 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
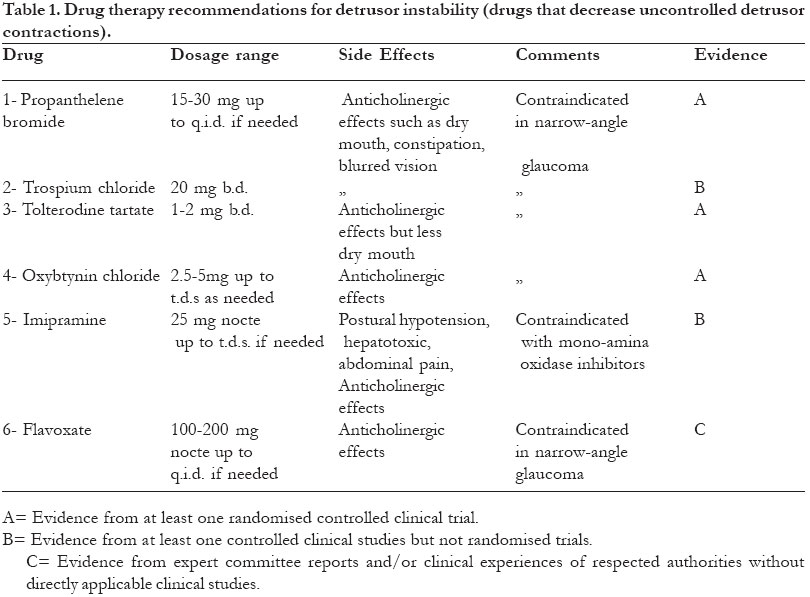
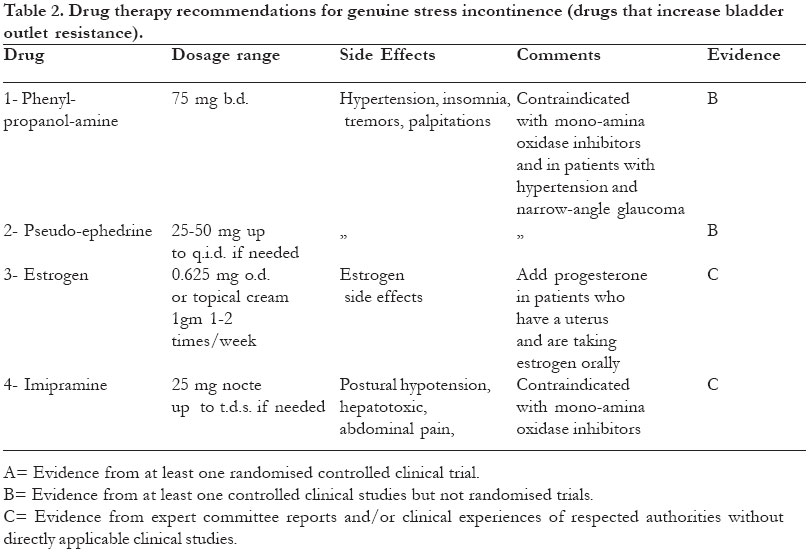
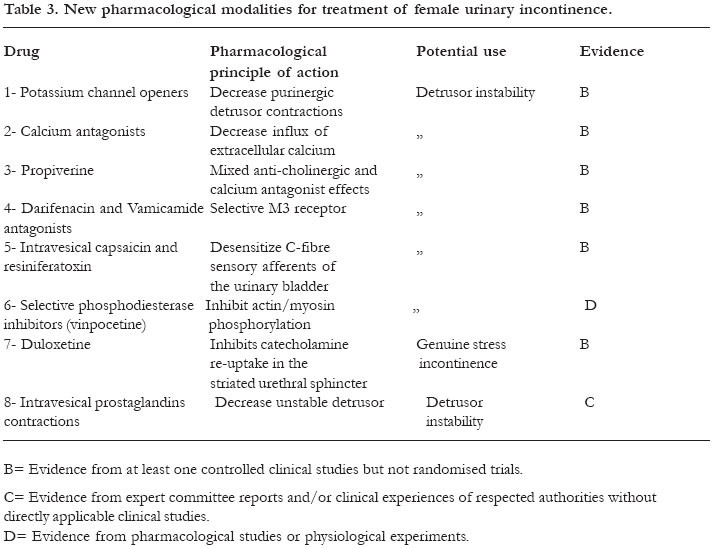
African Health Sciences, Vol. 5, No. 1, March, 2005, pp. 79-85 Practice Points Pharmacological therapy of female urinary incontinence Diaa E. E. Rizk Department of Obstetrics and Gynaecology, Faculty of Medicine and Health Sciences, United Arab Emirates, University, Al-Ain, United Arab Emirates. Author for Correspondence Diaa E.E. Rizk, P.O. Box 17666, Al-Ain, United Arab Emirates. Tel: (971-3) 7672000 Fax: (971-3) 7672067 E-mail address: rizk.diaa@uaeu.ac.ae Abstract Backgound: Although not a life threatening condition, UI is a common problem in women that produces embarrassing and debilitating symptoms, severely affects the quality of life and represents a significant public health problem. The bladder and urethra in women constitute a functional unit that is controlled by a complex interplay between the central and peripheral cholinergic and noradrenergic nervous systems and local regulatory factors. A substantial part of urethral tone in women is also mediated through the effect of estrogen on urethral mucosal function. Theoretically, detrusor instability can be improved by agents that decrease detrusor contractility and genuine stress incontinence by agents that increase outlet resistance. Key words: Drugs, pharmacology, urinary incontinence, women. African Health Sciences 2005; 5(1): 79-85 Introduction Urinary incontinence [UI] is a common distressing and disabling condition causing significant physical and psychological morbidity in women of all ages. Female UI can result from a number of factors such as weakness of the urethral sphincter mechanism (genuine stress incontinence- GSI), diminished bladder capacity or compliance, inadequate bladder sensation and neurological dysfunction (detrusor instability- DI) and genito-urinary fistulas1 . The bladder and urethra in women constitute a functional unit that is controlled by a complex interplay between the central and peripheral nervous systems and local regulatory factors. The detrusor muscle is diffusely and richly supplied with cholinergic nerve fibers from S2-S42. Muscarinic receptors are located predominantly in the body of the bladder. Acetylcholine acts on these receptors to cause a contractile response. Parasympathetic efferents to the bladder also innervate the urethral smooth muscle and cholinergic stimulation produces contraction. The functional significance of this response in women is however unknown. Several subpopulations of muscarinic receptors have been identified (M1-M5) all with a wide distribution in the body. The M3 receptor is thought to mediate bladder contraction3. The presence of noradrenergic terminals in the human bladder from T10-L2 is controversial2. In several mammalian species, a receptor sites producing contraction in response to noradrenaline binding have been shown to predominate in the bladder base whilst b receptors (primarily b2 receptors) producing relaxation, are predominant in the vault. The female urethral smooth muscle contains minimal a adrenergic receptors, primarily a2, which elicit a contractile response when stimulated. A substantial part of urethral tone in women is also mediated through the effect of estrogen on urethral mucosal function4 . Principles of pharmacological therapy I- Agents that decrease bladder contractility (Table 1) 1- Antimuscarinic (Anticholinergic) drugsMuscarinic receptors mediate not only normal bladder contraction but also the principal contractions of the unstable bladder. Antimuscarinic agents are currently the most widely used treatment for DI but they lack selectivity for the bladder and effects on other organ systems may result in anticholinergic side effects that limit their usefulness7,8,9,10 . Propantheline bromide is a quaternary ammonium compound with a documented effect on detrusor hyperactivity in most clinical studies and may in individually titrated doses be clinically useful10. However, in a recent randomized, double-blind, multicentre trial, there was no differences between the efficacy of propantheline and placebo for the treatment of DI11. Trospium chloride is another quaternary ammonium compound with antimuscarinic actions, but also with effects on ganglia12. Several open studies have indicated that the drug may be useful in the treatment of DI with fewer side effects compared to other antimuscarinic agents. Trospium chloride has also a documented effect on detrusor hyperactivity in in-vitro studies5. Tolterodine tartate is a new potent and competitive antagonist at muscarinic receptors, intended for the treatment of DI13. The drug has no selectivity for muscarinic receptor subtypes, but still shows some selectivity for the bladder over the salivary glands in animal models and possibly in man. Several randomized, double-blind, placebocontrolled studies on patients with DI have documented significant reduction in symptoms and the drug was also well tolerated with long-lasting effects on the bladder14. 2- Drugs with ‘mixed’actionsSome drugs have a pronounced antimuscarinic effect and an often poorly defined “direct”action on bladder muscle that may involve blockade of voltage-operated calcium channels. Among the drugs with mixed actions was terodiline, which was withdrawn from the market because it was suspected to cause polymorphic ventricular tachycardia5. Oxybutynin chloride has several pharmacological effects, some of which seem difficult to relate to its effectiveness in the treatment of DI15. It has both an antimuscarinic and a direct musclerelaxant effect, and local anaesthetic actions. Oxybutynin has a high affinity for muscarinic receptors in human bladder tissue and effectively blocks carbachol-induced contractions6,7,11. Several studies, both open and controlled, have shown that oxybutynin is effective in controlling DI16. The therapeutic effect of oxybutynin is however associated with a high incidence of side effects (up to 80% with oral administration). These are typical antimuscarinic and are often dose-limiting. Therefore, forms of oxybutynin other than the conventional 5mg tablet have been introduced; rectal and intravesical administration and a controlledrelease preparation, administered once daily, were reported to have fewer adverse effects5. Oxybutynin thus has a welldocumented efficacy in the treatment of DI and is currently, despite its adverse effect profile, the drug of first choice and the gold standard for treatment of this disorder4-11,15. Antidepressants have been found to have beneficial effects in patients with DI (10). However, imipramine is the only drug that has been widely used clinically to treat this disorder. Imipramine has complex pharmacological effects, including marked systemic anticholinergic actions and blockade of the re-uptake of serotonin but its mode of action in DI has not been established11. Several investigators have shown that the drug can be effective in the treatment of bladder hyperactivity although it is well established that therapeutic doses may cause serious toxic effects on the cardiovascular system5. Flavoxate has mixed actions but the main mechanism by which this drug exerts an effect on smooth muscle has not been established7. The drug has moderate calcium antagonistic activity, can inhibit phosphodiesterase and has local anaesthetic properties and a mild anticholinergic effect10. The clinical effects of flavoxate in DI have been studied in both open and controlled investigations, but with varying rates of success. In general, few side effects have been reported during treatment with flavoxate but its efficacy, compared with other therapeutic alternatives, is not well documented5,11. b Adrenoceptor agonists have a pronounced inhibitory effect on isolated human bladder and the administration of such drugs can increase bladder capacity in man6. Favourable effects on bladder hyperactivity were reported in open studies with selective b2 adrenoceptor agonists such as terbutaline17. However, other investigators have not been able to show this effect4,5. Moreover, b adrenoceptor-mediated responses of the human bladder has recently been shown to be mediated by a β3 adrenoceptor but whether stimulation of this receptor will be an effective way of treating the unstable bladder has yet to be shown in controlled clinical trials17. II- Agents that increase urethral outlet resistance (Table 2)α Adrenoceptor agonists: Several drugs with agonistic effects on αadrenoceptors have been tried as a treatment of GSI but ephedrine and norephedrine (phenylpropanolamine) seem to be the most widely used drugs and have both been reported to be effective10,11. Both drugs directly stimulate α and β adrenoceptors and can also release noradrenaline from adrenergic nerve terminals. These drugs however lack selectivity for urethral α2 adrenoceptors and may increase blood pressure. Attempts have thus been made to develop agonists with selectivity for the human urethra, but presently, no such drug is available. Estrogen: The role of estrogen in the treatment of GSI has been controversial, even though there are several reported studies18. Some have given promising results but this may be because they were observational, not randomized, blinded or controlled. The situation is further complicated because several different types of estrogen have been used with varying doses, routes of administration and duration of treatment. A recent meta-analysis, however found that estrogen therapy alone was not an effective treatment for this condition but may have a role when combined with other therapies such as α adrenoceptor agonists18. Imipramine: Imipramine inhibits the re-uptake of noradrenaline in adrenergic nerve endings and this can be expected to enhance the contractile effects of noradrenaline on urethral smooth muscle11. However, no controlled clinical trials on the effects of imipramine in GSI are available15. New pharmacological modalities for treatment of female UI (Table 3).Potassium channel openers In many animal models and the isolated human bladder, anticholinergic drugs only partially antagonize the cholinergic contractile response5,15. The most widely accepted explanation is that a major portion of neurotransmission involved in bladder contraction is non-adrenergic, non-cholinergic. A purinergic system releasing adenosine 5'triphosphate [ATP] that acts on a subtype of purinoceptors called P2x or the ATP-sensitive potassium channel seems to be the most likely mechanism11. Potassium channel openers are a newly developed group of smooth muscle relaxants that decrease membrane excitability by acting on these channels in the cell membrane to increase potassium efflux resulting in membrane hyperpolarization and reduction of opening probability of ion channels involved in depolarization19. The best known and most clinically tested members of the group are pinacidil and cromakalim. Several experimental and clinical studies have shown that both drugs reduce bladder contractions induced by electrical stimulation, carbachol and detrusor hyperactivity which may be useful in the treatment of DI as a supplement or alternative to anticholinergic drugs19. Calcium antagonists: The activation of detrusor muscle, both through muscarinic receptor and non-adrenergic, non-cholinergic pathways seems to require the influx of extracellular calcium ions through calcium channels as well as via mobilization of intracellular calcium6,7. The former pathway can be blocked by calcium antagonists and theoretically this would be an attractive way of inhibiting detrusor hyperactivity10. However, there have been few clinical trials of the effects of these drugs on DI. Oral nifedipine or intravesical verapamil were not found to be effective in most studies but the latter produced objective improvement in urodynamic variables. Calcium antagonists may also enhance the effects of antimuscarinic agents in DI6,7,10. Propiverine: Propiverine is a new drug that has combined anticholinergic and calcium antagonistic actions and has been shown to have beneficial effects on detrusor hyperactivity in several investigations20. Controlled clinical trials have also confirmed the efficacy of propiverine in patients with DI and suggested that the drug may have equal efficacy with and fewer side effects than oxybutynin. Darifenacin and Vamicamide: Studies with muscarinic receptor antagonists with selectivity for M3 receptors, such as darifenacin and vamicamide21,22 have been in progress and will reveal whether or not the principle of selective M3 receptor antagonism offers therapeutic advantages. As M3 receptors are located not only in the bladder but also in the salivary glands and the intestine, this could mean that two of the most common side effects of anticholinergic drugs, dry mouth and constipation, will not be avoided. Intravesical capsaicin and resiniferatoxin: Capsaicin, the pungent ingredient of red peppers, exerts a biphasic effect on sensory nerves; initial excitation followed by a longlasting blockade through its action on specific ‘vanilloid’ receptors and in sufficiently high concentrations, will cause ‘desensitization’of C-fiber sensory afferents23. Intravesical capsaicin, given in considerably higher concentrations (1-2 mmol/L), has been used with success in patients with DI. Side effects include discomfort and a burning sensation during instillation that can be avoided by prior instillation of lidocaine. No malignant changes in the bladder have been found in biopsies of patients who had repeated capsaicin instillations for up to 5 years. Resiniferatoxin is a resin isolated from some species of a cactus-like plant which has effects similar to those of capsaicin but is >1000 times potent. Further investigations are needed to explore the clinical potential of both drugs in the treatment of DI5. Selective phosphodiesterase inhibitors: In vitro data from functional organ bath studies suggest that Ca/calmodulinstimulated phosphodiesterase [PDE] is important in the regulation of actin/myosin phosphorylation involved in detrusor muscle contraction in humans and that this response can be inhibited by the use of isoenzyme-selective PDE inhibitors such as vinpocetine24. These data are supported by initial clinical experience with the oral administration of this drug in the treatment of DI in patients not responding to conventional pharmacological intervention. Duloxetine: Duloxetine is a combined noradrenaline and serotonin re-uptake inhibitor that has been shown, in animal experiments, to increase the neural activity to the external urethral sphincter. In clinical studies, the drug was effective in treatment of GSI in women and well tolerated with few side effects25. Further recent evidence for the safety and efficacy of duloxetine has accumulated from a number of multicentre placebo-controlled trials 26. Intravesical prostaglandins: The human bladder mucosa has the ability to synthesize eicosanoids and these agents can be liberated from bladder muscle and mucosa in response to different types of trauma6. It is still unclear whether prostaglandins contribute to the pathogenesis of unstable detrusor contractions but these substances may sensitize the sensory afferent nerves of the bladder increasing the afferent input produced by a given degree of bladder filling and triggering involuntary bladder contractions5. Treatment of DI with intravesical prostaglandins or with prostaglandin synthesis inhibitors could be expected to be effective if this is an important mechanism4. However, clinical evidence for this is still lacking15. CONCLUSIONAlthough not a life threatening condition, UI is a common problem in women that produces embarrassing and debilitating symptoms, severely affects the quality of life and represents a significant public health problem. The use of some of the currently prescribed drugs for treatment of female UI is, however, founded more on tradition than on evidence based on results from controlled clinical trials (27). According to current recommendations (Tables1, 2), anticholinergic agents particularly oxybutynin chloride or tolterodine tartate is usually considered the drugs of first choice for the treatment of DI because they reduce bladder contractions and associated symptoms in most patients. Propanthelene bromide is the second-line drug if patients can tolerate the full dosage. Imipramine should be reserved for carefully selected patients. Flavoxate is not recommended for the treatment of DI. α adrenergic agonists such as norephedrine or ephedrine are the first-line pharmacological therapy for women with GSI who have no contraindications for their use particularly hypertension. Estrogen therapy may be considered as an adjunctive agent for postmenopausal women. Imipramine is recommended as an alternative therapy when either agent has proven unsatisfactory. Duloxetine is a new promising drug for treatment of female GSI pending further clinical experience. There is an urgent medical need for a new smooth muscle agent for treating UI in women because current drug therapy of UI is either inadequate or ineffective. The clinical requirement for treatment of the contractility disorders of the bladder and urethra is drugs that affect the excitability of bladder and urethral smooth muscles with no significant effects on neuronal activity or the contractility of the smooth muscle itself so as to maintain normal micturition. Further clinical experience with drugs that selectively modulate the electrophysiological properties and the intracellular pathways of the smooth muscles of the lower urinary tract in women as therapeutic agents for UI is, therefore, awaited with interest. References
Copyright © 2005 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs05015t1.jpg] [hs05015t2.jpg] [hs05015t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}