 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 5, No. 2, June, 2005, pp. 137-144 The Response Inventory for Stressful Life Events (RISLE) I.refinement of the 100-item Version Emilio Ovuga, Jed Boardman, Danuta Wasserman
Code Number: hs05026 ABSTRACT Background: No indigenous screening instruments are available
for the detection of depression and suicide risk relevant to the context of
patients in Uganda. The Response Inventory for Stressful Life Events (RISLE)
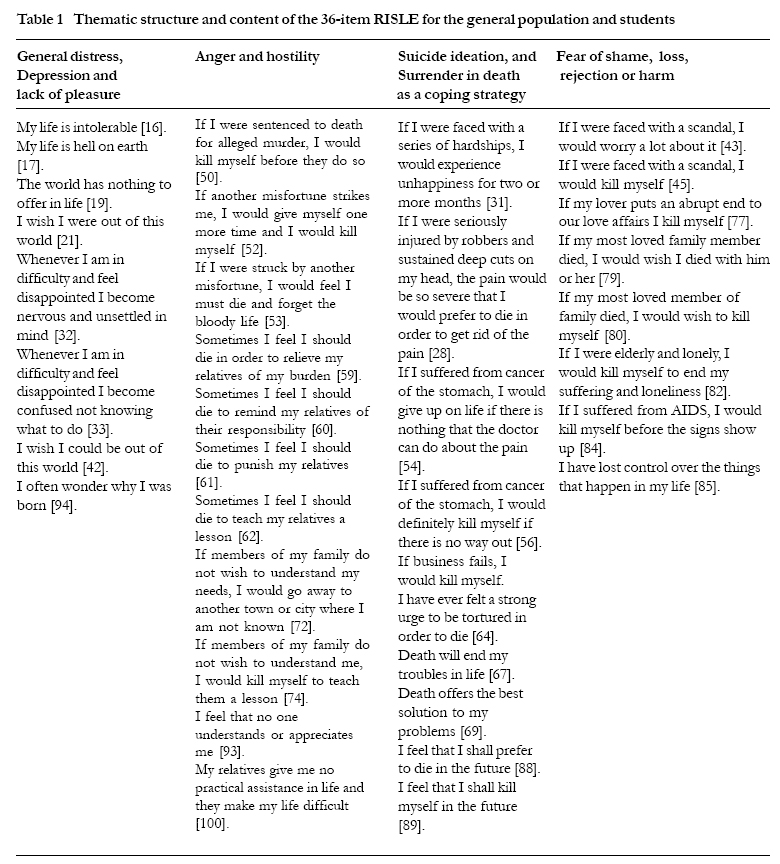
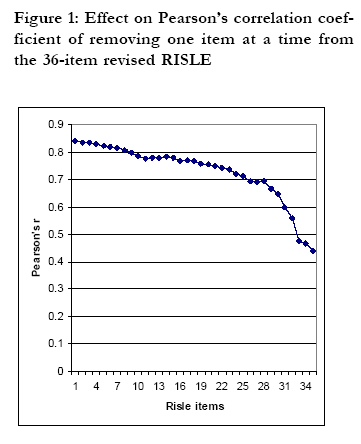
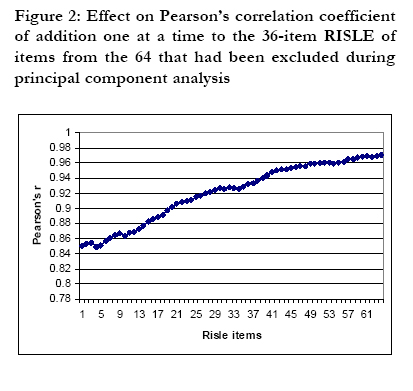
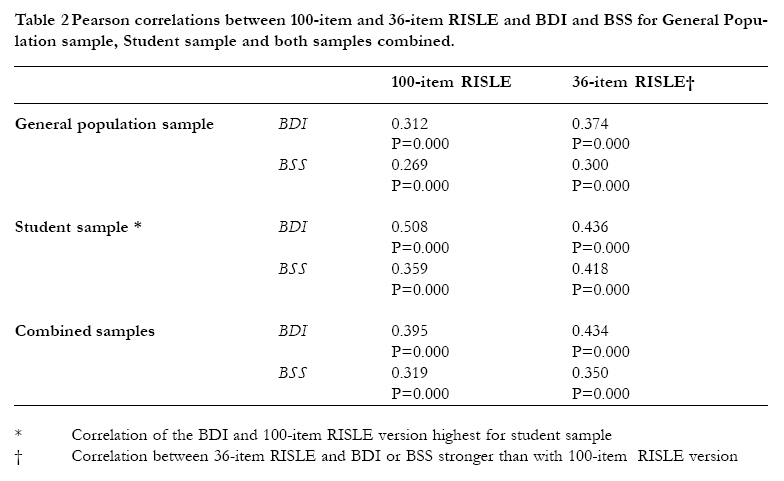
may be an appropriate tool, but requires validation. INTRODUCTION A challenge for psychiatric epidemiology has been to develop highly sensitive and highly specific screening instruments, which can detect individuals with psychiatric disorder in the general population 1. No indigenous screening instruments are available for the detection of depression and suicide risk relevant to the context of patients in Uganda. The present study investigated whether it would be feasible to detect depressed and/or suicidal individuals in the general population using the Response Inventory for Stressful Life Events (RISLE), a questionnaire already developed in Africa. Development of the RISLE The development of the RISLE was based on three assumptions. First, suicide ideations are prevalent in the community and uniformly distributed in the population. Second, suicidal individuals can be identified in primary care with appropriate screening instruments2 and finally, individuals with high risk suicide ideation are at increased risk of completed suicide. The aim was to develop a screening instrument for the identification of people with a high risk of suicide in primary care and the general population. The initial instrument was developed from clinical material gathered during clinical interaction with depressed and or suicidal patients in Kenya and the Transkei Homeland of South Africa from 1982 to 1985. In the course of routine cognitive psychotherapy with depressed suicidal persons, suicidal ideas expressed by patients in response to perceived stressful life events were recorded. The ideas were converted into questions or stem statements concerning hypothetical stressful situations organized around six themes representing attitudes towards oneself, attitudes toward life, attitudes towards one’s social world, responses to stressful life events, passive wishes to die, and active wishes to commit suicide. In the construction of the instrument, each question or stem statement was followed with two or more response items graded to correlate with the likelihood of a suicidal response. Responses were constructed to elicit cognitive evaluation of the hypothetical difficult situations facing the person, and to provide the individual with a range of alternate solutions that people in distress might consider in responding to their situation. Self-destructive tendencies represent the most extreme form of these responses. (See appendix 1). Following a series of studies2-5 a questionnaire with thirty questions or stem statements with 100 response items was developed. Each respondent is instructed to respond to every item with one of four answers: 1. "I strongly disagree", 2. "I disagree", 3. "I agree", or 4. "I strongly agree". In doing so, every respondent is asked to take into account lifetime experiences in addition to how he or she currently feels. The instrument also has a section on background history that includes questions on family history of mental illness, family history of suicide or suicide attempt, personal history of suicide attempt, personal lifetime history of suicide wish or death wish, and past week experience of death or suicide wish. The response items in the instrument comprises a list of negative thoughts and beliefs with suicidal wishes, thoughts about dying, and active intentions to end one's life in response to a stressful event. Along side these items, positive attitudes and problem-solving strategies are included as alternatives. It is the choice of negative attitudes and belief systems that is expected to distinguish the depressed and or suicidal person from the one who is not. Since the primary aim of the screen was to detect suicidal tendencies in people, a neutral and nonstigmatizing name, the Response Inventory for Stressful Life Events (RISLE), was coined. The instrument is heavily biased toward the detection of suicidal feelings and potential in relation to non-health related general distress and experience. The response items were, however, so chosen as to differentiate between non-suicidal and suicidal individuals based on their individual patterns of response to stressful life events. Since suicide ideation is also associated with depressive disorder, it was expected that the RISLE might be effective in detecting individuals with depressive symptoms at the appropriate cut-off point. The results of two previous studies indicated that by using the RISLE it is feasible to detect individuals with probably clinically significant depression2, 4 and suicide behavior5. The present study was conducted because the instrument had not been validated. All previous studies were conducted among student populations2-4 and members of the Uganda armed forces5. This paper is the first of two papers to report on the validation of the RISLE as a screening tool in a Ugandan population. The paper reports on the methods used and the refinement of the 100-item RISLE into a shorter version for use in large samples. The accompanying paper reports on the clinical validation of the shorter version of the questionnaire. METHOD Study populations Two samples were used; a general population sample from the Adjumani and Bugiri districts of Uganda and a student sample from Makerere University in Kampala district. General population sample Adjumani district is situated in the northwestern region of Uganda and has a population of 202,491 with an annual growth rate of 6.3% 6. Bugiri district, with a population of 239,307 and annual growth rate of 3.4%, is situated in southeastern Uganda 6. The populations from the two districts comprised mainly of rural peasants. Study subjects from the general population in the two districts were sampled using multi-stage stratified random sampling strategy 7-9 widely used in rural areas of developing countries (see Ovuga et al, 2004 for further details). Sample size calculation for members of the general population was based on an assumed prevalence for depression of 10% and a standard deviation set at 1.96 for the general population10. Student sample The student sample was drawn from the Faculty of Medicine that comprises of the Faculty of Medicine, and the Departments of Nursing, Pharmacy, Dentistry, and Radiology and the Institute of Public Health. Current undergraduate student enrolment at the Faculty stands at about 650 per year while postgraduate student enrolment is 120 per year. A sample of fresh students who joined various programs at the Faculty during the academic year 2002/2003 was used. Instrument translation The RISLE, the BDI and the BSS were translated into Madi and Lusoga, the indigenous languages used in Adjumani and Bugiri districts respectively, and pre-tested and modified in the course of interviewer training in the district hospital of the respective district. One health educator on the research team from each district ensured the quality of translation (health educators in Uganda are responsible for the production of health education materials in Uganda’s health care system). Ethical clearance The Faculty of Medicine Ethical Review Committee and the National Council for Science and Technology granted ethical clearance for the study. The Dean of Students of Makerere University, civic health authorities and community leaders in Adjumani and Bugiri districts granted further permission for the study. Data Collection Procedures General population sample After the completion of the sampling exercise in the village, all selected adults gathered at the central location where interviews were conducted in small groups by each of five interviewers, and supervised by the first author (EO) and two research assistants. Of the five interviewers in each district, four were psychiatric nurses and one, a health educator. The health educator served as quality controller for instrument accuracy and clarity. The respective District Director of Health Services selected all the interviewers. The subjects were asked to complete the 100-item RISLE, the 13-item Beck Depression Inventory (BDI) 11, 12, the Beck Scale for Suicide Intent (BSS) 13 and to give demographic information. When a subject was illiterate, a resident of the household or village who could write and read helped complete the questionnaires on the instruction of the respondent. Every participant was instructed and supervised to provide their responses on the questionnaires individually except if assisted by someone else. To ensure this, EO and the research assistants, throughout each interview session, supervised the interviewers and respondents. Every evening questionnaire sets were checked for completeness. Student Sample All 180 students in their first year of study in the Faculty of Medicine were approached through their lecturer at the end of a lecture, and invited to participate in the study. After a full explanation of the study including its aims, procedure, risks and benefits, students who did not wish to participate in the study were asked to leave the lecture room. Consenting students were asked to complete the 100-item RISLE, BDI and BSS. Data management and analysis Data was entered using Epi Info version 6.04 and analyzed with SPSS version 11.0. Several analyses were undertaken: Factor Analysis Factor analysis (Principal Component Analysis, PCA), a statistical modeling procedure, reduces the number of items on a screening instrument to those that significantly contribute to the instrument’s power of distinguishing between members of a population with a characteristic from those without the characteristic. The use of PCA reduces questionnaire length without loss of efficacy, enhances brevity of the instrument to promote compliance among respondents and encourages clinicians who wish to use the instrument to increase their detection rates for psychiatric disorder to employ it in clinical practice. Factor analysis further ensures that the resulting instrument items will apply equally to both cases and non-cases in the general population, and that the items have equal chance of eliciting positive or negative responses from cases and non-cases. Thus a positive response from a respondent would denote caseness while a negative response, noncaseness. Factor analysis was performed with the pooling together of all RISLE items for all respondents using the enter method. No selection variable or co-variables were specified to ensure that the resulting instrument applies to respondents of all socio-demographic backgrounds. In performing factor analysis, respondents’ scores on every RISLE item were first converted to either a zero for “I strongly disagree” or “I disagree”, or a one for “I agree” or “I strongly agree”. Using the space saver method, all 100-response items on the original RISLE were entered in the equation. Discriminant function analysis, content analysis and reduction of the RISLE It is hypothesized that depressed suicidal individuals view their social worlds negatively, do not tolerate stressful life events well, and respond to stressors in daily life with negative belief systems and response patterns14, and use suicidal wishes to cope with stressful life events. Suicidal individuals fear real or perceived threat of loss, rejection, harm or death, and they attribute the basis of their fear in the social milieu. Accordingly the suicide prone person does not take personal responsibility to solve his or her problems, but ascribes responsibility for coping in his or her social milieu, which he or she does not approach for help for fear of rejection based on imagined or real previous poor social relations. Rather than solve stressful personal problems in life, the suicidal individual engages in self-destructive behavior to change his or her situation and or elicit support from the social milieu. To test this hypothesis discriminant function analysis of the shortened RISLE, which was derived during the performance of PCA was carried out. Discriminant function analysis is an extension of PCA and it allows for the reduction of the length of a screening instrument to a few meaningful factors that significantly contribute to the performance of the instrument in question. Discriminant function analysis makes it possible to study and group questionnaire items into common themes or groups which seem to make sense and coherent meaning. In order to refine the original RISLE instrument all the factors derived from PCA and which comprised the first function were entered into the equation. The outcome of the procedure was 36 items each of which had a loading of at least 0.500, and had an eigenvalue of at least 1. The items so selected as a result of this procedure formed the refined new RISLE with 36 response items on it. The exercise also examined the contents of the items on the 36item RISLE to determine the probable themes that could be used to describe suicide ideation in the general population. To test the quality and efficacy of the revised RISLE Pearson's correlation coefficient between the shorter 36-item RISLE and the 100item RISLE was calculated. Thereafter one item was dropped at a time from the revised RISLE and corresponding correlation coefficients to the 100item RISLE were calculated. Following this one item at a time was added to the 36-item RISLE from the 64 RISLE items that had been excluded after principal component and discriminant function analysis. Reliability analysis Reliability analysis was performed on the RISLE to determine its homogeneity and degree of internal relationships between its component items. Alpha values were calculated using respondents randomly selected from the data set. Concurrent validity Pearson correlations were calculated between the new shorter form of the RISLE and the 100-item version and between the BDI, BSS and both versions of the RISLE to examine the overall concurrent validity of the two versions of the RISLE. RESULTS Attrition rate Five hundred seventy one questionnaires were collected from Adjumani district and 428 from Bugiri. Forty-seven questionnaires from Adjumani and 13 from Bugiri were discarded for being incomplete, leaving available for analysis 524 (91.7%) questionnaires from Adjumani and 415 (97.0%) questionnaires from Bugiri. Out of 180 students 101 (56.1%) agreed to complete the questionnaire sets. Sample characteristicsGeneral population sample There were 341 (32.9%) females and 696 (67.1%) males in the district study population. Two respondents did not provide information on their sex. The mean ages for the participants were 36.3 (SD=14.4) years for males, 33.8 (SD=9.2) years for females. Eighty three percent (83.9%) of the respondents were aged less than 45 years. The majority of respondents were peasant farmers and only 7.7% worked in other occupations. Student population sample There were 69 (69%) male and 31 (31%) female students. One respondent did not provide information on sex. These proportions represent the ratio of males to females at Makerere University. Seventy five percent of the students were aged 20-29 years, 17.7% aged 30-39 years and 7.3% 18-19 years. The mean age of students was 23.5 (SD=5.0) years. None of the students was currently employed outside their studentship. Factor analysisUsing the space saver method, all 100 response items on the original RISLE were entered in the equation. The end result of this procedure was 18 functions and 48 components, which accounted for 49% of the variance. No selection variable was made to ensure that the RISLE items derived will apply equally to both cases and noncases. Discriminant function analysis and content analysisSelection of component items from the first 18 functions derived from principal factor analysis yielded 36 items with a loading of 0.500 or higher and eigenvalues set at 1. The first function accounted for 98.7% of the total variance with eigenvalues of 106.1. This function was heterogeneous and was made up of four themes, namely, general distress, depression and lack of pleasure; anger and hostility; fear of loss, harm, shame and rejection; and suicide ideation as a way of coping. Anger and hostility, and fear of loss, rejection and shame formed the bulk of the instrument's themes in suicide ideation. In the face of hardships, the suicide-prone individual surrenders to fate and considers death or suicide (suicide ideation) as a coping strategy to attain peace, rest or comfort in life or to mobilize appropriate response from the social support system. The description of these themes, also referred to as factors in the present study, was derived from clinical data and statements made by depressed suicidal patients over many years and may well be described differently under different circumstances15. In keeping with the conceptual framework of the present study, the themes that best approximated the suicidal response patterns of people in distress appeared to fit well with the content of this heterogeneous function. The actual grouping of items into the proposed themes was derived by studying the content and possible interpretation of what they might represent in the understanding of suicide ideation in the general population in Uganda. Table 1 shows the factors and the 36 items of the refined RISLE that collectively describe the respective factors. Reliability analysisAlpha values for the RISLE indicate high internal consistency. Using the Space saver method, internal consistencies for the 100-item RISLE instrument were 0.9171 for 1034, 0.9103 for 515 respondents randomly selected from the data set and 0.9192 for 519 respondents. Alpha values for the 36-item RISLE were 0.8693 for 1038, and 0.8581 for 517 randomly selected respondents. Correlations100-item RISLE and 36-item RISLE The 100-item and 36-item RISLE forms were highly correlated with each other for the combined general population and student data sets (Pearson r = 0.918, P = 0.000). The Pearson correlations between the 100-item RISLE and 36 item RISLE for the general population sample was 0.820 (P = 0.000) and for the student sample was 0.820 (P = 0.000). Quality control for 36-item RISLE Removal of items one at a time from the revised 36-item RISLE resulted in a progressive drop in the value of Pearson's correlation coefficient from 0.842 to 0.439 giving a range of 0.403. Figure 1 that depicts the effect of item removal from the 36-item RISLE indicates that correlation coefficient of the revised RISLE with the 100item version remains high at 0.700 or higher when the shorter RISLE contains 25 items. Addition of items one a time from the 64 items excluded during the process of principal component analysis and discriminant factor analysis resulted in a small rise from 0.842 to 0.971 with a range of only 0.129. See figure 2. RISLE and the BDI The 100-item RISLE was moderately correlated with the BDI in the student and general population samples and in both samples combined (table 2). The 36-item RISLE showed slightly improved correlations with the BSS for the general population and for both samples combined. RISLE and the BSS The 100-item RISLE was moderately correlated with the BSS in the student and general population samples and in both samples combined (table 2). The 36-item RISLE showed slightly improved correlations with BSS for the general population and student samples and for both samples combined. DISCUSSION The present study was conducted to reduce the number of items of the RISLE from 100 items to a shorter 36-item version to improve the scale's clinical utility, and to validate the use of the RISLE scale in the Ugandan population. This paper has presented the RISLE and outlined the attempt to refine the 100-item version by reducing it to a more practical and shorter version that may be more readily used in large samples. The resulting 36-item version appears to have face validity and to perform as well as the 100-item version when compared to two familiar questionnaires measuring depressive symptoms and suicidal ideas. Reliability analysis revealed high levels of internal consistency. The shorter RISLE Using principal component analysis and discriminant function analysis, the 100-item RISLE was reduced to a short 36-item version. A comparison of the 100-item RISLE revealed that it correlated significantly but moderately with the BDI and BSS in the general population. The revised 36-item RISLE was highly correlated with the 100-item long form, which would require considerable time in its administration, a factor that is a serious disincentive in population surveys if the 100-item version were used. Correlation coefficient between the 100-item RISLE and the revised version remained high even though the shorter version was reduced to 25 items suggesting that factor reduction of the 100-item RISLE with the use of principal component analysis did not compromise on the efficacy of the RISLE as a screening instrument in non-clinical settings. The high correlation between the short and long forms of the RISLE suggests that screening with the short form might achieve reliable prevalence rates in the general population. Correlations were better between both the 100-item and 36-item RISLEs and the BDI than the BSS suggesting that the RISLE and BDI share common properties, and therefore overlap somewhat in their ability to detect current psychological distress, probable cases of depressed mood and suicide risk. The suggested overlap between the RISLE and the BDI is probably explained by the fact that both instruments appear to detect significant levels of general dysphoria that qualitatively characterizes depressed mood, psychiatric disorders and high-risk suicide ideation. The RISLE is a dimensional scale that can be utilized for screening purposes. However in utilizing the RISLE as a screening tool in the general population, the instrument does not detect specific psychiatric disorders but appears to detect evidence of dysphoria common to all forms of psychiatric illness suicide behavior. It is this evidence that should then alert the clinician to the possibility of specific psychiatric disorder and suicide risk, which should be confirmed by diagnostic clinical interview. RISLE themes The RISLE was reduced in length from 100 items to 36, and the main themes in suicide ideation were determined. Since the instrument was derived from clinical materials in suicide behavior, the short form of the RISLE was heavily biased toward the detection of suicide ideation. Thematic analysis of the instrument revealed four areas in suicide ideation including general distress, depression and lack of pleasure; anger and hostility; fear of shame, loss, rejection and harm; and suicide ideation as a coping strategy. Content analysis of the four themes suggests that suicidal thoughts are probably used as coping strategies in the face of adversity, and that fear of rejection, and anger and hostility, are important determinants of suicidal thoughts. The 36-item version was subject to further tests of clinical validity and these are reported in the accompanying paper. AcknowledgementsThanks to The Swedish National Center for Suicide Research and Prevention of Mental Ill-Health (NASP) and the Department of Public Health Sciences at the Karolinska Institute, Stockholm, Sweden for developing in collaboration with the Makerere University, Kampala, Uganda of a Ugandan National Plan for Prevention of Mental Ill-Health and Suicide. We are grateful to Dr Seggane Musisi for valuable comments and guidance. Declaration of interestThis study was supported by SIDA/SAREC funds to build research capacity at Makerere University. Reference:
Copyright 2005 - Makerere Medical School, Uganda |

{kind=link}
{kind=link}
{kind=link}
{kind=link}