 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
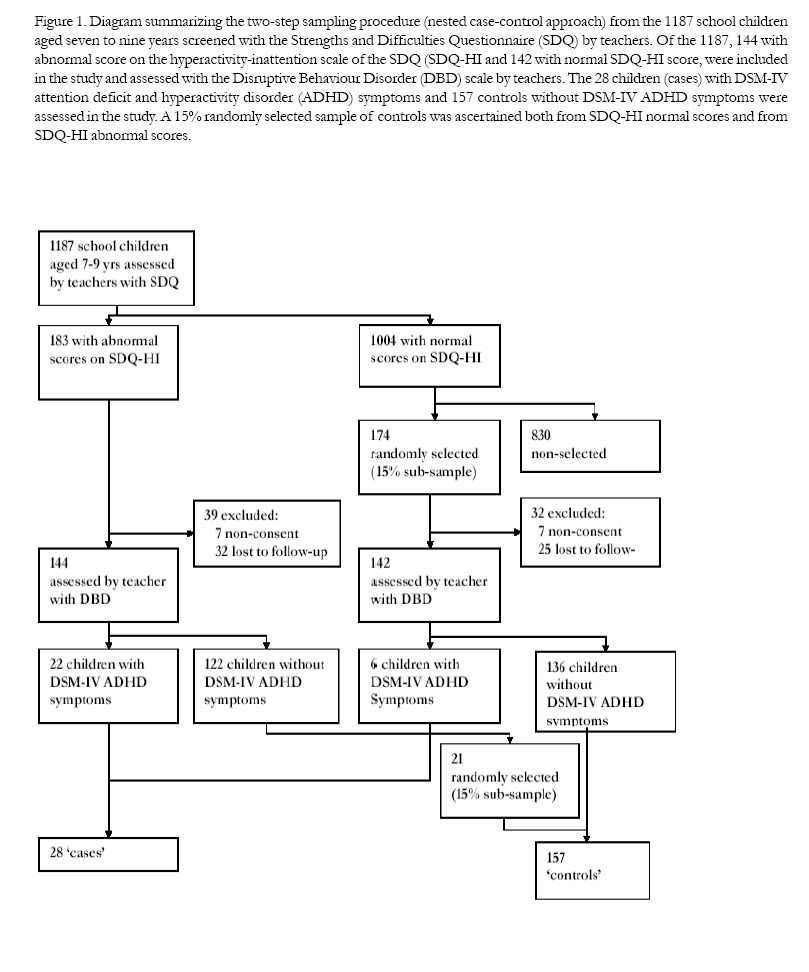
African Health Sciences, Vol. 5, No. 3, September, 2005, pp. 172-181 ORIGINAL ARTICLES Attention deficit and hyperactivity disorder among school children in Kinshasa, Democratic Republic of Congo Kashala E1, 2, Tylleskar T2, 3, Elgen I3, Kayembe KT1, Sommerfelt K3 1 Department of Neurology, Kinshasa University Hospital, Kinshasa, Dem. Rep. of Congo. Correspondence author: Espérance Kashala University of Bergen Center for International Health Armauer Hansen Building 5021- Bergen, Norway E-mail: esperance_Kashala@yahoo.com Phone: +47 55 97 46 92 Fax: + 47 55 97 49 79 Code Number: hs05032 AbstractObjectives: To estimate the prevalence and determinants of attention deficit and hyperactivity disorder (ADHD) symptoms among school children in Kinshasa, an African urban setting. Keywords: ADHD, DSM-IV, school children, risk factors. IntroductionAttention deficit and hyperactivity disorder (ADHD) is one of the most commonly diagnosed behavioural disorders in child and adolescent psychiatry in high-income countries in Europe and North America1 . Its prevalence varies between 2- 14% of school-age children2 . The variation in reported prevalence of ADHD may, in addition to real differences, be attributed to factors such as varying diagnostic criteria, and use of different diagnostic instruments and informants3 . To assess ADHD symptoms, different instruments based on the Diagnostic and Statistical Manual of Mental Disorders (DSM) have been used. Their psychometric properties appear to be generally good worldwide4 . However, most of them have not yet been systematically evaluated in Africa. Besides the role of neurobiological5 and genetic factors6 in the pathogenesis of ADHD, family environmental adversity may also play a role in the pathogenesis of the disorder. However, it is believed that it is the aggregate of psychosocial adversities rather than a specific family environmental factor that increases the risk for ADHD7 . In Africa, little is known about ADHD and its determinants. The few data available also indicate that it is one of the most prevalent disorders in childhood in African children8 . The present study was therefore conducted in order: 1) to estimate the prevalence of ADHD symptoms among school children in Kinshasa, and 2) to identify clinical and socio-demographic risk factors for ADHD symptoms in an African urban setting. Methods Study area A detailed description of the study area is given elsewhere9 . In short, the study was conducted in Kinshasa, which is the capital and largest city of the Democratic Republic of Congo (DR Congo). The city has a population of five million and is located in the Western part of the country, which is about 2-3 hours away by plane from the war-affected Eastern part of the country. According to the Ministry of Education, Kinshasa is divided into two sectors for administrative purposes, Kinshasa East and West, and comprises 24 municipalities. Since the country’s independence in 1960, efforts have been made to increase access to education. All children at six to twelve years of age are required to attend school, which is seen as a key for a better life. The schooling system is divided into three levels, which comprises primary level (six years), high school level (six years), and high learning institutions or universities (after the high school level). In primary schools, there is one teacher per class with an average of 30 pupils each. All schools in Kinshasa have school fees. The city has a high rate of adult literacy (89.5%) compared to rural areas (60%). Test materials Two behavioural instruments were used: the SDQ (Strengths and Difficulties Questionnaire, www.sdqinfo.com) and the DBD (Disruptive Behaviour Disorder rating scale)10. The Strengths and Difficulties Questionnaire (SDQ) is a brief questionnaire comprising 25 items divided between five scales yielding scores for emotional symptoms, conduct problems, hyperactivity-inattention, peer problems and prosocial behaviour. For each item, the respondent may answer, ‘not true’, ‘somewhat true’ and ‘certainly true’. The DBD is a rating scale based on both the third revised and the fourth editions of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III-R and DSM-IV)10. The scale consists of 45 items representing symptoms of Disruptive Behaviour Disorders that are conduct disorder (CD), oppositional defiant disorder (ODD) and ADHD. Of the 45 items, 18 are DSM-IV ADHD symptoms criteria. Only these 18 items were used in the present study. Each symptom is rated on a 4-point scale indicating the occurrence and the severity of symptoms: 0 (not at all), 1 (just a little), 2 (pretty much) or 3 (very much). The scoring was done according to the symptoms counting method given by Pelham10. According to the DSM-IV, ADHD is divided into three subtypes that are predominantly inattention (ADHD-I), predominantly hyperactivity/ impulsivity (ADHD-HI) and combined (ADHD-C). ParticipantsThe subjects included in the present study were all eligible school children aged seven to nine years old recruited from 10 randomly selected schools. A step-wise cluster sampling procedure was used: initially six out of 24 municipalities were randomly selected. From the selected municipalities, a list of all primary schools was established. From this list consisting of 30 schools, 20 schools were randomly selected of which 10 consented to participate9. All the 1187 eligible school children aged seven to nine years old were included and screened by their teachers with the SDQ (Figure 1). This screening yielded abnormal scores on the hyperactivity-inattention scale of the SDQ (SDQ-HI) for 183 children, and normal SDQ-HI scores for 1004 others. In the latter group, a random 15% sub-sample yielded 174 control children. Of these 183+174 children, 71 were excluded due to non-consent or loss to follow-up (39 with abnormal SDQ-HI scores and 32 with normal SDQ-HI scores). The remaining 286 school children (144 with abnormal SDQ-HI score and 142 with normal SDQ-HI score) were assessed by teachers using the Disruptive Behaviour Disorders rating scale (DBD, Figure 1). The DBD assessment yielded 28 school children that fulfilled the DSM-IV ADHD criteria (‘cases’) and 157 children, who did not fulfil the criteria (‘controls’). Of the 28 cases, 22 had an abnormal SDQ-HI score and 6 did not. To make the final control group comparable to the original population of 1187 children regarding normal SDQ-HI score vs. abnormal SDQ-HI score – that is to avoid a potential selection bias from the preceding SDQ screening – a random 15% sub-sample was selected also from the group with abnormal SDQ-HI score, but DBD negative: This resulted in 21 randomly selected children, added to the 15% randomly selected sub-sample of 136 with normal SDQ-HI score and without DSM-IV ADHD symptoms (i.e. DBD negative) (Figure 1). The procedure can be regarded as a nested case-control procedure. Study procedureThe project protocol was approved by The National Medical Council in DR Congo and The Regional Ethics Committee on Medical Research in Norway. The collaboration and informed consent obtained from the head masters, teachers and parents’ committee before the project started facilitated re-contacting the teachers. Written informed consent was obtained from parents/caretaker. Prior to the interview, parents/caretakers of each selected child were officially contacted through the head master of the school to inform them of the interviewer’s visit and to request their consent to participate. When an agree-ment was met, all parents/caretakers were visited at home. In addition informed consent to examine each child was individually obtained from parent or primary caretaker during the interview. At the same time, teachers of selected children were re-contacted and asked to fill out the 18-items of DBD questionnaire for each participating child. Prior to the study, a pilot interview was performed with 30 individuials using the parents’ questionniare. This was done to ensure uniformity in the questionning technique and to refine background questions. Information from parents/caretakers was collected by a single interviewer in order to avoid bias in data collection. The interviewer was a graduate from the National Pedagogic Institute of Kinshasa and was trained in interviewing. He was specifically trained for five days with this particular questionnaire. A semi-structured interview with parents was performed using a questionnaire specially designed to assess the child socio-demographic characteristics and background. A questionnaire was designed to obtain the following information: 1) socio-demographic characteristics of the child, the family structure and the household composition; 2) maternal status: being the first wife or not; 3) living with both parents or single-parent home, are parents divorced, are both parents alive; 4) parents’ education and profession/ occupation; 5) parents’ age at child’s birth; 6) mother smoking or not during pregnancy; 7) perinatal factors (pregnancy, delivery, birth weight, neonatal period and child growth/development); 8) the child’s medical history and the presence of particular disorders in the family; 9) child’s global health (seeing and hearing difficulties, physical disability, child’s nutritional status), and socio-economic status as perceived by parents; 10) child’s school performance and learning disability as perceived by parents; 11) parents’ description of their child. The parts 9-10 consisted only of close-ended questions rated from 1 (non-optimal) to 3 (optimal) whereas the other parts had both close- and open-ended questions. In case of missing information during the first interview, the parents were contacted again a few days later to obtain the needed details. The parents and teachers’ response rate was 100%. Both the interviewer and the clinician were blinded to the child’s scores. All children underwent a complete standard clinical examination, including neurological assessment in a room specially prepared at school for that purpose. In addition, the visual acuity was measured by means of the Snellen chart and the hearing performance was assessed by asking the child if she/he has hearing difficulties and by clinical evaluation. A neuropsychiatrist (EK) blinded to the child’s background factors and to the SDQ-HI and scores, performed the clinical examination. The clinical examination and the observation of the child were performed with the main purpose of excluding other clinical, neurological and/or behavioural problems that could explain the presence of ADHD symptoms. The short version of the Examiner’s Rating Scale (ERS)11 was used in the observation of the child. A daily team meeting was held prior to the computer data entry in order to discuss and resolve problems or mistakes found. The major difficulty encountered was of logistic nature: tracing houses and change of addresses. In the present study, ADHD symptoms were defined as meeting the following two criteria:
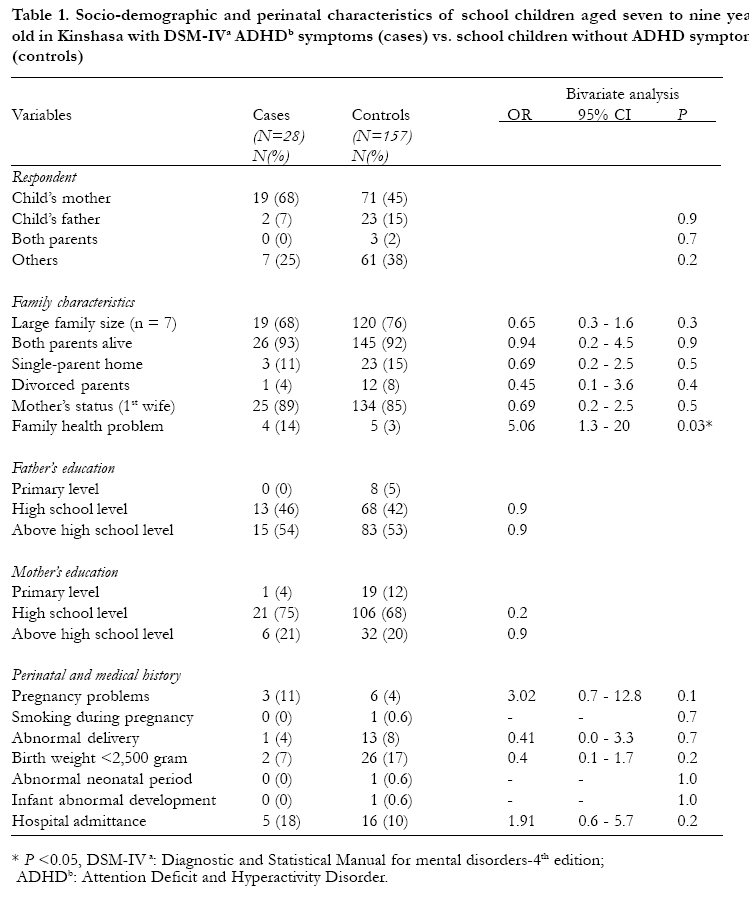
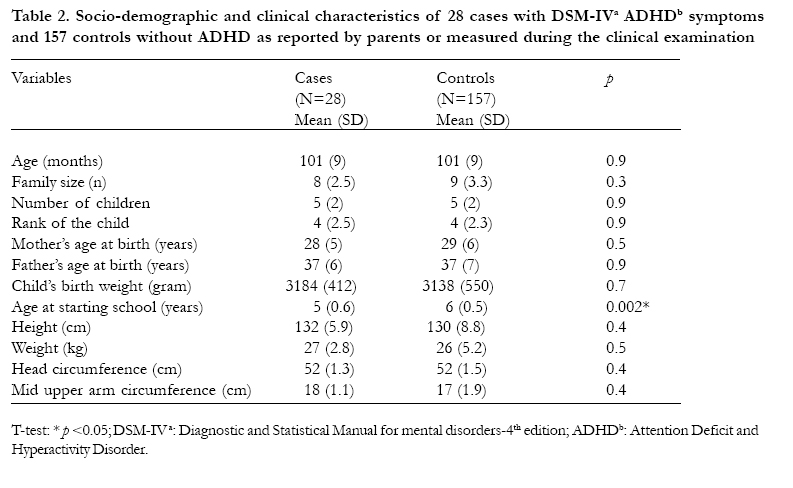
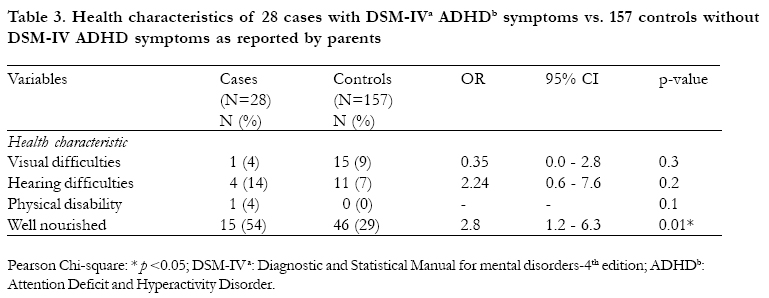
Statistical analysis We used the Statistical Package for the Social Sciences (SPSS) version 11.5 for data management. Mean group differences were compared using t-tests. Differences in proportions for outcome variables between groups were compared using Pearson Chi-Square and odds ratios were used as risk estimates. Fisher’ Exact Test was used when appropriate. Correlation and logistic regression were used for bivariate analyses. All tests were 2-tailed and the results were considered statistically significant when p-values were less than or equal to 0.05. Results Estimated prevalence of ADHD symptoms Out of the 286 school children (45% boys and 55% girls) evaluated with the DBD scale, a sub-sample of 185 school children was studied (28 were ‘cases’ reported by teachers with DSM-IV ADHD symptoms and 157 controls). Of these 28 cases, 15 (54%) were boys and 13 (46%) girls (OR: 1.8, 95% CI 0.8 to 4.1, p = 0.1). The mean age was 100 months (SD 9). No differences in gender or age distribution were found between cases and controls. ADHD-C was most frequent and seen in 24 (86%) school children followed by ADHD-I and ADHD-HI in 2 (7%) school children, each. Of these 28 children, 6 were identified among the 142 children with normal SDQ-HI score (4.3%) and 22 among the 144 with abnormal SDQ-HI score (15.3%). Assuming the same prevalence of DSM-IV ADHD symptoms among all children in the two groups (4.3% of 1004 and 15% of 183), estimated prevalence of DSM-IV ADHD symptoms among the general school child population is 5.9% (70/1187). Teachers’ report on children identified with both SDQ and DBDEach child was assessed by her/his own teacher. The number of school children assessed by one teacher varied according to the total number of pupils per class. The total number of school children identified with both instruments by teachers was 22/ 286 (8%). The risk of being reported with DSM-IV ADHD symptoms criteria was fourfold higher when previously reported with abnormal SDQ-HI score (OR: 4.1, 95% CI: 1.6 to10, p = 0.002). The Spearman inter-teacher correlation, using the SDQ and the DBD, was medium (rs = 0.2; n = 286; p = 0.001). The internal consistency of SDQ hyperactivity-inattention items and DBD, evaluated with the Cronbach’s alpha coefficient was 0.7 and 0.9, respectively. Respondents’ and family’ characteristicsParents were the principle respondents regarding child characteristics in more than 60%, the child’s mother being the main respondent (Table 1). Approximately half of the fathers had an education level above the high school (either high learning institutions or universities), whereas two thirds of the mothers had high school level of education. Half of the fathers were employees in the private sector whereas almost 60% of the mothers were housewives. Regarding the parents’ education level, no significant difference was found between the two groups (Table 1). Among the fathers of the 28 cases, 14 (50%) were working in the private sector, 13 (46%) in the public sector and one (4%) was unemployed. Eighteen mothers (64%) were housewives, seven (25%) were workers in the private sector and three (11%) were workers in the public sector. Similar proportions were reported among controls with no significant differences found between the two groups (Binary analysis for logistic regression p > 0.05). Overall, no significant difference was noticed between the two groups regarding the family structure (Table 1). The households included an average of eight persons, including an average of five children. Both cases and controls were on average the 4th born (t-test p > 0.05). According to the parents, more than 95% of the families (cases and controls) were classified in the middle socio-economic class (of three) (Binary analysis for logistic regression p > 0.05). It was found that the risk for ADHD symptoms according to the DSM-IV criteria was five fold when a family health problem was reported either among siblings or parents (Table 1). The health problems reported were sickle-cell anaemia, hypertension and diabetes. Perinatal and medical historyIn general, no significant differences were found between cases and controls regarding parents’ age at child’s birth or perinatal factors. Smoking during pregnancy was reported only by one mother in the control group (t-test p > 0.05). Pregnancy, child’s birth weight, neonatal period and infant development were normal for more than 95% of the children, both groups being comparable. Child’s birth weight was comparable in the two groups (Table 2). The proportion of children that had ever been admitted to a hospital was also comparable in the two groups (OR: 1.9, 95% CI: 0.6 to 5.7, p = 0.23). Parents’ description of their child and its school performanceWhen asking the parents to describe their children, among cases, about half of them, 13/28 (46%) were described as rowdy, whereas among controls only a quarter of them 43/157 (27%) were described as such. The mean school performance was significantly lower among cases compared to controls, 2.0 (SD 0.5) vs. 2.4 (SD 0.5) (t-test p < 0.05). Furthermore, cases were significantly younger at start of primary school compared to controls (Table 2). Child’s general health The proportion of children with seeing, hearing problems, or physical disabilities as reported by parents was comparable in both groups (p > 0.05). Surprisingly, cases were reported with a significantly better nutritional status than controls (Table 3). In general, the standard clinical and neurological examination was normal for all children (p > 0.05). The mean height, weight, head circumference and left arm circumference was comparable in both groups (Table 2). After the blinded clinical examination and the blinded observation, presumed psychopathologic conditions (ADHD, difficulties in sustaining attention, over-activity or anxiety) were made for 53 (29%) children. In this completely blinded clinical examination and observation, 17 of the 28 cases (61%) were identified with either suspect ADHD symptoms (7), hyperactivity (4), inattention (1) or other psychological problems (5). Discussion This is one of few studies aimed at estimating the prevalence of, and socio-demographic risk factors for ADHD symptoms among school children in an African urban setting. The two major findings of the present study were: first, a prevalence estimate of DSM-IV ADHD symptoms of 6% among a large, randomly selected group of school children aged seven to nine years in Kinshasa, similar to that found in high-income countries; second, the family structure, parent’s education, pregnancy, pre-and perinatal period, infant development, general health and socio-economic status were not correlated to DSM-IV ADHD symptoms. In Africa there is a lack of studies on the prevalence of ADHD, and its determinants. One study from Ethiopia, reports a prevalence of 1.5% that is lower than the one found in the present study12Furthermore, in accordance with our findings, they did not find specific determinants for ADHD apart from that older children and those living in urban areas were more at risk than younger children and those from rural areas13. Also, our study used a younger age sample and was limited to the urban area. The estimated prevalence of DSM-IV ADHD symptoms of 6% is in accordance with reported prevalences of 2 to 14% among schoolage children from other parts of the world2. In contrast to previous studies, where the ADHDpredominantly inattention subtype was the most common14, we found the ADHD-combined subtype to be more prevalent. In addition, no gender differences were found. The lack of gender differences may be related to the predominance of the combined subtype. Indeed, girls are more often considered to be less overactive than boys, therefore more likely to be underestimated. In the ADHD combined subtype, both the hyperactivity and inattention are present and the chance to be identified may be similar for boys and girls. According to Biederman et al., the risk for ADHD is the same for boys and girls15. The variation in the estimated prevalences of ADHD across studies is probably mainly due to use of different diagnostic approaches3. Some studies have reported an estimated prevalence based on results from either teachers or parents reports alone14. However, other studies have used a twostage design to estimate the prevalence of ADHD16The first stage involves a population-based sampling using behavioural screening tools completed by either parents or teachers, or both. In the second stage, those screened positive and a sub-sample (10-20%) of those who screened negative are recruited for a more detailed assessment. In the present study, we used a two-stage design, which allow us to consider our estimate close to the reality. How robust is this estimate? It comes from a large study of randomly selected children in a multiethnic urban setting in Africa, which is clearly an advantage. But it is based exclusively on school children. A populationbased estimate could be different, as 25% of the school age population are not attending school in Kinshasa. In the lower grades, like in this study population, attendance is somewhat higher but this study clearly is not giving a population-based estimate. One would suspect ADHD children to be drop-outs from the school more often than not so that the true prevalence would probably be. somewhat higher than our estimate. There is therefore a need for further similar studies in rural settings and with population-based samples to determine the prevalence of the disorder among school aged children. The internal consistencies of SDQ and DBD, evaluated with Cronbach’s alpha coefficient were high, 0.7 and 0.9, respectively. These findings indicate that both instruments can be considered reliable in this population. Indeed, a previous study using the DSM-III diagnostic criteria found these to be useful for psychiatric research in the DR Congo, formerly Zaire17. According to the present study, the SDQ may over-report hyperactivity-inattention symptoms in African school children. Therefore, on the basis of the present study, it would be more effective to use a tool such as the DBD as the primary tool when looking for ADHD instead of first screening with a broad range questionnaire such as SDQ. Although half of the respondents were the children’s mothers with more than 80% being the first wife, neither the respondent relationship with the child nor the maternal status were associated with the outcome. This may indicate that non-maternal main caretakers do not increase the risk of ADHD. Adverse family environmental factors have been found to predict behavioural disturbances in several studies. However, it may be the aggregate of adversity factors, which are associated with behavioural disturbance7. In the present study, we were unable to find any association between adverse background factors and DSM-IV ADHD symptoms. These results are in line with those from Ethiopia where no socio-demographic correlates were found for ADHD among children13. This may be. explained by absence of such explanatory mechanisms in this population, or lack of identification of the appropriate environmental risk factors. Also the lack of variability in the studied sample may have contributed to the lack of significant association. Indeed, different findings may have been observed if children non-attending school or those from lower socio-economic status were equally represented. Large family size has been found to be a risk factor for mental disturbance in several studies18. No such association was found in this study even though the majority of children were from large families. These results are consistent with those from Ethiopia where large and extended family sizes were found protective for mental distress19. Also our findings are in line with the study on American children from Caucasian and non-Hispanic families that found no association between birth order, family size and ADHD20. Behavioural problems are known to be more common in pre-term children of low birth weight (LBW)21. Term children with LBW (small for gestational age) in Western countries do not have an increased frequency of behavioural problems22. Since all LBW children in the present study were term, our findings are in correspondence with previous research from Western countries. Only one child was classified in the VLBW category and none in the extremely LBW (ELBW: <1000g). Therefore the association could not be evaluated in these categories of LBW children. The affective quality of the home environment, including parental expressed emotion, may predict ADHD symptoms23. In the present study, family health problems in the form of sickle cell anaemia, hypertension and diabetes were related to DSM-IV ADHD symptoms. In the DR Congo, health care is not subsidised by the government. Therefore having a family member with such a chronic disease is a heavy burden. Parents who are facing such problems may also have their mental well-being affected, which may influence the affective climate at home. This may explain the relationship found in the present study. However, the impact of family health problems on the parental emotion or affective quality of the home environment could have been better understood if a life event instrument to evaluate the mental well-being of parents had been used 24. School performance requires persistence in work-related tasks, sustained attention, mental effort, behavioural restraint and adaptation to rules. These conditions are known to worsen ADHD symptoms25, which will therefore affect the school performance and adaptation. In accordance with other studies, we found that school performance was lower among cases26. However, school performance is also related to other factors such as environmental factors, family relationship or depression. Indeed, depression in children might be a cause of poor school performance27. Nevertheless, during the clinical observation of these children, none of them presented behaviour suggesting a depression condition. In addition, the proportion of children reported with an abnormal emotional score in the screening was comparable. This finding may support the presence of ADHD symptoms as causation for poor school performance in the present study. Inattention or hyperactivity symptoms may be induced by diverse clinical and psychopathologic conditions3. In the present study, none of the children were identified with somatic or psychopathologic conditions that could explain the presence of ADHD symptoms. The clinical examination performed in all selected school children was normal. Therefore, the identified symptoms could be attributed to the ADHD status. LimitationsThe limited power (only 28 cases) and the lack of variability in our sample – i.e. non- school attendants or rural children not included – limit the generalisability of the present findings. In addition, teachers were the sole informants to assess DSM-IV ADHD symptoms. However, teachers are considered as particularly valuable source of information in diagnosing ADHD2. The age of onset criterion for symptoms was not evaluated. Indeed, it is often impossible to recall the age of onset of symptoms. The DSM-IV age of onset criterion has raised controversy and some authors suggest its revision28. It could be argued that it would have been useful to have a more extensive psychiatric evaluation of the children in the present study to make the ADHD diagnosis more certain. Electroencephalogram investigation could have helped identify specific aetiology such as undiagnosed epilepsy as an explanation for ADHD in a very small number of children in the present study. Indeed, temporal lobe dysfunction as in complex partial seizures may lead to hyperactivity and aggressive behaviour. However, such investigation has not proven very useful for ADHD diagnosis in high-income countries29. ConclusionThe current study indicates that DSM-IV ADHD symptoms are as common among school children in Kinshasa as elsewhere. The risk factors for ADHD, such as large family size, single-parent home, parents’ level of education, usually described in other studies were not found in the present study. This difference may be attributed to a protective role of an extended family on child mental health. However, family health problems and poor school performance were associated with DSM-IV ADHD symptoms. The present results suggest the need of more investigations including extensive neuropsychiatric evaluation to better understand ADHD in the DR Congo. AcknowledgementsThe authors thank all the parents, head masters and teachers for their kind collaboration. We are also grateful to the interviewer José Kalambayi for his commitment throughout the project and to all children who kindly accepted to be involved in the study. The Norwegian Educational Loan Fund and the University of Bergen, Norway funded the study. References
Copyright © 2005 - Makerere Medical School, Uganda |

{kind=link}
{kind=link}
{kind=link}
{kind=link}