical difficulties surrounding the interpretation of comparative data, nosocomial infection rates are generally likely to be higher in teaching hospitals, compared to non-teaching ones. Moreover, the evidence is inconclusive as to whether technical intervention or education and feedback work best -both activities are often required.18,28 Genuine human error and real (or perceived) limitations of time aside, concern over the effect of detergents on the hands has been an issue as well. Several studies have investigated the acceptability and/or effectiveness of waterless alcohol-based gels and hand rubs in comparison with hand washing with antiseptic soap29-32 and the results show that alcohol-based hand rubs combined with either an antibacterial or a plain lotion soap may be both effective and kinder to the skin29, or just more popular, resulting in increased rates of hand cleansing.32 It is worth bearing in mind that some of these studies have declared funding support from the manufacturers of the hand gels and lotions in question29,30 and so their evidence may serve the interests of stakeholders other than hospital patients and health workers. An earlier study (conducted over 25 years ago) had demonstrated clearly that simple hand washing with running water and soap draws bacteria from deeper layers of the skin, even after alcohol rubs had already been used to disinfect the hands.33 However, there is also real concern among health workers about the risk of dermatitis caused by frequent washing of hands with harsh detergents, so there is clearly more to hand washing than Semmelweis first noted. This paper hypothesizes that a complex interplay of cognitive, socio-economic and technical factors may determine hand-washing practice among hospital-based health workers, particularly doctors, regardless of the location of the country or hospital they work in. Furthermore, high-level political will and attention to the quality of health care, coupled with adequate provision of supplies and practical training to motivate health workers may achieve significantly positive results, where prestigious formal education and handsome salaries alone prove to be insufficient. We report on the first study designed to assess quality of care with respect to hand washing practice as a routine measure of infection prevention in Eritrea, the youngest African country making strides in post-war recovery of quality in national health care provision. Health Policy ContextEritrean health policy and practice has a long tradition of responsive planning and effective implementation of service delivery under dire conditions of protracted war. Historically, the system has been progressive: inclusive, equitable and accountable, with highly motivated health workers across the broad range of primary and secondary health care.34, 35 Less than five years after the country’s formal independence, the Eritrean government Ministry of Health (MOH) initiated a quality assurance program (1997) as part of the development and implementation of the national primary health care policy.36 Assessment of quality of service provided by all hospitals was conducted, and a set of quality standards were developed and approved in the year 2000. Infection prevention was identified as a priority area, and all hospitals were requested to establish their own infection control committee (IPC) in order to develop and test appropriate quality assessment and improvement process for infection prevention tailored to their specific sites.37 The present study was conducted to examine the feasibility of adherence to quality standards once established, with particular reference to routine hand washing practice as a measure of infection prevention. Study site, participants, and methods Keren hospital, the second largest in Eritrea, was selected for this study as a representative of provincial referral hospitals for which baseline data could be gathered for the purposes of developing standards and procedures for quality assessment and improvement in infection control nationally. The hospital is located in Keren, capital city of Zoba Anseba, one of the six Eritrean provinces. It is thus a provincial/zonal referral hospital, and has the capacity of 100 beds, and 142 health workers of whom 10 are doctors, 37 nurses, and the rest are health assistants and other support staff. Keren hospital’s catchment area includes 428 villages, a total of approximately 334, 862 inhabitants, the majority of whom subsist on agriculture, combining transhumant and pastoralist modes of livelihoods. The climate and terrain of Zoba Anseba encompasses mid and high altitude regions ranging from 600 to 2040 meters above sea level. The study team comprised the first author (principal investigator) and five nurses (research assistants) in Keren hospital who were trained over an intensive period of three days, in observation and interviewing methods, contributing to subsequent modifications of the interview guide/questionnaire used. A total of 34 health workers including doctors, nurses, health assistants and other support staff working in Keren Hospital; and 37 in-patients participated in this study –see Table. Participants joined the study on a voluntary basis. Information about the purpose of the study was given to both the hospital health workers and patients verbally, and verbal consent was obtained from those who participated. No incentives and/or rewards in cash or in kind were offered to the study participants. Focus group discussion facilitators, a doctor, an administrator and a head nurse from within Keren hospital were trained by the first author (principal investigator) and her advisor (third author) and given a set of five questions (listed in Table 1) to guide their group discussions. All three focus group discussions were conducted in Tigrinya and were tape-recorded. Doctors and nurses formed two separate focus group discussion groups, while health assistants/ associate nurses, lab technicians and a pharmacist formed the third group. All three groups were mixed in terms of gender: two groups had majority men and the third had majority women – Table 1. Direct observations of existing hospital hand washing facilities were conducted using standard check-lists prior to the intervention and observations of health workers’ hand washing practice were conducted by the principal investigator during weekly facilitative supervision and coaching visits to the hospital – see ‘Intervention’ section below. These weekly visits were conducted upon the recommendation of the participants of a one-day data interpretation workshop conducted after the first phase of this study. Semi-structured interviews were conducted individually with the 34 health workers who participated in focus group discussions, and with 30 consenting hospital patients (and in the case of child patients, with their adult carers) in the medical, surgical and obstetric wards. The study design and methods provided a robust system of data quality check through triangulation of information by sources and methods, as is established practice in health/hygiene research.38 Intervention
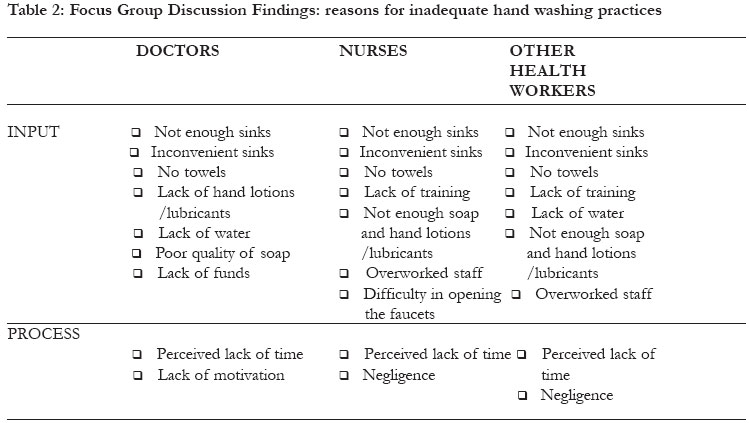
During the initial assessment, it was found that barriers to handwashing included lack of clean towels (staff shared a common cloth towel) and soap. The sinks were located in the nursing station, which was considered inconvenient for the staff. Therefore, health workers were provided with individual hand towels and soap. A portable water tap for hand washing was placed in each ward. In addition, in-service training was provided to all hospital personnel including doctors, nurses, laboratory assistants, pharmacists, cleaning, kitchen, and laundry staff, as well as security guards. Everyone was trained to observe basic hygiene precautions including hand washing at critical times, use of gloves, disposal of sharp objects, and decontamination. Facilitative supervision and coaching visits were made every week for a total of 10 consecutive weeks. Each visit lasted 6 hours on average. Immediate feedback was given and correct hand-washing practice demonstrated whenever requested. A multidisciplinary infection prevention committee was initiated. Post-interventionParticipating health workers were given a pre and post intervention test comprising multiple-choice questions about infection prevention practices. The tests were administered in English to all training participants with the exception of some cleaners and security guards who were not literate in English. The first trainer/first author graded all tests. Post-intervention patient satisfaction interviews (N=37) were conducted by members of the study team over the course of 10 weeks from September to November 2001. The purpose of the revisit (postintervention) study was for the principal investigator to provide more supportive training and follow-up on the issues raised by the study, as requested and recommended by the data interpretation workshop participants. Results Observations of hospital facilities revealed that all wards had running water, 60% had functioning and conveniently located sinks. Ninety five percent of the sinks had good drainage and functioned well even if the location of some was inconvenient. All observed health workers’ washed their hands after contact with blood, body fluids or contaminated objects. Seventy two percent washed their hands for 10-15 seconds and 30% washed their hands thoroughly, rubbing between fingers and around nails. Only 30% of health workers routinely washed their hands between patient contact. The rest used gloves. In their focus group discussion, most doctors admitted that they did not wash their hands between patient contact. Various reasons were mentioned: lack of adequate and conveniently located sinks, lack of adequate hand towels, lack of water, poor quality soap, lack of hand lotions/lubricants for use after hand washing, and lack of time – see Table 2. When asked to propose solutions to the problem of inadequate levels of hand washing, doctors, nurses and other health workers who participated in the focus group discussions suggested that staff training and sufficient supplies where necessary; that mechanisms for continuous supervision and follow-up should be put in place; and that good practices should be rewarded – Table 2. The interview results concurred with the focus group discussion findings. Fifty percent of the health workers interviewed said that they prefer to wear gloves, and admitted that they do not change their gloves between patient contacts. Those who preferred gloves saw them as protective devices for themselves, rather than for their patients. These same health workers considered hand washing to be time consuming. Some said that the reason they did not wash their hands was because they did not like to use common towels to dry their hands after washing. These findings were disseminated among the study participants and other health workers who attended the one-day data interpretation workshop. 71 participants including members of the hospital management team attended this participatory workshop aimed at engaging everyone in problem solving. Workshop participants agreed that the hospital facilities were in fact adequate for hand washing, and so the reasons for the observed and reported lack of hand washing may have been more associated with inadequate training in infection prevention. It was also agreed that regular and sufficient supplies of protective materials including cleaning agents, facilitative supervision and follow-up were necessary ingredients of success in implementing prevention of HAI. The workshop ended with the formation of a new IPC for Keren hospital comprising of the hospital medical director, surgeons, gynaecologists and obstetricians, hospital matron, pediatrician, operating room nurses, surgical and laboratory technicians, pharmacist and laundry staff. The post intervention test results showed that health workers’ knowledge about infection prevention practice had improved significantly – there was a 25% rise in post intervention scores when compared with preintervention. Marked improvement in compliance with infection prevention standards were noted with respect to hand washing after removing gloves (from 76% pre to 100% post intervention), cleaning beds and bedside equipments with disinfectant (from 12% pre to 87% post intervention), changing masks and oxygen catheters and tubes between patients (from 26% pre to 80% post intervention), and availability of isolation rooms for infectious patients (from 24% pre to 90% post intervention). Patient Satisfaction The most important finding was the increase in patients reporting that they observed health workers wash their hands between patient contact (from 20% pre to 60% post intervention). When asked for their suggestions for health service and care improvement in Keren hospital, patients recommended the following: health education for patients and their relatives; continuous supervision of hospital staff; maintenance and repair of blocked toilets; teaching health workers to be conscientious and to respect the patients; provision of psychological/moral support for patients, particularly for women in labor. Finally, observation of hospital facilities post-intervention showed that all wards were provided with sterilizing equipment, disinfectants, soap, towels and buckets. Cleaners were also observed using their own individual towels. It was noted that provision of supplies resulted in improved hand washing practice by 40% among health workers in Keren hospital as a direct outcome of this study. DISCUSSIONReminders of the importance of hand washing as a simple and effective means of preventing the spread of infection abound. For example, in Boston (USA), National Public Radio announcements around Christmas Eve include reminders for priests to wash their hands thoroughly before they handle communion bread, in order to prevent the spread of seasonal infections, particularly influenza. Similarly, in the Far East, public health advice concerning the latest outbreaks of viral infections such as SARS have pointed the lay person in the direction of the simple practice of handwashing with soap and water, especially in children’s day care centers, pre-schools, schools, shopping malls and other public places. Hospital nurses, doctors and consultants are rarely mentioned in public as likely vehicles of the spread of infection in health care settings; and yet they are, if they fail to wash their hands routinely and thoroughly. In the USA, patients are advised to demand that their doctors wash their hands before they touch them. However, such advice is not very practical for those in ICUs hitched to ventilators, intra-venous drips and catheters; or those who are under anesthetics undergoing surgery or otherwise unconscious. Dissemination of infection prevention information and advice concerning HAI is probably best carried out in the community, away from hospitals, so that lay people can prepare themselves for hospitalization well in advance. To this effect, a renowned University Professor (Elaine Larson) was pictured in her laboratory with her microscope and test tubes in a fairly recent issue of the glossy magazine PEOPLE, with a caption that read “Nobody washes their hands enough”. This included five tips under “Patients’ Best Defense” – see Box. So, can hospital patients in western countries take legal recourse for HAI? Anecdotal evidence suggests that at least some relatives of deceased patients do, but may not succeed in establishing the cause of death beyond reasonable doubt.39 In the case of Eritrea, patient protection and infection prevention policy and practice have started on the right foot, bearing the legacy of veteran health workers’ motivation and dedication to compassion and not just competence. Ironically, this can be more of a challenge at peace time than it was at war time; but it is by no means insurmountable. The findings of this study make two major contributions to the literature on nosocomial infection prevention. Firstly, the study confirms that both cognitive and technical input are necessary for infection prevention - it is not an ‘either-or’ proposition. Promotion of hand washing is also relevant to clinics and health stations which do not accommodate in-patients. A study conducted in Belgium has shown that General Practitioners’ hand washing practice left more to be desired, highlighting the need to target them as well.40 However, the point of international comparison is not to encourage complacency among Eritrean (and other African) doctors. The view that “even rich countries have this problem, so why bother?” needs to be tackled head on. In Eritrea, the challenge is to at least maintain previously documented and celebrated standards of cleanliness and patient care; if not to excel. Can doctors who can’t be bothered to wash their hands get away with using gloves? In the case of Keren hospital, doctors’ preference to use gloves, and their failure to change them between patient contact seemed to be indicative of two basic misconceptions: one, that gloves are meant to protect the doctor, and not the patient; and two, that repeated use of the same pair of gloves does not matter to either the doctor, the patient, or for both. Studies have shown the use of gloves to be hazardous for both patient and health worker unless certain precautions are taken. Latex gloves can easily get punctured and/or provide ambient medium (moisture and warmth) for bacteria to breed rapidly. Washing hands and donning them with antimicrobial substances before gloving (particularly for unsterile vinyl gloves) and washing hands immediately after removing the gloves (even when using sterile gloves) is recommended41, but much depends on the particulars of the hospital unit concerned. In one study involving nurses in a teaching hospital ICU, no significant differences were found between antiseptic hand washing and the use of nonsterile gloves over washed hands; or between the use of antiseptic donning technique, prior antiseptic hand washing and the use of individually packaged sterile gloves.42 Unmentioned by the authors, this may be more a reflection of nurses’perfection of the art of hand washing than the relative merits of sterile or non-sterile gloves versus hand washing. While the majority (72%) of Keren hospital health workers were observed washing their hands for 10-15 seconds, only 30% washed their hands thoroughly. Other studies have shown that many operating room nurses wash their hands for as short as half the recommended time of 5 minutes for surgical nurses43, but the technique used is clearly more important than the amount of time spent washing hands. Secondly, this study’s major contribution in the area of patient participation is important. A recent systematic review has highlighted the significance of patient involvement in quality of health care and service planning and improvement in the UK.44 The review concluded that “the effects of involving patients were likely to be complex, affecting different aspects of services in different ways. The views of patients are among many factors that influence change in health services, and providers of health care remain the final arbiter of how much weight is attached to patients’ views.” (p. 1267) This may hold true for Eritrea as well, although the Eritrean health service does not easily lend itself to simple categorization by political orientation. According to Gill Walt’s careful analysis, so-called “Egalitarian-authoritarian” systems such as those of Cuba and China have been characterized by resource redistributive policy and practice, often with positive health effects such as declines in infant mortality.45 Eritrea shows a similar trend,46 however, the findings of this study concerning patients’ views deserve careful consideration. Improvements in hand washing practice and general cleanliness of beds and disinfecting of the equipment and surroundings of patients’ beds in the post-intervention phase of this study are praiseworthy. Patients’ voices definitely carry more weight in this regard as health workers may be expected to over-report good practice. This study had controlled for such bias through triangulation: by using multiple sources and methods of data collection; and participant involvement in the interpretation of research findings. Health workers’ training in infection prevention needs to incorporate their own protection as well. With particular reference to autopsy units, the use of gloves, even double layers and strong gauntlets for the nondominant hand are recommended.47 Health workers may also protect themselves with gloves from the hazards of ingesting deadly pathogens while reading and licking their fingers in order to turn the pages of hospital patient records.48 However, the most important lesson seems to be, doctors: avoid treating gloves as protective devices against your patients. The costs of HAI transmitted by contaminated gloves and hands are enormous for the patient – literally a matter of life and death – and they are also costly to the hospital, the Ministry of Health and to the country as a whole as increased morbidity and mortality means loss of human, social, and economic capital. One study has documented the cost-effectiveness of simple preventive strategies such as health workers’ proper washing and scrubbing of hands to prevent and control nosocomial infections.49 This is relevant to Eritrea and to other countries in similar stages of post-conflict reconstruction and health policy and practice improvement. Finally, the patients’ observations and suggestions concerning health workers’ attitude and behavior is worth discussing. The concerns of hospital patients and their relatives, particularly women in labor, point to the need for training in communications and patient care. Pregnant and newly delivered mothers constitute an important section of any population’s vulnerable groups. In the Eritrean psyche, mothers and motherhood are sacred across the religious, socio-economic, ethnic and cultural spectrum. Women have borne the brunt of hardship wrought by war. Lack of basic respect, if not moral support to women in labor on the part of health workers who happen to abuse their ‘power’ over life and death is therefore both repugnant and intolerable to the Eritrean people, be they rural agro-pastoralists of humble means or urban well-to-do citizens. The quality of maternity health care service provision will remain a litmus test for the level of progress in health care policy and practice in post conflict Eritrea; and health workers entrusted with the care of women in childbirth have a very important role to role to play.50 An important strength of this study is its participatory and experimental design which has served to engage hospital-based health workers from all levels of service in problem solving activities and processes. Such studies are iterative and dynamic, rather than linear and static. Thus, the formation of an IPC for Keren hospital representing stakeholders who are inclined to take it upon themselves to raise the standards of quality of health care as they develop a stronger knowledge base of infection prevention and the necessary skills to implement agreed procedures, is a logical outcome of the study. There are indications of positive and dynamic change as health workers are motivated and empowered to work in partnership amongst themselves and with their patients, traditional birth attendants and relatives who may accompany the patients to the hospital and help with their care. This will require sustained high-level commitment and political will to allocate the necessary resources to improve quality of health care services in the country. This study is yet to be replicated in other zonal referral hospitals in the country where both cognitive and technical capacity for infection prevention may be different from those of Keren hospital. The study design and methods are robust and replicable, paving the way for more such studies to be conducted in order to build a strong, reliable and useful evidence-base for policy and practice concerning nosocomial infections that may be applicable to other countries in similar stages of post-war reconstruction and rehabilitation of health services in Africa. CONCLUSION Prevention and control of HAI remain major priorities for Eritrea and other countries around the world. It can effectively be advanced through the simple and inexpensive hygiene practice of proper handwashing between patient contact by doctors, nurses, health assistants and other support staff. Whatever their reason for failing to wash their hands at critical times, health workers who spread HAI stand guilty of violating the Hippocratic Oath, Do No Harm, that is sacred to their profession, and should therefore be made accountable in the most appropriate way. Rewarding good practice may be a useful step forward, however, ultimately, only the doctors (and nurses and other health workers) individual as well as collective motivation, sense of professional integrity, and pride in their own work can galvanize collective efficacy and accountability. ACKNOWLEDGEMENTS We thank the study team and participants in Keren hospital; the facilitators and instructors of the Institute of Public Health at Makerere University; Minister of Health, Saleh Meky; Director of Clinical Ser vices, Dr Michael Gebrehiwet; Sister Kidisty Habte and Dr Dan Wendo (TASC); Dr Berhane Debru; Dr Leul Banteyinga; and Joanne Ashton. Funding support for literature review and preparation of this manuscript was generously provided by Tufts University’s Henry R. Luce program. REFERENCES
Copyright © 2005 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs05003t2.jpg] [hs05003t1.jpg] |
| |||||||||

{kind=link}
{kind=link}