 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 5, No. 2, June, 2005, pp.157-163 Esophageal cancer in north rift valley of western Kenya Johnston Wakhisi, Kritika Patel, Nathan Buziba, Joseph Rotich Moi Teaching and Referral Hospital Eldoret, Kenya, Moi Teaching and Referral Hospital, Eldoret, Kenya Correspondence to: Dr. Johnston Wakhisi Faculty of Health Sciences Moi University P. O. Box 4606 Eldoret, Kenya Email: jwakhisi@yahoo.com Fax: 254-053-33041 Tel: 254-053-31743 Code Number: hs05029 ABSTRACT Background: Cancer of esophagus is the 9th most common
cancer in the World and the 5th most common cancer in developing
countries. It is aggressive with poor prognosis especially in its late stage.
Cancer of esophagus is geographically unevenly distributed with high incidence
found within sharply demarcated geographic confines. Earlier reports from this
country indicated relatively high proportion of cases in residents of Western
and Central provinces with low incidence in the residents of the Rift Valley
Province. This does not seem to be in agreement with our findings. Several
aetiological factors have been associated with this type of cancer although
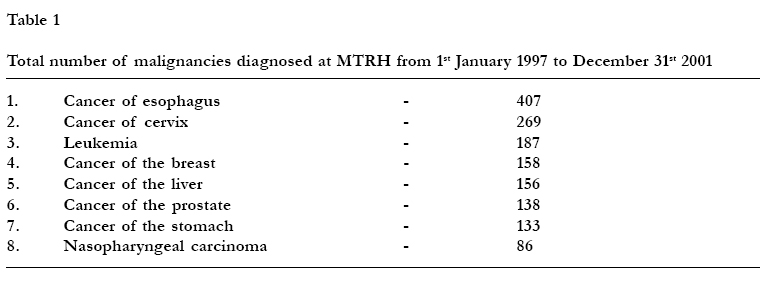
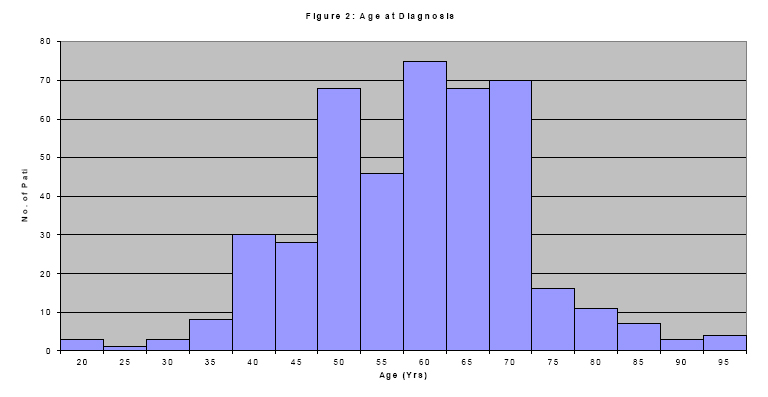
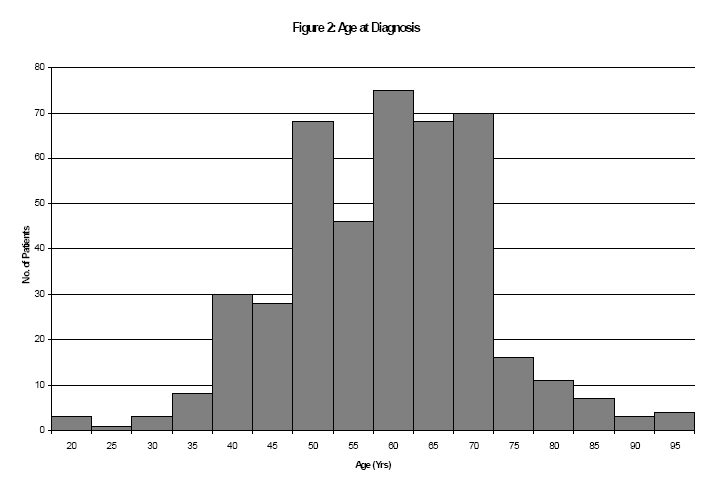
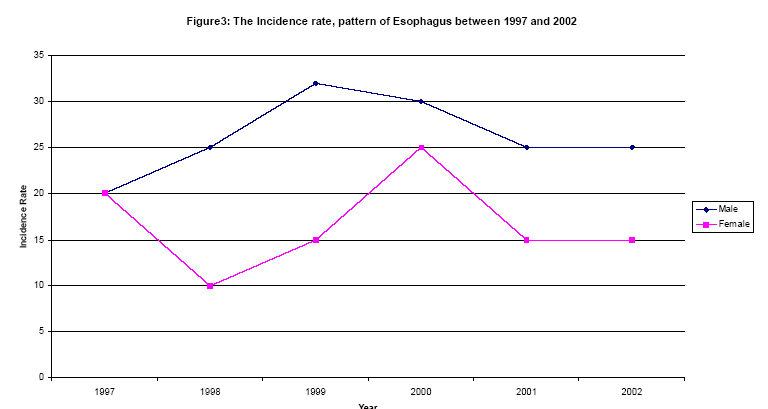
their definitive mechanistic role is not clear. INTRODUCTION Esophageal cancer is the 9th most common cancer in the world, and the 5th most common cancer in developing countries, with approximately 300,000 newly diagnosed patients every year1. A unique epidemiological feature of esophageal cancer is its very uneven geographic distribution, with high incidence found within sharply demarcated geographic confines2. These geographic ‘hot spots’ include areas in Northern Iran, Kazakhstan, South Africa, and Northern China3 where annual incidence rates can exceed 200 per 100,0004. In contrast, the incidence rates in most of North America and Europe are much lower, generally between 5 and 10 per 100,000 per year1. On the African continent, a number of reports have documented a very high incidence of esophageal cancer in South Africa, particularly in the Transkei districts 5. There have been few reports regarding the occurrence of esophageal cancer in Central and Eastern Africa6. In Kenya, Ahmed and Cook published several report series from 1966-1971 involving relatively few patients2,7. These reports indicated that in certain regions of Central and Western Kenya, esophageal cancer ranked as the first or second most common cancer. However, at the same time, in nearby regions of Uganda and Tanzania, this cancer was much less common. Ahmed and Cook2, on the basis of an analysis of records from Kisumu hospital, suggested that the area of high incidence of esophageal cancer was localized in Central Nyanza district, close to Lake Victoria. Gatei et al3 in 1978 reported an uneven geographic distribution; relatively high proportion of cases occurred among individuals from the Luo and Luhya tribes, who originate from Western Kenya (around Lake Victoria), while <1% of esophageal cancers in their register were from the Kalenjin people of the Rift Valley, the majority of the people around Eldoret where our hospital is located. They reported that the incidence among the Kalenjin, was 0.2 per 100,000 per year, and the overall incidence for the country was 0.67 per 100,000 per year. This study ranked esophagel cancer as the 5th most common cancer nationwide, accounting for 5.4% of all solid malignancies3. They used data from the histopathology register at Kenyatta National Hospital. Unfortunately, these rates were based on the assumption that all cases of esophageal cancer were reported to the Kenya cancer registry at the hospital. These numbers are clearly a gross underrepresentation of the actual incidence, as accurate case reporting to the Kenya Cancer Registry is very difficult to obtain. Thus, the true incidence and mortality rates for Kenya remain unknown. The number of patients presenting with esophageal cancer in Eldoret is high. This high number of patients in an almost always fatal disease, prompted us to review existing case information with a view toward defining the magnitude of the problem, establishing the groundwork for further studies into its etiology and developing locally appropriate screening and treatment strategies. This report describes the basic epidemiology of esophageal cancer in patients seen at Moi Teaching and Referral Hospital, in the North Rift Valley of Western Kenya in the years 1994 - 2001. MTRH is a referral hospital situated in North Rift Valley of Western Kenya. AIM The main aim of this study was to determine the incidence and distribution of esophageal cancer in the North Rift region of Western Kenya which forms the patient catchment areas of Moi Teaching and Referral Hospital, Eldoret. OBJECTIVES The specific objectives were: i) To analyze esophageal cancer patients' records data in order to determine the gender, age, ethnic groups as well as the geographical distribution MATERIALS AND METHODS All the 468 patients in this study who presented at Moi Teaching and Referral hospital in Eldoret between 1994 and 2001 were drawn from Western Kenya. This retrospective study involved review of all available pathology reports from the time period beginning January 1994 and ending May 2001. All the cases were confirmed on the basis of histological diagnosis. The incidence rate is calculated from 1998 to 2000 as our records before 1998 are not complete and the Eldoret Cancer Registry is still updating records from year 2001 - 2003. The study was carried out at the Moi Teaching and Referral Hospital which is situated in a rich farming highland with an (altitude of 2000 metres above sea level)area in the North Rift Valley of Western Kenya. It serves a population of over 4.5 million people. It has a bed capacity of 500 patients and this capacity is rapidly expanding. The MTRH was upgraded from Eldoret District Hospital to a teaching and referral hospital by an act of the Kenya Parliament in 1990. The MTRH has a cancer registry which was formally established in December 1999 with the support of the International Agency for Research on Cancer; Lyon France. Data collection and analysis All reports of esophageal malignancy were obtained and data on gender, residence, age and tribal background was abstracted and recorded. Statistical analysis was performed using the SPSS software package. All tests were two-sided and statistical significance level was set at alpha=0.05. Comparison of means and proportions were done using the Wilcoxon test and the chi-square test respectively. RESULTS We reviewed of all malignancies as compared to cancer of esophagus. We considered only records of patient whose tribal data was available in Eldoret Cancer registry. The results from Eldoret Cancer Registry of MTRH for the three year period 1998 - 2000 show that, in this highland area, cancer of esophagus is the most common cancer of men. The most common cancers in men in this area in the descending order were oesophagus, Lymphomas, Prostate, Liver and Stomach (Table 1). The Annual Specific Rate (ASR) of 24.5 per 100,000 in men is moderately high for esophageal carcinoma. In women it is third in frequency compared to other cancers like cervix, breast, ovary, uterus and liver cancer. The incidence rate of cancer of esophagus in women is around half that of men (Figure 1). The 468 cases of esophageal cancer seen during this period accounted for 13.8% of the total neoplasms (3400 cases) seen from Jan 1994 to May 2001. Of these 468 confirmed cases, 290 cases occurred in males and 178 occurred in females, a male to female ratio of 1.5:1. The youngest patient was 20 years and the oldest patient was 96 years. The mean age was 58.69 years and the distribution of cases according to age is shown in (Figure 2). Most of our cases were of age between 50 to 70 years. The difference in mean age at presentation between males and females was not statistically significant (p-value=.653). There were a sizable number of young patients in this group, with 30 (10%) of all cases of esophagel cancer occurring in patients less than 40 years of age. The tribal origin was known in 468 cases and the breakdown is given in (Figure 1) Twenty percent of these patients died during their first admission at the hospital and the probability of dying in hospital was similar for all the tribes (p-value=.297). The probability of dying in hospital was not different between the sexes (p-value = 0.754). Squamous cell carcinoma accounted for 90% of the cases that had histology results. The occurrence of cancer of the esophagus according to site were: lower third 32 cases, middle third 31 cases, and upper third 17 cases. However there was a high number of cases which were unknown. This was so due to the fact that many of the surgeons and pathologists did not indicate the site from which the biopsy or autopsy was taken. All the cancer of esophagus cases analyzed were based on confirmed histology reports. The incidence rate of cancer of esophagus in males rose rather sharply between 1997 and 1999. It however showed some decline between 1999 and 2001 and then remained steady through 2002. There was a sharp decline in the incidence rate of cancer of esophagus in females from 1997 to 1998, followed by a sharp rise between 1998 and 2000. This was followed by a sharp drop, then the incidence rate remained steady between 2001 and 2002 (Figure 3). The risk factor associated with esophageal cancer in this area as indicated from the files were alcohol and smoking. However there were also cases of esophageal cancer in people who have never taken alcohol nor smoked cigarettes in their lifetime. DISCUSSION Patient characteristics Esophageal cancer is not a new disease and it has been with us since quite some time. Its incidence rate has soared recently due to the presence of experts and the improved hospital facilities to diagnose the disease in our area. It is our belief that the presence of experts or a particular relevant facility in an area is responsible for creating an "epidemic". Esophageal cancer is the most common cancer in this part of the Rift Valley Province in Western Kenya. This finding is similar to the earlier observations of Ahmed and Cook2 but is different from the report of Gatei et al3 which was based on less complete case ascertainment. Further, our data suggests that the incidence of esophageal cancer in this area is high. The Rift Valley was previously considered as a low incidence area. However our observation is that it could be a 'hot spot' for esophageal carcinoma. The male: female ratio among esophageal cancer patients was approximately 1.5:1. This sex ratio is more or less similar to that found in other populations at a high-risk for esophageal cancer, including 1:1 in the Karakalpakstan region of Uzbekistan8, 1.4:1 in Linxian, People's Republic of China9 and 0.85:1 in the Gonbad region of Iran 10, but is lower than that found in low-risk regions for esophageal cancer, such as 3.0:1 in Lithuania11, 4.6:1 in the European Union12 and 2.4:1 among US whites13. It is therefore not very surprising that in our population both the male and the female are affected at more or less the same rate. This may be due to the fact that males and females are more or less exposed to the same risk factors in this environment. The median age at diagnosis was 58.7 years, consistent with published reports in other high-risk population14,15. Clinical Features Dysphagia and weight loss were the most common presenting symptoms, in keeping with a wide series of published reports. In fact, weight loss combined with dysphagia was almost always pathognomonic of this cancer. Vomiting and chest pain were also very common presenting complaints. Although hematemesis has been reported by others to be quite common9,16, we did not see any patients with this complaint. The lower third of the esophagus was the most common location for tumors, followed closely by the middle third. In comparison to other case series in Kenya, our localization of tumors is consistent with the findings of Gatei et al9 but is quite different from that of Nevill17. The preponderance of squamous cell carcinomas over adenocarcinomas and the late tumor state at the time of presentation are in keeping with virtually all other published reports from endemic regions18. Risk factors The graph of the incidence rate pattern of cancer of esophagus in this area shows that both males and females seem to be exposed to the same putative agents. However the incidence in female remained lower than that in males. Our study does not involve a detailed evaluation of risk factors for the development of esophageal cancer in the MTRH population, but an examination of known risk factors will be beneficial in future studies. Excessive use of tobacco and alcohol has clearly been shown to be a risk factor for this condition19. In fact, it is estimated that 90% or more of the risk of esophageal cancer in Western Europe and North America can be attributed to tobacco and alcohol18. Family history has also been shown to be relevant in some high-risk areas. A study in Shanxi Province, China, found that families who have a prior history of esophageal cancer were significantly more likely to have reported a new case during 10 years of follow-up20. The population at highest risk for esophageal cancer, in northern China, Iran and South Africa rely heavily on corn or wheat as their dietary staple3,9. The inhabitants of this area typically consume maize at every meal. Several hypotheses have been raised regarding the link between maize consumption and esophageal cancer. One hypothesis suggests that increased risk it derived from nutritional deficiencies, which are often seen in diets composed mainly of cereal grains. Dietary deficiencies in vitamins A, C, E, selenium and zinc have all been suggested as factors in the development of esophageal cancer21, 22. A second hypothesis proposes that the reliance on maize increases exposure to the mycotoxin fumonisin, produced by the commonly occurring maize mold Fusarium moniliforme Sheldon. Fumonisins in association with nitrosamines have been shown to be statistically correlated to the prevalence of esophageal cancer in the Eastern Cape, a high incidence area of esophageal cancer in Southern African23 and China24. Maize is the staple diet for our population. They also take a locally brewed beer called 'busa', which is made of maize (maize and millet) that may not be free from moulds. Although several etiological studies have supported this hypothesis23,24, a recent nested case-control study conducted in northern China failed to find an association between a biomarker of fumonisin exposure and risk of esophageal cancer25. Drinking of a malt has been associated with increased risk of esophageal cancer in South America, but only when consumed at a very high temperature26. It is thought that the high temperature causes cancer through repeated thermal injury. Although data on tea consumption was not collected in our study, tea drinking is very common in the Western region of Kenya and the temperature of the consumed tea can be high. Human Papilloma Virus (HPV) infection is another potential risk factor for esophageal squamous cell carcinoma. HPV is the primary etiologic agent in cervical squamous cell carcinoma. Four case-control studies have examined the risk of esophageal cancer associated with HPV infection, and 3 of the 4 found significant positive associations27, 28. There is currently no consensus on the importance of HPV in the etiology of esophageal squamous cell carcinoma. Cervical cancer was among the top most common cancers seen at MTRH in our series suggesting that HPV infections are common. Polycyclic aromatic hydrocarbons (PAHs) are known carcinogenic agents. Ingestion of food contaminated with household smoke or soot particles has recently been suggested as a possible route of esophageal exposure to PAHs and was common in the high-risk areas of northern China 5. Nearly all the people in this area are habitually exposed to smoke from cooking and heating fires as most homes in these communities do not have sufficient ventilation. Drinking of 'mursik' (fermented milk laced with charcoal powder) is also very common. 'Mursik' is a local beverage which is likely to be contaminated with PAHs as it contains some particles of charcoal from a special herb plant. The charcoal is ground and added to the container to flavor the milk. An additional factor, which may interact with this exposure, is genetic variation in the enzymes responsible for the metabolism of PAHs. Although this has not been examined in our population, other studies have reported that smokers who are homozygous for the rapid metabolizing allele (valine/valine) of cytochrome P4501A1 and are homozygous for GSTM1*0 are pron to increased risk of developing squamous dysplasia of the esophagus5. CONCLUSION The area surrounding MTRH in the Rift Valley Province of Western Kenya appears to be another region where esophageal cancer is endemic. In this area, esophageal cancer is the most common malignancy seen in both males and females and the incidence rate appears to be rising. The sex distribution shows a slightly higher male to female ratio, however more female cases were seen in the Kikuyu and the Nandi tribe. The Kikuyus have greater awareness of the disease than the Nandis. Patients presenting with this condition usually have obstructing lesions and are generally offered either surgical resection or endoscopic stenting, depending upon the individual condition of the patient. Our findings point to the need for further studies to ascertain the actual incidence rate of esophageal cancer, elucidate known and novel risk factors and to evaluate the feasibility of screening programs to find patients at earlier stages when appropriate treatment offers a reasonable chance of cure. Further work is also needed to develop appropriate palliative measures for those presenting at late stages. This study forms a preliminary basis of the work we intend to carry out to identify genes that are altered during the neoplastic process and examine their mutational pattern. This may lead to identification of molecular biomarkers to be used in future for the early detection of this neoplasm. ACKNOWLEDGEMENTS We wish to acknowledge the Institutional Research and Ethics Committee of Moi Teaching and Referral Hospital for permission to carry out this work. We thank the members of staff in the clinics, wards and Hospice for their support and co-operation. We thank the MHO Netherlands coordinator for encouragement. We thank the International Agency for Research on Cancer (IARC), Lyon, France for assistance in establishment of the Eldoret Cancer Registry and the registry staff. REFERENCES:
Copyright 2005 - Makerere Medical School, Uganda |

{kind=link}
{kind=link}
{kind=link}
{kind=link}