 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 5, No. 1, March, 2005, pp. 50-54 Human immunodeficiency virus (HIV) seropositivity and hepatitis B surface antigenemia (HBSAG) among blood donors in Benin city, Edo state, Nigeria Patience Idia Umolu, Lawrence Ehis Okoror and Philip Orhue Department of Microbiology, Faculty of Natural Sciences, Ambrose Alli University, Edo State, Nigeria Correspondence to: Dr. Idia P. Umolu, Department of microbiology,Faculty of Natural Sciences, Ambrose Alli University, P.M.P 14, Ekpoma, Edo State, Nigeria. Larison86@yahoo.com Code Number: hs05010 ABSTRACT Background: Human Immunodeficiency Virus and Hepatitis B virus are blood borne pathogens that can be transmitted through blood transfusion and could pose a huge problem in areas where mechanisms of ensuring blood safety are suspect. This study became necessary in a population where most of the blood for transfusion is from commercial blood donors. African Health Sciences 2005; 5(1): 55-58 INTRODUCTION
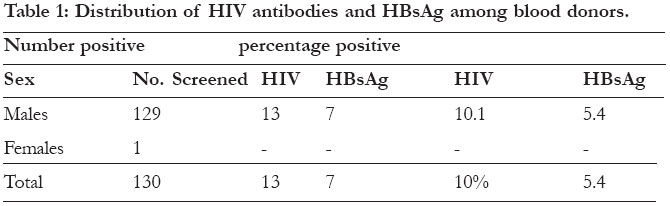
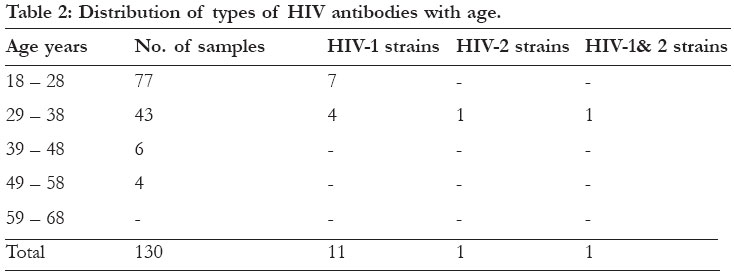
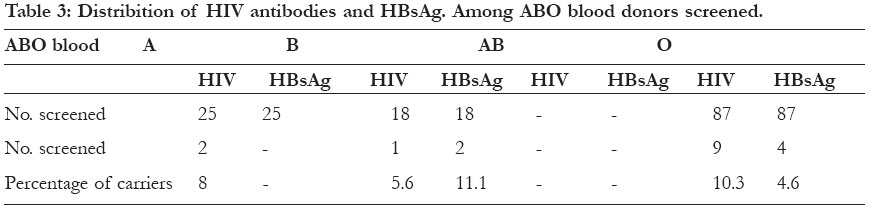
Acquired immune deficiency syndrome is a life threatening complication of HIV, which is a retrovirus having two strains namely; HIV 1 and 211. Sub Saharan Africa has been severely hit by the HIV/AIDS pandemics11. HIV is now the leading cause of death in Africa replacing malaria and other communicable diseases. Hepatitis B viral infection is one of the world most fatal malignancies. There have been fears about hepatitis B vaccine in AIDS transmission and Hadler et, al.,4. Postulated that infection with the Human immunodeficiency virus might alter the immune response to hepatitis B vaccine. Hepatitis B virus and HIV are know to be transmitted through sexual intercourse, blood and blood products, shared needle, other body fluids such as semen, virginal fluid and breast milk6,12. Due to the risk of transmission of HIV through breast milk, many mothers have been advised not to breast feed7. However, recent research has shown that exclusive breastfeeding for 3 months results in less transmission than artificial feeding8. In Nigeria, the prevalence of HBsAg in normal population ranges from 2.7% to 13.3%9 – 11. The epidemiology of human immunodeficiency virus infection has been described in detail by many worker15, 6. Over the years, the rise from 2 in 1986 to 436 in 1992 and by December 1995, 5,201 cases had been reported to the national STD/AIDS control program13. But today, it is estimated that about 6million people are already infected with AIDS virus although the official records put the population of those infected with HIV in Nigeria at 2.5million. Everyday records also show that by December 1998, 1,000,000 Nigerians were already living with AIDS or already killed by it and 9 of every 10 cases of HIV infection occur through sex15. Human immunodeficiency virus and hepatitis B virus infections are two major viral infections worldwide. The presences of infection markers to these two viruses in blood donors obviously present great risk to recipient. In this study we report the prevalence HIV seropositivity and Hepatitis B surface antigenemia in blood donors in order to ensure that proper screening of blood and blood products in the population sampled are effected, it is also aimed at ensuring proper counseling of blood donor. MATERIALS AND METHODSA total of 130 blood samples were collected by venal puncture into sterile vacutainiers from blood donors in Benin City. The red blood cells were used for ABO typing while the sera were collected aseptically after centrifugation at 3000rpm for ten minutes into sterile containers and preserved at -20°C until tested for the presence of HBsAg and antibody to HIV. Prior to testing the sera were allowed to attain room temperature. For the detection of Hepatitis B surface antigenemia, Quimica Applicada kits were used as described by the manufacturers. Antibodies to human immunodeficiency virus or HIV seropositivity were determined using immuncomb II HIV 1 and 2 Biospot kit. RESULTSA total of 130 apparently healthy blood donors were screened for antibodies to human immunodeficiency virus (HIV), and hepatitis B surface antigen (HBsAg) using the immunocmb II HIV 1 and 2 Biospot and the Quimica Clinical Aplicada direct latex aggulation respectively. Ten (7.70%) were voluntary donors while 120 (92.3%) were commercial donors. Table 1 reflects the carrier rate of HIV antibodies and HBsAg among the blood donors with 13 (10%) being positive for HIV antibodies and 7 (5.4%) were positive for HBsAg. Of the total positive cases, eleven had HIV – 1 strain, one had HIV – 2 strains, one had both HIV 1 and 2 (Table 2). The blood group O had the highest number of donors and 9 (10.3%) and 4 (4.8%)
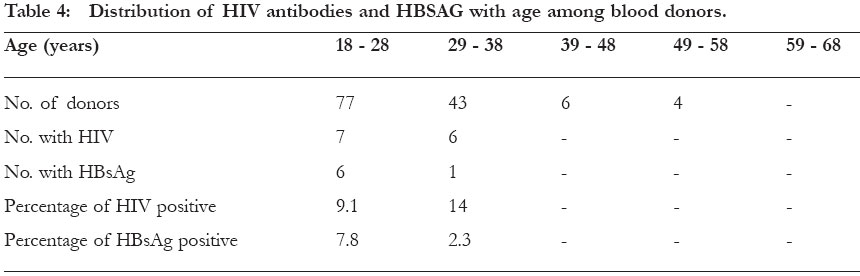
positive cases for HIV The rate of occurrence was found to be higher among the group 18 – 28, 6 (7.8%) for HBsAg and 29 – 38 had 6 (14%) for HIV (Table 4). DISCUSSIONThe prevalence of HIV antibodies and hepatitis B surface antigen in blood to be transfused to recipient who by virtue of his/her compromised health status (e.g. anemia or surgery) is thought provoking and leaves room for serious concern. Most people infected by these viruses have no symptoms and do not know that they carry the virus, but all who are infected can transmit the virus to others15, 16. This is further compounded in cases of donors, in that after testing positive to the viruses, counseling is withheld as it is thought that it may frustrate donors and lower the blood pool. The effect of this action is that, those uncounselled seropositive donors are innocently infecting the society17. In Nigeria, the prevalence of HBsAg range from 6 – 11% among blood donors10. Further research on the incidence of HBsAg in the Northern Nigeria blood donors, revealed that 8.9% of 1860 blood donors tested were positive19. This study revealed a prevalence rate of 5.4% among blood donors in Benin City, which is lower than the result obtained in Northern Nigeria. However, there could be a steady rise in the infection rate when considering the rate at which the youths who form the bulk of donor engage in indiscriminate sex. The lack of interest in protected sex (use of condoms) may be a factor that could lead to the steady rise of infection due to both viruses. So there should be a creation of enough awareness by those involved in formulating policies on blood donation and everyone interested in building a safe society. Among the 130 donors screened for HIV using immunocomb II HIV 1 and 2 Biospot, a total of 13 (10%) was found to be positive, they were confirmed with immunocomb Firm. Eleven out of the 13 positive cases had HIV 1 as compared to HIV 2, one had HIV 1 and 2 the high increment in HIV 1 as compared to HIV 2 is as a result of high social habits of individuals. Simultaneous presence of antibodies to HIV 1 and HIV 2 was observed in this study. This is in harmony with what was observed by DeCock and BrunVezinet5. Okolie17 stated that HIV is on the increase in Benin City. Since the predisposing factors to HIV are similar to those of hepatitis B virus, hepatitis B virus infection could also be on the increase. Though no relationship exist between hepatitis B surface antigen and human immunodeficiency virus with ABO blood group9, 20. The study showed that most donors were group O and subsequently had the highest HBsAg and HIV seroposititvity prevalence rate. The high rate of infection noticed in commercial donor may not be unconnected with lack of awareness, since most of the commercial blood donors in this part of the world are actually those from low socio-economic class where the campaign against these dreaded diseases are limited. They still engage in indiscriminate unprotected sex and drug addiction, which could even, be a factor to which they decided to be commercial blood donors. They will need money to maintain their life style (sex and drugs). And it has earlier been reported that sex remains a major transmitter of both viruses in this part of the world14. Hence extra care should be taken when it comes to blood from commercial donors. The apparent lack of incidence in voluntary donors could be due to the fact that they are stable and probably aware of the HIV / hepatitis scourge. This does not mean that voluntary donors are not carriers but the prevalence is low, as some may also be involved in indiscriminate sex and drug addiction12. However, the involvement of voluntary blood donor is not conclusive in this study, since the number of voluntary blood donors screened is statistically insignificant using the student t test at 95% confidence limit (ten as against 120 for commercial blood donors). The age range of 18 – 28 had the highest number of positive cases for HBsAg while 29 – 38 had the highest number of positive cases for antibodies to HIV. Hepatitis B surface antigenemia HIV were higher in the younger age than in the older age groups and this younger age group (18-28) is the adolescent age involved in active sexual activity. This is harmony with the report of Awosere et, al.1. The fact that age group 29-38 had the highest seropositivity to HIV does not rule out more of the infection in younger age group 18-28 as most of older people may have contacted the infection in their younger active sexual age. UNAIDS correlates that in Africa, AIDS, will be the cause of death of 50% of people now in their teens. The age of peak infection with HIV and HBsAg correlates well with the age of greatest sexual activity, supporting the role of sex in the transmission of HIV and hepatitis B virus. Patients co-infected with HIV and HBV have a high progression to hepatic fibrosis and 3.5 fold increases in hepatic cirrhosis when compared with HIV alone22. Co-infection with HIV and HBV could also increase hepatic cirrhosis and carcinoma. The high incidence of HBV may not be due to HIV infection which has caused a reduction in the immunity of the population in general. Although blood transfusion is not thought as a significant mode of transmission, blood transfusion where mechanisms of ensuring blood surety are suspected, HIV and HBV is prevalent in the community, and where many transfusions are conducted (sometimes needlessly), the problem can be high. There is also problem of the ‘window period’ when the antigens or antibodies are not yet demonstrable; the blood can still transmit the infection3. The possibility of such transmission can be minimized by selecting donors at low risk of HIV and HBsAg infection and by screening blood for the presence of HIV antibodies and HBsAg. A single polymerase chain reaction assay that screen for hepatitis C virus, hepatitis B virus and human immunodeficiency virus in a single assay is now available. African governments should try and make these kits available since it will aid in the diagnosis of these deadly viral infections since it has been noted that PCR can reduce the window period of HIV by 11days. These viruses remain the greatest public heath problem as of today. REFERENCES
Copyright © 2005 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs05010t3.jpg] [hs05010t2.jpg] [hs05010t4.jpg] [hs05010t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}