 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 5, No. 2, June, 2005, pp. 107-113 Perception of peers' behaviour regarding sexual health decision making among female undergraduates in Anambra State, Nigeria 1Okonkwo P. I, 2Fatusi, A. O., 3Ilika A. L.
Corresponding Author: Dr. Adesegun Fatusi Department of Community Health College of Health Sciences Obafemi Awolowo University Ile-Ife, Nigeria adesegunfatusi@yahoo.co.uk (++234) 803-719-7434 Code Number: hs05021 ABSTRACT Background: High-risk sexual behaviours are prevalent in tertiary
educational institutions in Nigeria, but little is known about the social influences
that bear on the reproductive health decision-making and behaviour of the undergraduates.
On the other hand, perceptions regarding the behaviour and influence of peers
have been documented to be key social factors associated with reproductive
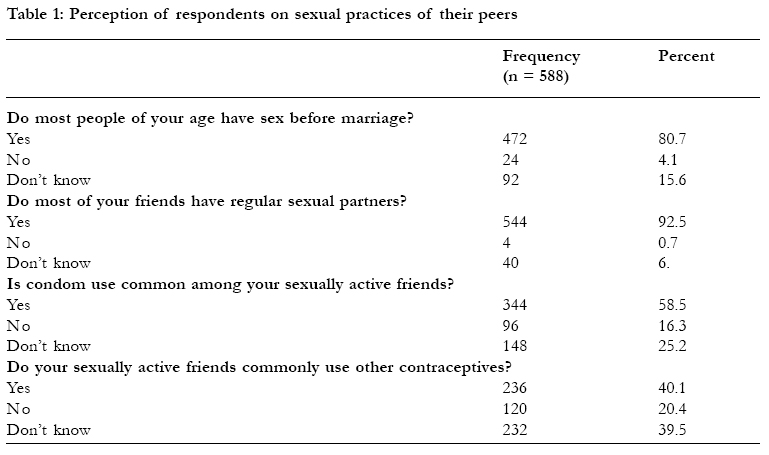
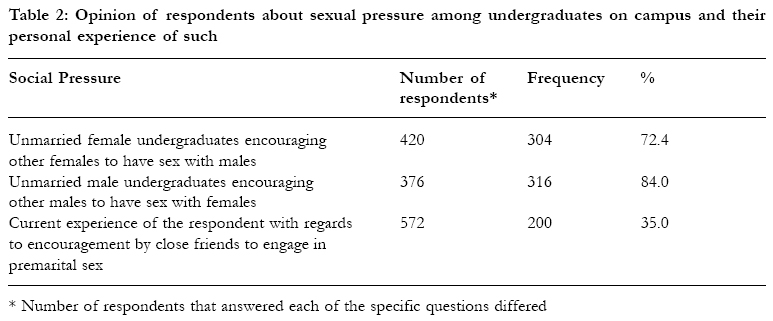
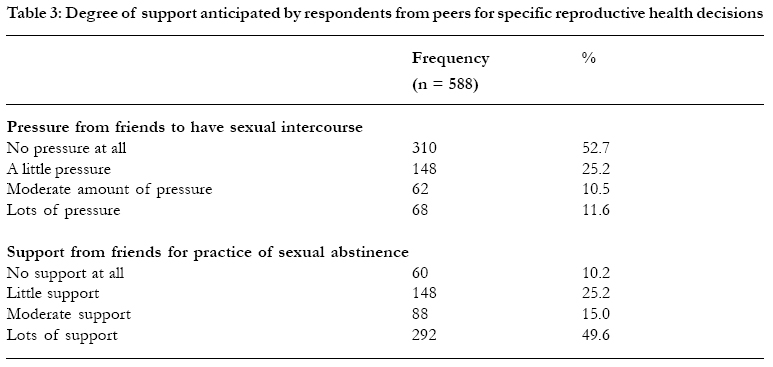
health behaviour of young people. INTRODUCTION Studies on reproductive health behaviour of young people in Nigeria indicate that many adolescents and youths initiate sexual intercourse at an early age and engage in high-risk sexual behaviors. Such risky behaviour include having unprotected sex and multiple partners, with the resultant effects of high rate of unwanted pregnancy, illegal abortions and sexually transmitted infections, among others1-4. Concerns regarding the implications of this behaviour have led to increasing intervention for those in the early phase of adolescent life, particularly in-school adolescents. However, very little attention has so far been given to young adults within the age range of late adolescents and youths. According to the World Health Organisation (WHO), “adolescents” cover the age of 10 to 19 years, “ youths” are defined as belonging to the age group of 15 to 24 years, while the terminology “young people” covers the age of 10 to 24 years5. Young people in institutions of higher learning, who are typically from the age of 18 to 25 years, have particularly been neglected in terms of reproductive health programmes. One factor that may account for this relative neglect of young people in the older age bracket and tertiary institutions is an assumption that members of these latter groups are “mature” enough to take care of themselves. While it is true that older adolescents and youths,potentially, have better access to reproductive health information and services than younger ones, available information shows that their reproductive health risk remains high. The prevalence of risky sexual behaviour is high among students in tertiary institutions despite a high level of knowledge about reproductive health (RH) issues6-8. Indeed, the environment in higher institutions of learning in Nigeria, like that in many other parts of the world, is characterised by high level of personal freedom and social interactions. Socially, the typical university environment in Nigeria offers opportunities for high level of sexual networking, and the "freedom" that characterizes the higher institutions permits permissive lifestyle9. Sexual lifestyles in higher educational institutions in Nigeria, and a number of other African countries, have been documented as featuring a high level of risky sexual behaviour such as transactional sex, engagement with multiple partners, unprotected casual sex, and gender-based violence8, 10, 11. Based on the picture of the sexual behaviour within the campuses, African institutions of higher learning have recently been described as "high-risk institutions for the transmission of HIV"11. Current statistics on HIV/AIDS in Nigeria, provide evidence as to the relatively higher risk that young adults (within the age bracket of undergraduates) face with respect to HIV transmission. The 2001 national survey12, for example, recorded a minimum of 6 percent sero-prevalence level for different categories of young people (6.5% for 25 - 29 years, 6.0 for 20 - 24 years, and 6.1 % for 15 - 19) as compared to all other age categories none of which had a sero-prevalence rate of above 5.0%. Unfortunately as a recent study on Nigeria universities showed, higher educational institutions have so far mounted very little institutional responses to HIV/AIDS. The government and development partners have also, unfortunately, neglected the university environment9. There is now a great need to direct attention to the reproductive health behavior of young people in Nigerian tertiary institutions, in terms of both research and interventions. As the results of numerous studies have shown, the social environment plays an important role in the health-related behaviour of young people, and this include their friends and peers, sexual partners, family members as well as the community, school and other youth-serving institutions13. The impact of peers on reproductive and sexual behaviour of young people has particularly been documented to be strong14-16. Among others, beliefs of young people as regarding the behaviour of their peers have been shown to have impact on their actions in various spheres of health behaviour. Some studies have shown that young people who believed that their peers were using condoms were more likely to use condoms compared to those who had contrary beliefs.14,17,18 The present study specifically aimed to assess the perception of young unmarried Nigerian female undergraduates about sexual behaviour of their peers as well as the type of influence their peers tended to exert on them regarding to sexual behaviour. METHODOLOGYThe study was carried out in two Nigerian tertiary institutions in Anambra state- Federal Polytechnic, Oko (FPO) and Anambra State University of Technology, Uli (ASUTECH). Anambra state is located in the present south-eastern geo-political zone of Nigeria. The choice of the institutions strategically reflected diversity in terms of both institutional types and ownership. While one was a university (ASUTECH), the other (FPO) was a polytechnic. FPO is owned by the federal government and ASUTECH is owned by the state government. While universities are at the top of the ladder in terms of regular academic institutions in Nigeria, the polytechnics rank very close in standard and have a larger proportion of Nigerian youths pursuing tertiary education. Admission to both types of institutions, irrespective of their types and ownership, is conducted through a central federal agency - the "Joint Admission and Matriculation Board" - and is therefore open to all Nigerians. Each institution has its catchment areas, which are typically the state in which it is based and its immediate neighbouring states. Both FPO and ASUTECH, therefore, have a preponderance of students being from South-east Nigeria, which is largely inhabited by the Igbo tribe. While the federal and state-owned educational institutions are quite similar in many respects, a major difference is that state-owned institutions typically charge higher fees than the federal ones. Privately-owned institutions charge higher fees than those charged by the federal or state owned ones. The socio-economic background of students in FPO and ASUTECH is generally similar. Both institutions are located in rural areas, but are easily reachable from Awka, the state capital, and Onitsha, one of the largest commercial centres in Nigeria. This was a cross-sectional study. A total of 600 unmarried undergraduate female students, equally divided among the two institutions, were randomly selected based on a two-stage stratified sampling method. Data collection was by means of a pre-coded, structured and selfadministered questionnaire. The questions were generally close-ended in nature, with provisions usually made for other options (accompanied with the request that respondents should state their opinions in such cases). However, a few questions that sought more in-depth opinion of the respondents on issues of interest to the study were open-ended in nature. The questionnaire had different sections requesting information on socio-demographic characteristics of the respondents and the sphere of social influences surrounding their reproductive health lives, particularly peers and parents/significant adults. The questionnaire had no provision for personal details that might lead to the identification of individual respondent, thereby ensuring confidentiality. Respondents were also assured of confidentiality in writing and participation was declared to be totally on voluntary basis. A total of 588 students, representing 98% respondents' rate, returned the completed questionnaire. Data entry, editing and analysis were carried out by the use of Epi-Info statistical software. RESULTSThe majority of the respondents were youths between ages 20 and 24 years (63.9%), a tenth (10.9%) were adolescents and the rest (25.6%) were aged 25 years. Almost all respondents (98.6%) were christians in terms of religious affiliation: 61.2% Roman catholic 17.7% protestants; and, 19.7 percent belonged to pentecostal christian groups. Most respondents came from homes where both parents had formal education, with only 8.8% of mothers and 6.1% of fathers not formally educated. Whereas the highest level of 21.8% of fathers was primary school education and 31.3% had secondary school as their highest level of education, 23.1% of mothers had only primary school education and 38.8% had a maximum of secondary school education. The proportion of parents that had tertiary education was 40.8% for fathers and 29.3% for mothers. In 95.9% of cases, respondents' mothers were alive at the time of the study while fathers were alive in 81.0% of cases. Three-quarters of the respondents were living with both parents most of the time, 8.5% were living with mothers only, 1.7% with only their father, while 8.2% indicated that they were living in the school accommodation facilities most of the time. A major area of interest in the study was respondents' perception of sexual behaviour among their peers, including engagement in pre-marital sex and use of contraceptives. The majority of the respondents believed that young people of their age were already engaged in pre-marital sex (Table 1). Almost all respondents (92 %) indicated that most of their friends had sexual partners (Table 1). Peers' influence was considered in terms of the general campus environment as well as within the context of the relationship of the respondents with their close circle of friends. Generally, most respondents were of the opinion that females on campus encouraged their female peers to engage in pre-marital sex and males also encouraged their male peers to do the same (Table 2). More than a third of the respondents indicated that they were being encouraged by close friends, to engage in sexual intercourse with the opposite sex. In relation to current context of influences that peers may be exerting on reproductive health decision making, we sought to know the degree of pressure and/or support that respondents were having from friends for sexual abstinence, on one hand, and pre-marital sex on the other hand. The results are shown in table 3 DISCUSSIONThis study explored the issue of peers' influence among Nigerian female undergraduates and holds the potential of contributing to a better understanding of the social context of reproductive health (RH) decision-making among a population sub-group that had been largely neglected both in research and programmatic terms. The respondents, as typical of any Nigerian higher educational institution, were predominantly young adults with three-quarters belonging to the 15-24 year age-group defined by WHO for young people. The religious affiliation declared by the respondents reflected the dominant religious pattern in south-eastern part of Nigeria, and is merely a socio-demographic characterization rather than an indication of religious practice, which was not specifically measured in this study. The socio-economic background of the respondents, as judged from the educational level of the parents (with 93.9 percent of fathers and 91.2 percent of mothers being educated), was slightly higher than the literacy level of 86 percent for males and 82 percent for females in south-east Nigeria19. The perspective of most respondents (80.7 %) that most people of their age are involved in pre-marital sex agreed with the results of recent national surveys in Nigeria. The 2003 Nigeria Demographic and Health Survey (NDHS)19, for example, showed that only 15.9 percent of 20-24 years and 4.0 percent of 25- 29 years had not engaged in sexual intercourse. The National HIV/ AIDS and Reproductive Health Survey20, also conducted in 2003, gave a similar picture with 84 percent of young people aged 20-24 years and 96.9 percent of persons of age 25-29 years documented to have been sexually active. The fact that only 58.5 percent of our study population indicated that condom use was common among their friends suggests that a high proportion of sexual activities among undergraduates may be unprotected. While studies conducted on Nigerian campuses have shown that a large proportion of undergraduates considered themselves as being not at risk for HIV/AIDS6,9, a gradual increase in self-perception of risk is being observed. Compared to a 1994 study6 that reported only 40 percent of university students as considering their group as being at risk for HIV, a 2002 study8 documented that 52 percent of undergraduate students were of the opinion that they were at higher risk of contacting HIV as compared to the general population. On the other hand, the utilization rate of condom remains low in the Nigerian population, even in high-risk sexual encounter19. The response of 40.1 percent of study participants that their sexually active friends were using other forms of contraceptives suggests that condom may not be the contraceptive of choice among many unmarried sexually active undergraduates. It may also be a reflection that even among those that use the condom, it may not be used all the time (with other contraceptives being substituted at other times) or that "dual protection" (the simultaneous use of condom and another contraceptive method for concurrent protection from sexually transmitted infections and pregnancy) is being practiced by a number of students. The former picture is the more likely as studies have shown that pregnancy prevention is of greater focus and concern among undergraduates than sexually transmitted infections even when using condom8. A high level of negative perception about condom had also been reported among Nigerian undergraduates, with almost half reporting that condom reduces sexual pleasure8. If and when dual protection is practiced, it is not unlikely that it maybe due to some level of distrust for the condom as 69 percent of male undergraduates had been reported to know of an incidence of condom breakage that occurred to a close associate. The result of that study further indicated that the reproductive health risk may be high even among undergraduates using the condom and suggested that their efficacy in the use of condom may be low. The high proportion of respondents that indicated lack of knowledge about the contraceptive practices of their friends (25.2 % for condoms and 39.5 % for other contraceptives) may be an indication of inadequate communication among many close associates within the tertiary institution environment about reproductive health issues and practices. Thus, it is not unlikely that institutions of higher learning in Nigeria, despite their general openness to new ideas, may still have some traces of the "culture of silence" that had traditionally surrounded sexual issues and personal reproductive health practices in our environment. In terms of sexual engagement and the influence of peers, the finding that almost half of the female undergraduates had been under some pressure from peers to engage in premarital sex is an indication that the social environment of higher institution may not be very supportive of sexual abstinence. This finding agreed with the observation recently made by Omoregie8 in his study of sexual behaviour of tertiary institution students that abstinence is not a popular practice among Nigerian undergraduates. On the other hand, the indication given by two-thirds of the respondents that they would receive support from their friends if they chose to be sexually abstinent painted a somewhat conflicting and confusing picture. While the reasons for these findings are not entirely clear, it is likely that the findings represented the challenging sexual and reproductive health scenario that are confronting the current generation of young people in Nigeria: to remain sexually abstinent, as demanded by tradition, or to become sexually active as the case is with the majority of their peers. While there is a general belief that the incidence of sexual activity among young people is increasing in the Nigerian society, various studies had indicated that majority of parents and adults still believe that young people should not be sexually active.21,22 Thus, the co-existence of pressure for sexual engagement and anticipated support for abstinence from peers, as found in our study, may be a reflection of the state of dilemma of today's Nigerian undergraduates - raised under parents with the moral standard of sexual abstinence but growing up in a more permissive generation and environment where premarital sex appears increasingly as the norm. There is the possibility with this scenario that while pre-marital sexual engagement appears as the current trend, there is still considerable thought about sexual abstinence among Nigerian young adults in deference to their parents' desire particularly when they are resident with their parent most of the times (as was the case with our respondents). Another possible explanation for the opposing picture of pressure to be sexually active alongside that of anticipated support for sexual abstinence may be that while friends may advance a particular position on sexual behaviour, ultimately most friends in the social context of the Nigerian female undergraduates would likely respect the final choice of their friend to engage in sexual practices or to abstain from such. The influence of other factors that may shift the decision of the individual female towards pre-marital engagement or sexual abstinence may include parental influence and other alternative social support structure. There is a need for more detailed study, which would involve the use of both quantitative as well as qualitative methods to facilitate a better understanding of the situation and uncover associated issues. The findings from this study have implications for both programme and research activities. In terms of programme design and implementation, the findings indicate that in order to improve sexual behaviour among young people in Nigerian tertiary education interventions must target the totality of their social environment. This implies, among others, that in programming for sex-related behaviour change communication in the Nigerian universities, priority must be given to the use of theories that are applicable at the social and community level such as the social learning theory and the structuralenvironmental models. 23 The structuralenvironmental theories of behaviour change, which holds that sexual behaviour is a function not only of individual and social but of structural and environmental factor as well, would particularly provide an appropriate framework for such interventions.24,25 Another implication for programming purpose in terms of communication for sex-related behavioural changes in Nigerian campuses is that abstinence must not be discountenanced, despite the high level of sexual activity, and abstinence message must not be assumed to be appropriate for all groups. Rather, a holistic packaging of communication focusing on abstinence, faithfulness between partners, and condom use is needed. In terms of future research activities, our findings showed that there are still considerable gaps in the understanding of the social context of sexual behaviour among young undergraduates, and the degree to each of the elements in the social environment influence the actual behaviour. These issues need to be examined through the lens of appropriate psycho-social research work. REFERENCES
Copyright 2005 - Makerere Medical School, Uganda |

{kind=link}
{kind=link}
{kind=link}