 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 5, No. 1, March, 2005, pp. 50-54 Clinical presentation and management of alleged sexually assaulted females at Mulago hospital, Kampala, Uganda Samuel Ononge1, Julius Wandabwa2, Paul Kiondo2, Robert Busingye1
Corresponding Address: Paul Kiondo, Makerere University, Faculty of Medicine, Department of obstetrics and Gynaecology, P.O.Box 7072 Kampala. E-mail:kiondop@yahoo.com Code Number: hs05009 ABSTRACT Objective: To determine the presentation and treatment offered to sexually assaulted females attending emergency gynaecological ward in Mulago Hospital, Kampala, Uganda African Health Sciences 2005; 5(1): 50-54 INTRODUCTION Sexual assault is defined as any genital, oral or anal penetration by a part of the accused’s body or by an object using force or without the victim’s consent. Rape is defined as forced vaginal penetration of a woman by a male assailant. The two terms, rape and sexual assault have been used interchangeably in many countries, however many favour the concept of sexual assault because it is a gender neutral term. The magnitude of sexual assault world over is unknown. However well designed studies indicate that 7 to 18 percent of females have been raped. 1,2,3,4 Sexual assault accounts for approximately 7% of violent crime.2 In Transvaal Memorial Institute, Villiers and Prentice reviewed all the records of cases that presented to the child abuse and neglect clinic from May 1988 to April 1989. Of the 227 cases encountered in one year, 80% were females and sexual abuse was the complaint in 89.8% of the cases.5 In Uganda, the extent of sexual assault is unknown. A qualitative study on sexual abuse in Uganda was carried out to find out the knowledge, attitude and extent of sexual abuse in Kampala peri-urban area among the adolescents. The study found most groups were aware of sexual abuse, and the circumstances that lead to sexual abuse and the most venerable groups were children and orphans.6 All females of all age groups are at risk of sexual assault but the most vulnerable are the adolescents, children and the physically and mentally handicapped.6,7,8,9,10 In contrast, a retrospective study from the Agakhan Hospital Kenya showed that out of the 37 victims, 89.2% were between the age of 19-30 years and only 2.7% below 18years.11 The perpetrators of sexual assault (assailant) range from a person close to the victim like a relative, a neighbour, a friend, schoolmate, teacher, caregiver, husband or guardian to a stranger.12 The incidence of gang rape was noted to be high during the war situation and this was done to girls and women of all age groups.13 Sexual assault is usually associated with physical trauma such as injuries in the genital area or extra genital areas or both, but in the majority of cases one may not find any signs of physical injuries. In a study in Nigeria physical injury was present in 33% of the alleged rape victims and genital injuries were present in 30% of all alleged rape victims. Sexually assaulted victims are also at a risk of contracting sexually transmitted infections and as a general rule, the isolation of exogenous sexually transmitted organisms, such as Neisseria gonorrhoea, Chlamydia trachomatis, Trichomonas vaginalis, or the diagnosis of genital warts, genital herpes, or syphilis in a child who has had no previous voluntary sexual activity suggests the likelihood of sexual abuse.14 Although theoretically the risk of HIV transmission during rape is presumed to be very low, victims none the less are fearful.15 Sexual assault in Uganda has been mostly highlighted by newspapers and no study has been done to describe the magnitude, presentation and treatment of the survivors and yet this is becoming a common gynaecological condition with legal implications. The major objective of this study was to determine the magnitude, presentation and management given to victims of sexual assault in Mulago hospital emergency gynaecological ward. MATERIALS AND METHODS Design: This was a prospective descriptive study. Setting: Mulago hospital emergency gynaecological ward Study population: Females who were admitted at Mulago hospital gynaecological emergency unit. Sample size calculation: The sample size was obtained using a formula by Kish and Leisie. We used the prevalence of sexual assault in Dar es salaam of 14%9. The calculated sample size was 58 and this had a power of 80% to detect a risk ratio of two at the level of 5% of significance. Data collection: All patients with alleged sexual assault who had come for treatment and met the following inclusion criteria were recruited. The inclusion criteria were: all patients who had sexual assault and came for treatment and consented to participate in the study. Eligible patients were consecutively recruited until the sample size of 58 was achieved. The patients were interviewed using a questionnaire which was partially coded and also had open and close ended questions. The patients were asked about their socio demographic characteristics, relationship with the assailant and the location where sexual assault took place and the time. A physical examination was carried out for extra and genital injuries, and a speculum was inserted into the vagina where possible for high vaginal swab but where not possible a swab was taken from the lower third of vagina. The specimens were sent to the laboratory for a wet mount microscopy for Trichomonas vaginalis and evidence of sperms, gram staining and culture. Blood was taken for VDRL test for syphilis and HIV screening. If the victim was in her reproductive age, urine was taken for a pregnancy test to exclude the pre-existing pregnancy before the assault. The victims were given appropriate treatment. All the survivors received pre-test counselling for the HIV test by trained counsellors on HIV/AIDS before the blood was withdrawn for screening. The survivor or guardian received post test counselling before the results were given to the survivor or the guardian. All the survivors were discharged through Hope after Rape counselling Centre. They were given appointment for review at 3 weeks and 3 months. At 3 months the subject had another VDRL check and advised to come for another HIV test after another three months. The data collected was entered into a database using EPIINFO 6.4 statistical package, cleaned and analysed with the assistance of a statistician. Tests of significance were done using the chi squared test and presented using percentages and risk ratios with 95% confidence interval. RESULTSAge distribution of the survivors of sexual assault. The ages of the survivors of sexual assault are shown in table 1. There were fifty eight survivors of sexual assault recruited and all survived death. The age ranges of survivors were one to thirty five years with a mean age of 9.5 years and mode of 7 years. The majority (56.9%) of the survivors were in lower primary and pre-school going age. Site or location where sexual assault occurred and relationship between the assailants of sexual assault and the survivors. Table I: Age distribution of survivors seen at Mulago
The site or location where the sexual assault occurred and the relation ship between assailants and survivor are shown in table 2. Twenty six percent of the sexual assault cases took place at survivors’ home while half (50%) took place at assailants’ home with 58.6% of the assaults taking place during the day. In 46(79.3%) cases, the survivor was previously acquainted with her assailant. Relatives were involved in 30.9% and strangers were involved in 20.7% of the cases. Gang rape occurred in 4 (6.9%) of the cases and these were all strangers. In 10% of all the cases, the assailants were reported to have taken alcohol. Two survivors had also taken alcohol at the time of assault The time interval between the assault and being attended in Hospital varied widely from 3 hours to over a month. Only 16 (27.6%) of the survivors presented within 24 hours. The majority (72.4%) presented after 24 hours because they developed a vaginal discharge or were referred by the police. Table II: Site or location where sexual assault occurred and the relation ship between the assailants of sexual assault and survivor seen in Mulago hospital:
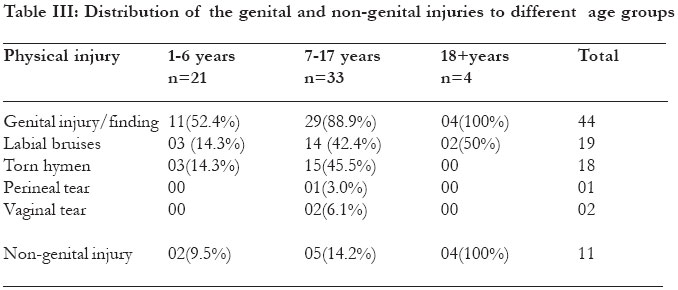
Distribution of genital and non genital injuries by different age groupsThe distribution of injuries are shown in table 3. The commonest genital injury was bruises or tears in the vulva. Fresh laceration of the hymen was present in 18(31%) of the survivors. One of the subjects sustained a second degree perineal tear. Most genital injuries were visible in the age group 7-17 years. Extra genital injuries were seen in only four adults. Eleven (19%) of the victims had both extra genital and genital injuries but 33(56.9%) of victims had genital injuries only. Laboratory investigations done Fifty four cases had high vaginal swabs for microscopy, culture and sensitivity examinations. One adult survivor had both trichomonas vaginalis and candidiasis. In another adult survivor had dead spermatozoa at microscopy. No Nisseria gonorrhoea organisms were observed on gram staining and culture. Most cultures grew Beta haemolytic streptococci bacteria. There were no facilities to test for Chlamydia trachomatis. Of the 55 cases, 4(7.3%) were HIV positive prior to sexual assault.(One was an adult aged 35 years and the rest were children under 6 years). Fifty one (92.7%) cases tested HIV negative. Only twelve out of the 55 cases came back for review at 3 months and all of them tested negative for HIV, but were advised to come back for another test after three months. Of the 55 cases tested for syphilis, only 2(3.7%) had a reactive VDRL. Therapeutic interventions offeredAll the survivors received counselling on sexual assault and all of them were later referred to Hope after rape counselling centre for further rehabilitation. All the 16 women who came for review, reported to have been to the counselling centre. None of the subjects received HIV prophylaxis because was not available. However 7 of the subjects in the reproductive age group were offered combined oral contraceptive pills as emergency contraception. T w o (4.6%) of the cases with genital injuries had their injuries repaired in theatre under general anaesthesia. One was a second degree tear in a 9 year old girl. The majority (87.9%) of the cases were given amoxicillin for treatment of various injuries and protection from sexually transmitted infections. DISCUSSION:Sexual assault is a crime of violence that puts the victim at risk for physical injury, emotional disturbance, pregnancy and sexually transmitted diseases. The majority (72.4%) of the victims of sexual assault were children below 12 years, with mean age of 9.5 years. This was comparable to studies from Australia 9, 10,12 but different from the Agakhan Hospital in Kenya study where the majority(89.2%) of the victims were between 1930 years.11 The difference could have been because of the affluent class of people attended this hospital. The higher number of children in these studies does not mean that this crime is less frequent in the older age groups but the scare of HIV infection is thought to be a major contributing factor to the increase in sexual assaults of young girls, who are considered to be relatively free of infection.17 However the feeling of anxiety, guilt and shame associated with sexual assault may prevent the victim of the older age group from reporting for medical treatment. A big number of sexual assault victims do not report the incidents because of the social stigma associated with it. The majority (79.3%) of the victims knew their assailants and 32.6% were relatives. Strangers were reported in 20.7% of the cases. Similar findings have been reported in some studies. 12 Some of the victims had been left with the assailant (e.g. househelp or relative) when the parents went to work. The acquaintance to the assailant increases the vulnerability especially of the young girls. In this study 50% of the assaults occurred at the assailant’s residence. This could have been because the victim knew the assailant and she did not suspect a person she knew could have such a motive. Gang rape involving multiple assailants is particularly a horrifying and a humiliating experience for the victim. It occurred in 6.9% of the victims in this study. The incidence of gang rape tends to be high during wars. 13 Genital injuries in this study were sustained by the young age group, especially those between 7 -17 years. This was similar to studies from Nigeria,10 USA2 and Malawi.16 In addition to physical trauma, the survivors of sexual assault suffer from psychological trauma. In this study, 10% of the cases were depressed and 8.6% of the cases were sobbing. These symptoms were observed in the adolescents and adult victims. In subjects where a high vaginal swab was taken, 1.9% had Trichomonas vaginalis and candidiasis and this was similar to most studies that found the incidence of Trichomonas vaginalis between 0-19% among patients tested.17,18 The study didn’t find gonorrhoea among the victims but most studies have reported the incidence to be between 0-26.3%.17,19 The reason for our study not having gonorrhoea was not clear but the survivors could have taken prophylactic antibiotics before the investigation were done. The reason for antibiotics cannot be strong when 3.7% of the cases had syphilis at first presentation. The HIV test was positive in 7.3% of the survivors at first presentation. However of the 12 cases that turned for follow up at 3 months, none had sero-converted and we recommended another test after another three months to confirm. Antiretroviral drugs were not given because they were not available in the hospital at the time. It is now recommended that HIV post exposure therapy be given to all sexual assault victims with antiretroviral agents. Though pregnancy is a possible complication of sexual assault in those in reproductive age group, it was not possible to observe this in our study because follow up was short. Only 43.8% of the victims in the reproductive age group were offered emergency contraception because they were able to come to hospital within 72 hours. All the survivors of sexual assault were offered counselling on sexual assault and later referred to Hope After Rape counselling centre for further rehabilitation by the psychiatrists and counsellors. For the minors, the counselling was directed more to the parents and guardians since they too were traumatised. Antibiotic treatment was offered to 87.9% of the survivors of sexual assault for prevention and treatment of sexually transmitted infection. This was in agreement with experts who suggest routine preventive antibiotic therapy. 21 CONCLUSION:Sexual assault is one of the most dehumanising crimes against women. It is associated with adverse medical and social problems in the society. There is urgent need to sensitize community to report for proper medical examination and treatment within 24 hours of a sexual assault. Anti retroviral drugs should be offered to all survivors. ACKNOWLEDGEMENTTo Gideon Kikampikaho, the Deputy Director of Mulago hospital for permission to publish the work; Prof. F. Mirembe and staff of gynaecology ward; and M. Ssekisolo for secretarial services. REFERENCES
Copyright © 2005 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs05009t2.jpg] [hs05009t3.jpg] [hs05009t1.jpg] |
| |||||||||

{kind=link}