 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 5, No. 2, June, 2005, pp. 126-130 Evaluation of CD4+/CD8+ status and urinary tract infections associated with urinary schistosomiasis among some rural Nigerians. 1OPG Nmorsi, 2NCD Ukwandu, 3OA Egwungenya and 1Obhiemi NU 1Department of Zoology, Ambrose Alli University, Ekpoma, Nigeria Corresponding author: Nmorsi OPG P.O. Box 902, Ekpoma, Edo State, Nigeria. Email: nmorsiopg@yahoo.com Code Number: hs05023 ABSTRACT Background: Data on urinary schistosomiasis in Nigeria are mainly
epidemological. The knowledge of co-infections of urinary schistosomiasis and
other pathogens are important epidemiological tools for the control and health
benefits of the rural dwellers. The granulomatous reactions in urinary schistosomiasis
is CD4+ dependent. The CD8+ is cytotoxic to parasites and it is activated by
CD4+. These parameters therefore participate in the immune responses to urinary
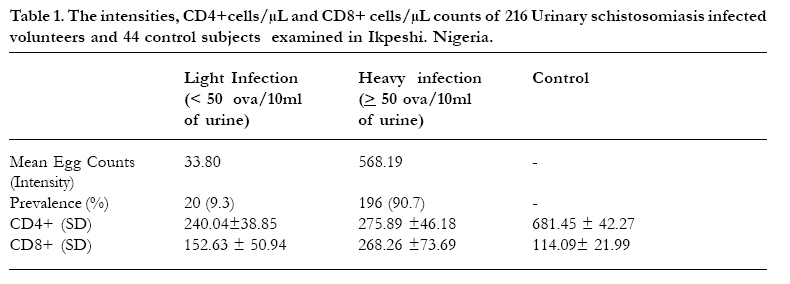
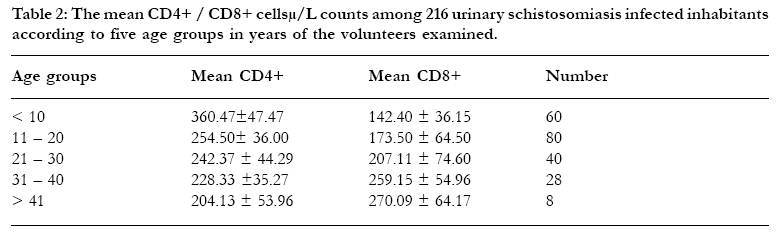
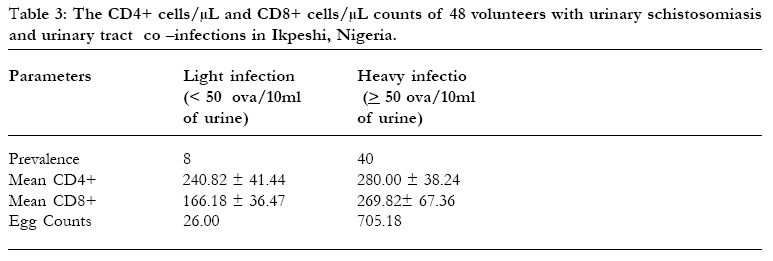
schistosomiasis Key words: CD4+, CD8+, urinary tract infections, urinary schistosomiasis, rural Nigerians. INTRODUCTION Schistosomiasis is a major public health concern in the tropics and subtropics because of its prevalence, associated morbidities and at times mortality. This disease is endemic in 74 countries and it infects more than 200 million people with 500 to 600 million at the risk of infection1,2. The immunopathological consequences of schistosome infections are as a result of the parasite eggs trapped in the host tissue which releases antigens that stimulate granulomatous responses followed by fibrotic reaction 3,4. The granulomatous inflammation in schistosomiasis is known to be dependent on CD4+ (5,6), among other factors such as eosinophils, macrophages, fibroblasts. The CD4+ produces cytokines which activates CD8+ among other factors such as macrophages and B cells. The CD8+ are cytotoxic. These substances participate in the immune response of the host. These granulamas along with the ultimate deposition of collagen results in most fibro-obstructive lesions of schistosomiasis. The granulomas at the lower end of the ureters impede urine flow and causes hydroureter and hydronephrosis7. The data on urinary schistosomiasis in Nigeria are predominantly epidemiological8-15. Because of the prevailing conducive environmental and socio - economic factors of the inhabitants living in rural communities of developing countries like Nigeria, multiple parasitic infections abound11. Reports of this type are quite invaluable in planning a comprehensive epidemiological investigations of tropical diseases. In Ikpeshi, reports on history of dysuria and suprapubic tenderness associated with urinary schistosomiasis had earlier been documented16 without elucidating the possible aetiologies that may be associated with these symptoms. This paper therefore attempt to address this problem. This paper reports the co-infections of urinary schistosomiasis and urinary tract infections in a rural community. Also it provides information on aspects of immune responses of this parasitic infection by evaluating the CD4+ and CD8+ status. MATERIALS AND METHODS Study Area Ikpeshi is a rural community in Akoko - Edo Local Government Area of Edo State, Nigeria which lies between latitude 6oN and longitude 6oE. The inhabitants are predominantly farmers who visit stream/river and burrow pits for their domestic and recreational activities. These water bodies in the community are infected with snail intermediate hosts of schistosomiasis which have been found to be shedding cerceriae. Study Population (Patients)Two hundred and sixteen volunteers who excreted S.haematobium ova in their urine sample were recruited for this study. Their age ranged between 5 and 60 years. Ethical permission was obtained from the State Ministry of Health and the local Health Authority. Thereafter, consent was obtained after a community mobilization campaign on the importance of the investigation. History and general body examinations to exclude patients with allergy and skin infections were carried out. The gastrointestinal parasites especially hookworm were screened for positivity of infection using the direct smear method on their faecal samples. The negative samples were confirmed after carrying out the formol ether concentration technique. Malarial parasites were screened for using thin and thick blood smear using Leishman's stain, and the individuals with positive smears were excluded from the study. Serum was subjected to screening for HIV type 1 and type 2 using the Global Diagnostic Kits(ACON Laboratories, USA). The negative individuals were then recruited into the next stage of the study. The mid stream urine of the volunteers were collected after a physical exercise of about 20 to 30 minutes into a sterile universal bottle. These urine samples were transported to the Tropical Diseases Research Laboratory of Department of the Zoology, Ambrose Alli University, Ekpoma for further processing. Parasitological investigation using ova in urine on a light microscopy was used to diagnose and confirm the positivity of these 216 volunteers for urinary schistosomiasis. These ova were graded as light infection (< 50 ova/10 ml of urine) and heavy infections (≥ 50 ova/10ml of urine)17. Urine culture and bacteriuria.Bacteriuria was determined and reported as the presence of 100,000 organisims/ml in the midstream urine (MSU)18 . Thereafter the microbiological urine culture was made using the standard microbiological techniques for the isolation and idenification of bacteria19, 20 . Evaluation of CD4+/CD8+ statusTen millilitres of venepuncture blood was collected aseptically from the urinary schistosomiasis infected patients and non infected controls. Blood samples of these patients were collected into EDTA bottles and subjected to CD4+/CD8+ analysis and quantification using the standard procedures by the CD T4 Dynabeads methods. This involved the use of light microscope, Dyna Mechanical rotator and the Dynabeads assay kits (Dynal A/S, Oslo, Norway). 250µl of EDTA whole blood sample from each subject was added to 225µl of buffer solution supplied in the test kit. This was followed by further addition of 25µl of magnetic beads coated with anti-CD4 antibody and the mix was incubated at room temperature on a Dyna rotator. The addition of the magnetic beads was to deplete the monocytes level of the blood sample. At the end of incubation, 200µl aliquot was taken from the supernatant of the monocyte-depleted blood was dispensed into a tube containing 200µl of buffer solution. A further 25µl of beads coated with anti-CD4 monoclonal antibody was added to the tube. The tube was incubated for 10 mins at room temperature on a Dynal Mechanical rotator. Subsequently the beads were separated using the magnetic particle concentrator and washed twice with buffer solution. The isolated CD4 T-Iymphocytes were then Lysed with 50ml of Iysing solution and stained with acridine orange. The stained nuclei were counted in a Neubeur counting chamber (Weber Scientific International) using a light microscope. The results were expressed as CD4 and CD8 cells per microliter of whole blood. Analysis of DataThe data analysis was done using the Micro Soft Excel computer programme. RESULTSThe intensity and CD4+ /CD8+ in cells/µL status of 216 urinary schistosomiasis infected volunteers as well as 44 control subjects are presented in Table 1. Twenty (9.25%) of the volunteers had light infections as defined by < 50 ova/10ml of urine while heavy infections (≥ 50 ova/10ml of urine) occurred among 196(90.74%) volunteers. The CD4+ value for the light infections is 240.04±38.85 and 275.89 ±46.18 for the heavy infections. The CD8+ are 152.63±50.94 and 268.26±73.69 for the light and heavy infections respectively. The mean CD4+ is 257.96 and CD8+ is 210.45 with the CD4+: CD8+ ratio of 1.23. The control subjects had a mean value of 683.27±42,27 and a CD8+ of 114.09±21.58 with the ratio of 5.99. The CD4+/CD8+ status of the 216 urinary schistosomiasis infected in five different age groups in years investigated are presented in Table 2. The table shows that the highest prevalence of urinary schistosomiasis occurred among the volunteers within 11 - 20 age groups while the inhabitants above the 41 years of age had the least infection. The pattern of the CD4+/CD8+ status showed that CD4+ decreased with age with the highest value (360.47 ± 47.47) occurring at <10 years old, while the CD8+ increased with age with the highest value (270.98 ± 64.17) recorded among the inhabitants above 41 years of age. In all, the CD4+ and CD8+ counts were positively correlated with the S. haematobium egg counts in their urine at r = 0.0108 and r = 0.516 respectively. Table 3 indicated that bacteriuria were observed in the urine samples of 48 volunteers. Also these volunteers had co-infections of urinary schistosomiasis and urinary tract infections namely; E, coli, Proteus, Pseudomonas aeroginosa, Staph. epidermidis and Staph. saprophyticus. These individuals had a mean CD4+ of 260.41 and CD8+ of 218.00 and a CD4+ : CD8+ ratio of 1.19. DISCUSSION The data of the prevalence of urinary schistosomiasis showed that more volunteers had heavy infections. This is a reflection of the level of endemicity and can be due to the level of exposure of the inhabitants who depend largely on the infected water bodies in the locality for all their recreational and domestic activities This factor as well as age, and genetic variation among the inhabitants have been suggested as possible reasons for the variation in the intensities of infection with a locality3 . The results on the urinary tract infections and urinary schistosomiasis co - infections showed that 40 out of the 48 with these co-infections had heavy infection. The higher the egg burden, the higher the tendency for more eggs to be trapped. This may indicate more granulomatous responses. These granulomas at the lower end of the ureters impede urine flow, causing hydroureter and hydronephrosis7, 16. When urine retention occurs , it could, among other factor,s predispose the inhabitants to proliferation of urinary tract infections and cystitis7,18. We demonstrated an age dependent pattern of infection where the children had high infections than their adult counterparts. This variation can be explained by the data on the CD4+ and CD8+. The CD8+ which is cytotoxic to the parasites and destructive effects on the cells infected by the pathogen21 might offer a protective effect which increased with age. The net effect is the reduction of the infections accordingly. The occurrence of the highest CD4+ count among the children is immunologically significant as it has been documented that the granulomatous inflammation is known to be dependent on CD4+ cells specific to schistosome eggs antigens5 and that granulomatous formation3 occurs in an environment dominated by CD4+. This is a major part of the immunopathology of schistosomiasis as CD4+ plays strong role in stimulation of antibodies and T cells that will produce the CD8+ which mediate cytotoxicity to the parasites. The net effect is regulation of the immune responses in the urinary schistosomiasis among the inhabitants. However, the mean CD4 values of the infected inhabitants appear low (257.96cells/µL when compared to the control uninfected subjects who had a mean CD4+ of 683.27 cells/µL. This may lead to reduced activation of CD8+ cytotoxic cells apart from fact that other substances like eosinophils and macrophages also contribute to granuloma formation and subsequent imune response. This pattern of low CD4+ and CD8+ will contribute to the maintenance of chronicity and endemicity of urinary schistosomiasis. Despite these comparative low mean values, the correlative measurements of the CD4+ and CD8+ with the S. haematobium ova indicates a relationship which shows that the CD4+ and CD8+ increases as the intensity of infections increases as evident by the increase in intensity of the ova in urine. We reported polyparasitism involving urinary schistosomiasis and urinary tract infections namely; E, coli, Proteus, Pseudomonas aeroginosa, Staph. epidermidis and Staph. saprophyticus among some inhabitants of Ikpeshi, Nigeria. The co- infections of these types among the inhabitants of rural dwellers where health facilities are poor and grossly inadequate should be of epidemiological concern considering the associated morbidities18, 22, 23 and possible mortality. For instance, urinary schistosomiasis is associated with painless terminal haematuria, frequency of micturition due to bladder neck obstruction, bladder or ureteric stone formation, hydronephrosis, renal functional abnormalities, ultimately renal failure with calcified bladder. Also urinary tract infection is associated with asymptomatic bacteriuria, symptomatic acute urethritis, cystitis, acute prostratis, acute pyelonephritis and septicaemia7, 18 22. Considering the above adverse effects of these infections, it becomes imperative to incorporate the management of urinary tract infections into the control programme for urinary schistosomiasis in a rural in tropical environment like in Nigeria where the diseases abound. REFERENCES
Copyright 2005 - Makerere Medical School, Uganda |

{kind=link}
{kind=link}
{kind=link}