 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 5, No. 1, March, 2005, pp. 65-68 Pattern of dental caries in Mulago Dental School clinic, Uganda Annet Kutesa1, Andrew Mwanika1, Margaret Wandera2 1.Department of Dentistry, Makerere University; 2. Makerere University Hospital, Kampala, Correspondence Annet Kutesa, Department of Dentistry, Faculty of Medicine, Makerere University, P.O.Box 7072, Kampala, Tel: 077531573 E-mail: kutesam@yahoo.co.uk Code Number: hs05012 ABSTRACTInformation on dental caries among patients attending Mulago Hospital
is scarce. Yet knowledge of the pattern of caries can be used to plan preventive
and treatment interventions. This study describes the pattern of dental caries
(in terms of age group,
tooth and tooth surface and gender) among patients attending the Public Health
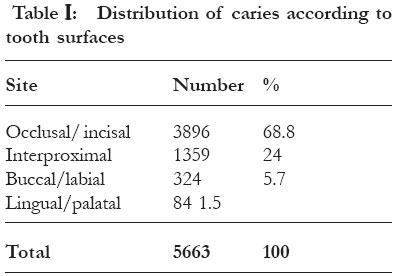
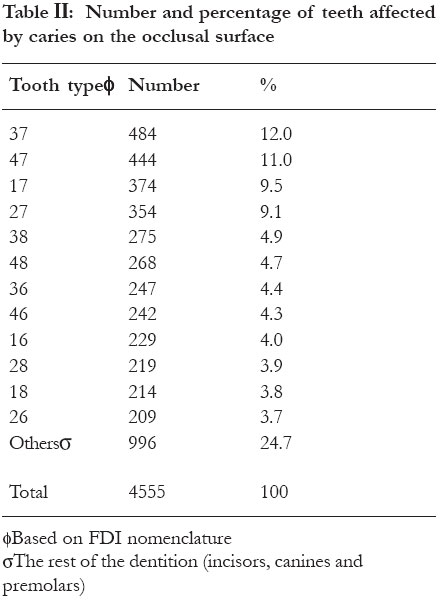
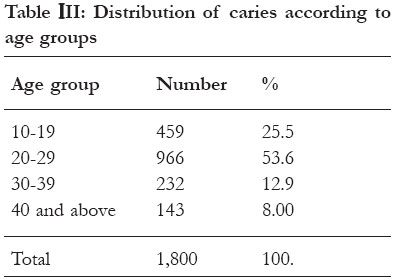
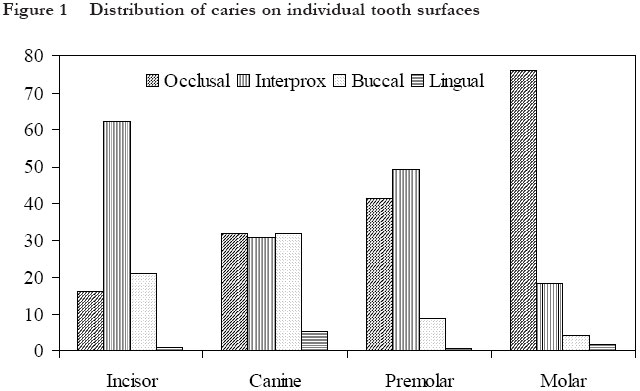
Dental Officers School Clinic, Mulago Hospital. Key words: caries experience, tooth surfaces, occlusal. African Health Sciences 2005; 5(1): 65-68 INTRODUCTION The pattern of caries among other things includes: the rate of attack, distribution, and progression of the disease within the population. This study looked at the pattern of caries among patients who attended the Public Health Dental Officers School Clinic, Mulago Hospital in relation to the type of tooth, tooth surfaces, age groups and gender most affected. Literature on oral health status in Uganda is limited. The available research1 mainly focuses on epidemiological data with respect to incidence and prevalence. Little attention2 has been paid to establish the pattern of dental caries on the individual teeth and surfaces. Data on teeth and surfaces at most risk is scarce in the African region. Yet knowledge about the most attacked teeth and surfaces can contribute to the design of preventive clinical procedures and community-based programmes. In this way resources can be targeted at teeth and surfaces at high risk. This is in line with the recommendations of Ismail et al 3 who suggested that to counteract the potential increase in the prevalence of dental caries in developing countries, preventive and oral health promotion programmes should be planned and implemented and especially targeted at those at greatest risk. Although caries was not taken to be a major problem in Africa 4, 5, there is now evidence of a rise 6-9 in prevalence of dental caries in the developing countries. This rise in dental caries places a further burden on the resources available for oral health. There is therefore, a need to study and understand the pattern of caries in Uganda in order to plan better for the appropriate allocation of these scarce resources. Pack10, in her paper on dental services and needs in developing countries, highlighted the need to focus on primary care, and prevention strategies to be designed and implemented urgently. These would have to be monitored and scientifically analyzed for effectiveness. The aim of this study was to establish the pattern of dental caries among age groups, gender, tooth types and tooth surfaces in patients attending the Public Health Dental Officers School Clinic, Mulago Hospital. METHODS AND MATERIALS This was a retrospective, cross-sectional study of the treatment records of patients who attended the Public Health Dental Officers School Clinic, Mulago Hospital. Students under supervision completed most of the patient record cards reviewed. Treatment records were used in this study because of the availability of the patients’ information long after their treatment is completed. The patient records were reviewed for the following information: diagnosis of caries based on tooth and tooth surface affected11, age and gender. Any card without the above criteria was rejected. Mulago Hospital was used because of the big turnover of patients who come from mainly urban and peri-urban communities. A search of the records for the period 1995 to 1999 was done and 1,800 cards were reviewed. The data was then analyzed using the EPI INFO 6 programme. RESULTS Table I shows the distribution of caries according to tooth surfaces. The sites considered were occlusal, interproximal, lingual and buccal. The most frequently affected site was the occlusal (68.8%) surface and the least affected sites were lingual/ palatal (1.5%) Table II shows the number and percentage of teeth affected by caries on the occlusal surface. The results show that the molars were the most affected of all the teeth with 75.3%. The distribution of caries within the individual molars shows that the second molars contributed the highest (41.7%) and the first molars contributed the least (16.4%). Caries distribution was higher in the lower jaw (53%) than the upper jaw (47%). Table III shows the distribution of caries according to age groups. Patient attendance was highest in the 20-29 age group. However above this age group the attendance decreased with an increase in age. Females showed a higher incidence of (54%) attendance to the clinic compared to the males (46%). Figure I shows the distribution of caries on individual tooth surfaces. The incisors had a high frequency of interproximal lesions (62%). The molars had more occlusal lesions. Generally the frequency of caries on the lingual surfaces in all teeth was very low. DISCUSSIONTreatment records were used in this study because of consistence in record keeping which facilitated easy retrieval of information. It is an inexpensive method of data collection. However, some background information like previous dietary habits and oral hygiene practices, which directly influence the development of caries, was not available on the record forms. It was found that the most frequently attacked site was occlusal, 68.8% (Table Ι), of which the molars contributed 91%. Manji et al 12 had similar findings in 12-year-old urban children in East Africa. The anatomical form of molars (the pits and fissures) probably makes them more retentive to cariogenic food particles and plaque, and therefore more prone to caries attack. The high occurrence of occlusal surface caries in these teeth also indicates that there is a relative lack of preventive procedures like fissure sealing. The high occurrence of interproximal caries in the incisors (Fig. 1) further implies that preventive procedures like regular flossing is lacking in the population. The most affected tooth in this study was the second molar both in the maxilla and mandible (Table ΙΙ). This finding corroborates previous studies in Uganda2, 13, 14 Zambia15 and Nigeria16. Akpata16 and Johnson17 attributed these findings to rural-urban migration at a period when the first molar had reached a high degree of maturation before being exposed to an increased cariogenic challenge. At the same time the second molar is erupting shortly before or during the onset of this challenge. Ismail et al 3 noted that the residents of urban areas in developing countries, regardless of social and economic status, consume sugar containing foods and drinks more frequently than those in rural areas. In contrast Manji et al12 found the first molar to be affected most frequently in 12-year-old urban children in East Africa although the second molar contributed significantly. This study demonstrated that caries activity continues throughout life and is not confined to any period of life, although the incidence decreases with an increase in age. A similar conclusion was made by Manji18. Assuming that the rate of progression of caries takes 3-4 years before it gets to pulpitis, (which is the trigger for seeking services), and considering that the age group most affected is 20-29 (Table III), it is probable that the initial attack occurred in their teens. It is therefore beneficial to target the 10-19 age group with preventive programmes. Of the 1,800 cases reported the ratio of females to males was 54.5%: 45.5%, suggesting females are more prone to caries than males. This could have been due to a number of reasons, which include early teeth eruption that is associated with girls compared to boys, different attitudes towards dental attendance between men and women due to lack of financial independence on the part of the females and difference in dietary pattern between housewives and working men19. CONCLUSIONIn conclusion the results showed a high occurrence of occlusal surface caries in molars especially the second molars in the 20-29 age group in the patients attending the Public Health Dental Officers School Clinic, Mulago Hospital. There is a need to carry out a national survey to verify these findings with the Ugandan population in order to plan better for the appropriate allocation of the scarce resources. REFERENCES
Copyright © 2005 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs05012t1.jpg] [hs05012t2.jpg] [hs05012t3.jpg] [hs05012f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}