 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 5, No. 2, June, 2005, pp. 164-167 Aetiology of low back pain in Mulago Hospital, Uganda Moses Galukande, Stephen Muwazi and Didace B. Mugisa Makerere University, Faculty of Medicine, Department of Surgery, Kampala, Uganda Code Number: hs05030 ABSTRACT Background: Low back pain exists in epidemic proportions in
the western world and is on the increase. Its cause is mostly nonspecific.
Not much is known about it in the developing world because the data is scanty.
This study was set out to investigate the possible causes of low back pain
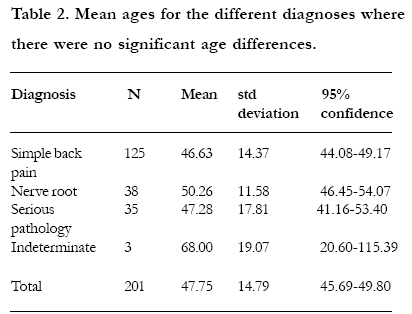
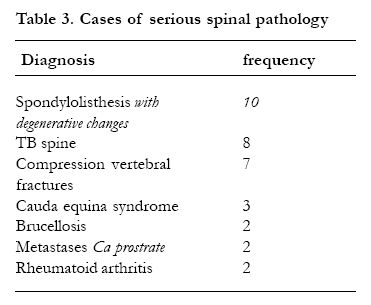
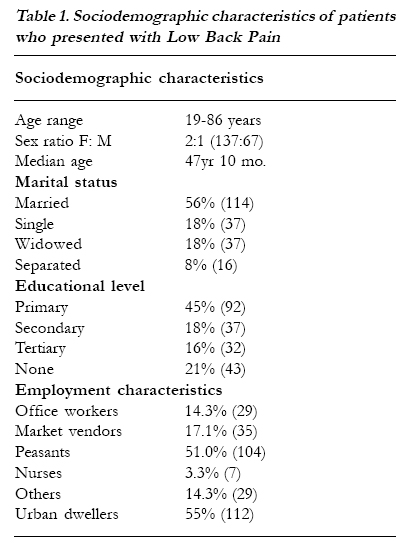
and prevalence. Back pain has affected humans through out recorded history. The oldest surviving surgical text, the Edwin Smith papyrus from 1500 BC, includes a case of back strain. Two key ideas in the nineteenth century laid the foundations for the modern approach to back pain: That pain came from the spine; and that it was due to injury. There is however no evidence that back pain has changed. The symptom of back pain appears to be no different and no more severe than it has always been. What has changed is how back pain is understood and managed 1 and may be its prevalence 2. Low back pain exists in epidemic proportions in the western world and is on the increase there.2 Data from the developing world is scanty. The literature on its epidemiology from the high-income countries is accumulating yet they comprise only 15% of the world population.3 The little there is about epidemiology has come from Nigeria, Southern China, Phillipines and Kenya. The prevalence ranges from 0% to 16%3,4,5,6. The aim of this study was to explore some aspects of low back pain in the developing world setting and contribute to scanty literature available and hopefully improve on our understanding. The objective was to investigate the aetiology of low back pain and its prevalence in Mulago, Uganda’s national referral and teaching hospital. METHODOLOGY Study design This was cross sectional descriptive study. 204 patients enrolled out of 1033, were subjected to a questionnaire, which included history taking, physical examination and investigations. Study subjects This study was carried out in the outpatient orthopedic clinic of Mulago hospital, the national referral hospital, in Uganda. Patients came mostly from Kampala, Mpigi and Mukono districts. These are in the central part of the country and closest to Mulago hospital. From the 1033 general patients that presented to the clinic during the seven months period of study, 204 were recruited. All these 204 patients had been referred to the clinic with low back pain as a major complaint and were above 18 years. Assessment Consecutive new consenting adult patients referred with low back pain as the major complaint were seen in the consulting room one at a time. A detailed history guided by a questionnaire included the details of pain, its site, its radiation; duration, aggravating factors, and variation with time and activity were taken. The past medical, surgical, obstetric and gynecological histories were taken. Physical examination was done for each patient starting with the general and examining all the systems. Weights and heights were recorded. The examination also included straight leg raising, muscle power assessment, reflexes and sensation. All patients took a plain lumbosacral Xray and a full blood count and ESR. Other investigations such as abdominal ultrasound scans, Computerized Tomography myelograms, Chest Xray, Brucella titres, Computerized Tomography guided Trucut Needle biopsy and histopathological analysis was ordered depending on the leads from history and physical examination as stated in the Clinical Standards Advisory Group, 1994 London diagnostic triage Algorithm. Patients below 18 years and those with non-spinal pathologies such as renal, abdominal or gynecological pathologies were excluded from the study. Sample size, Data processing and analysisSince the prevalence for sample, nerve root and serious back pain was not known, prevalence P was taken to be 50% which gives the biggest simple size. Kish and Leslie formula was used. A review of the records indicated that 428 patients with Low back pain were seen the previous year so N was taken to be 428 therefore giving a sample size of 202. The data was entered using Epi info software and analyzed using SPSS for windows version 10. The analyzed data was presented in frequency tables for categorical valuables. Means and standard variations were used to summarize continuous variables. P value was considered statistically significant if equal or less than 0.05. RESULTSThe point prevalence of low back pain was 20%. Of the 204 patients studied, 62.3% had simple (Mechanical) low back pain with no definable patho- anatomic causative factors identified. Of the patients 19.1% had nerve root compression secondary to prolapsed inter vertebral discs. A further 17.2% suffered serious spinal pathology as shown in tables 2 and 3. In 1.5% the diagnosis was undetermined. There were no statistically significant age and gender differences among diagnoses. (p = 0.057) Nerve root entrapment was more common in women though it was not statistically significant. (Table 1) DISCUSSION The term low back pain (LBP) as defined by Andersson and used in most surveys is defined as pain limited to the region between the lower margins of the 12th rib and the gluteal folds.7 Classification or categorizing of LBP has been varied making comparison of studies difficult. The one used in this study has 3 categories: simple back pain, nerve root compression and serious spinal pathology. It is mostly useful and more appropriate for clinical settings.1, 13, 14 Prevalence is used as an epidermiologic measure of LBP; the respondents report pain at the time of administration of the questionnaire. Other measures, besides point prevalence are reported in some studies such as annual or lifetime prevalence 3,15. Because point prevalence is the reported far more frequently in studies of low-income countries than these other measures .it serves as the most suitable basis of comparison between studies.3. Point prevalence has the added advantage that unlike other epidermiologic measures it is not based on recollection15, 16,17. This could be partly explained by the fact that this was a hospital based study as opposed to the reviewed studies that were community based. Or indeed it could be a true reflection of what is common in this society. Whereas nerve root compression is reported to be commoner in men, in this study it was seen more in women though it was not statistically significant. There was a significant gender difference with female: male ratio of 2:1.this is similar to Mulimba's findings in Nairobi, Kenya.6 Other studies 1, 18 showed no major or significant gender differences. Only a slightly higher frequency of back pain in women was reported, similar to most other bodily symptoms. Could this imply that women in our region/setting are more predisposed? Or they seek professional medical attention more than men? This deserves to be scrutinized further. The list of recognized causes of low back pain is vast in the numerous studies 19, 20, 21. In the literature review, simple back pain due to a non-specified cause accounted for over 90% of the etiology. The other name used to refer to nonspecific low back pain is mechanical low back pain. In this study it accounted for 62.3% of the patients. Nerve root pain or entrapment due to disc herniation or prolapse accounted for 19.1% .In the studies reviewed it accounted for about 5%. Serious spinal pathology due to various causes accounted for 17.1%. In others studies it accounted for less than 1%! 8,9,10 In the serious spinal pathology category infective processes accounted for 11 cases out of the 35.8 due to Tuberculosis (non pyogenic infection) and 3 due to brucellosis (pyogenic infection). In the literature Staphylococcus aureus was the commonest cause of pyogenic infection. It did not appear in this study. This reflects on the high burden of infectious diseases in the tropics. Such figures are not found in the literature reviewed from the western world. 11,12The second commonest cause of serious spinal pathology was spondylolisthesis with degenerative changes. This appeared with a mean age of 47 years. Rheumatoid arthritis contributed 0.1% compared to 6% in the literature. Rheumatoid arthritis is not as common a disease in Africa as in Europe or the rest of the western world. Low back pain is clearly an important health problem whose etiology is largely indefinable. The definable entities of nerve root entrapment due to disc herniation and the serious spinal pathologies due to various etiologies: infective, neoplastic, inflammatory and degenerative lesions are important. A systematic and logical approach to making a diagnosis is important through, history taking, physical examination, baseline investigations and specialized ones if indicated. There is need for research to establish the precise etiology of this large indefinable entity. Knowledge of precise aetiology may throw more light on management of individual cases and in designing preventive measures. For our region it is essential to further examine reasons why women seem to be more prone to low back pain. While managing low back pain, it is essential to consider infection processes which are not emphasized by literature from the western world. REFERENCES
Copyright 2005 - Makerere Medical School, Uganda |

{kind=link}
{kind=link}
{kind=link}