 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
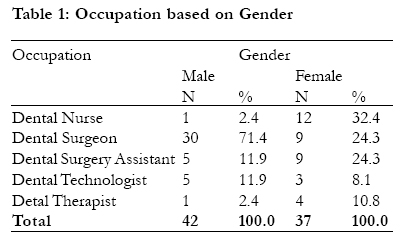
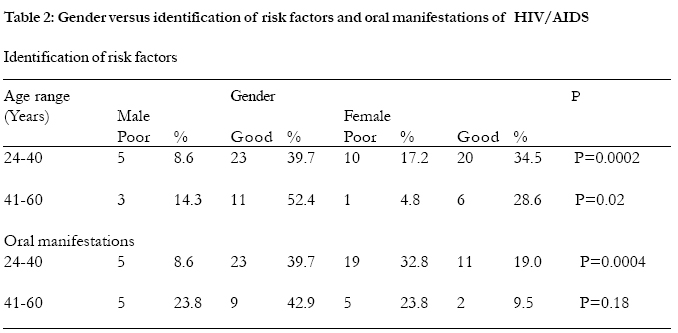
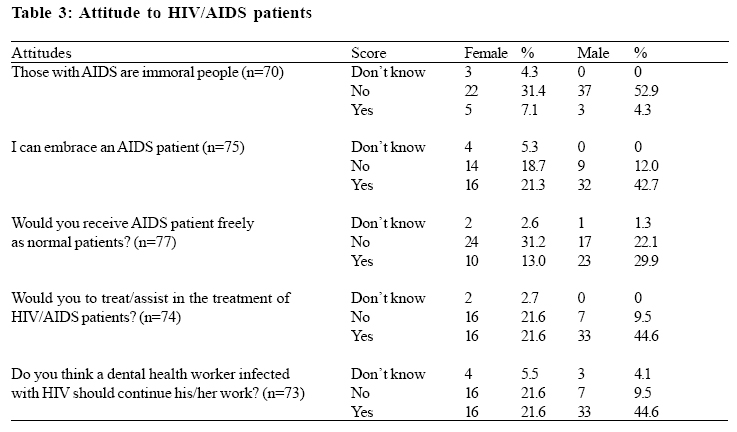
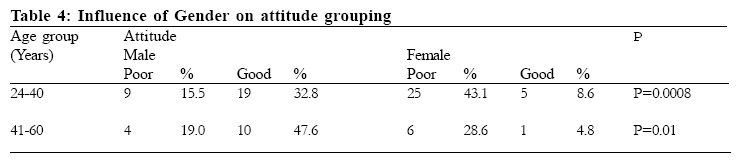
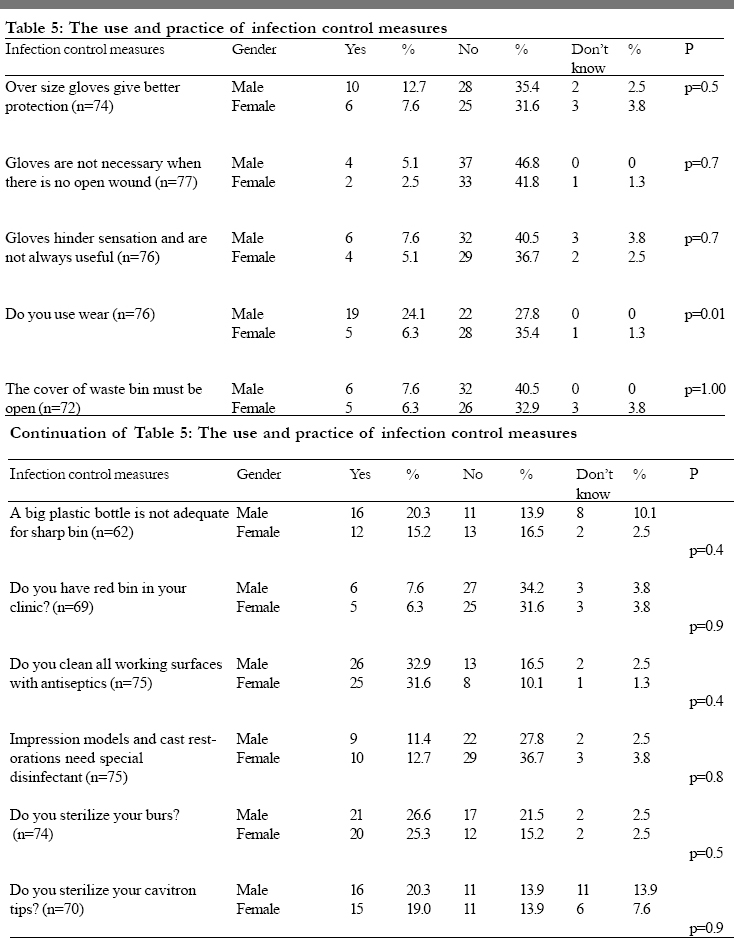
African Health Sciences, Vol. 5, No. 3, September, 2005, pp. 182-187 Gender differences among oral health care workers in caring for HIV/AIDS patients in Osun state, Nigeria Adedigba MA1, Ogunbodede EO1, Fajewonyomi BA2, Ojo OO3 and Naidoo S4 1 Preventive Dentistry Department, Faculty of Dentistry, Correspondence author: Dr. Adedigba M.A., Preventive Dentistry Department, Obafemi Awolowo University, Ile-Ife, Nigeria. E-mail: adedigba@oauife.edu.ng Code Number: hs05033 SummaryThe study investigated the relationship between gender and knowledge, attitude and practice of infection control among oral health care workers in the management of patients with HIV/AIDS in Osun State of Nigeria. It was a cross-sectional survey using 85 oral Health care workers (OHCWs) enlisted in the public dental health clinics. A self-administered questionnaire was designed and used for data collection. A total of 85 questionnaires were distributed. The response rate was 93%; 42 (53%) were males and 37 (47%) females. The majority of the respondents were in the 25-40 year old age group and the mean age was 37.3 years. Key words: Gender difference, Oral health workers, HIV/AIDS. IntroductionThe Acquired Immune Deficiency Syndrome is the major cause of death in Africa today, and it is estimated that 80% of the over 40 million people living with HIV/AIDS worldwide are residing in sub- Saharan countries1 . In Nigeria, AIDS was first reported in 1986 following the positive diagnosis of a 13 years old hawker. Since that time the epidemic has been on the increase with about two million infected in 1997 2 . The sentinel survey of 1999 reported a prevalence of 5.4%3 and that had increased to 5.8% by 20021. These low figures may be deceptive as many of the samples in these surveys were recruited from hospital-based environments4 , 5 and many of the HIV/AIDS patients might have died undiagnosed in other settings. Many secondary level health care facilities record up to 20 cases of HIV/AIDS weekly, while 40% of bed occupancy in others are as a result of AIDS related diseases 2 .The oral manifestations of HIV infection include fungal, viral and bacterial infections. Oral lesions such as candidiasis, herpetic ulcers and Kaposi’s sarcoma are among the first symptoms of HIV-infection. These conditions cause pain, discomfort, eating restrictions and provide a constant source of opportunistic infection. Early detection of HIVrelated oral lesions can be used to diagnose HIV infection, elucidate progression of the disease, predict immune status, and can result in timely therapeutic intervention. The treatment and management of oral HIV lesions can considerably improve well-being of such patients. Oral health care workers (OHCWs) have an important role to play in the overall health care delivery to patients with HIV/AIDS. There have been many reports in the literature reporting on the attitude and practice of oral health care workers and the care of HIV/AIDS patients 6-11 and many documented differences between male and female respondents. Moretti et al., (1992) 8 reported gender differences among OHCW with respect to their attitude to HIV/AIDS. Similarly significant differences between gender of OHCW and practice has been observed showing that male respondents were more compliant to the universal cross-infection control than their female counterparts 8 . In view of many studies that has been done on knowledge, attitude and practice (KAP) of OHCW worldwide very few are carried out in the sub-Saharan African region and in particular on gender differences among OHCWs. There is a need to determine gender differences among OHCW in order to draw appropriate conclusion and make adequate measure to alleviate these differences so as to make the OHCWs render adequate and appropriate care to HIV/AIDS patients in our community. Many researches centre their conclusion and recommendations on the general observation of OHCWs and not particularly addressing KAP issues based on gender. A study design to determine gender differences among OHCWs on management of HIV/AIDS patients will properly guide oral health educators in designing an appropriate intervention to alleviate this problem. This call for the relevance of this present study in presenting discernible differences among OHCWs. The aim of this study was to investigate the relationship between gender and identification of HIV/ AIDS risk factor, attitude and practice of infection control among oral health care workers. Material and Methods This was a cross-sectional study. The study population consisted of all the 85 oral health care workers enlisted in public dental health clinics in Osun State of Nigeria. A self-administered questionnaire was designed and used for data collection. It covered demographic factors, general knowledge on HIV/ AIDS expected of OHCWs, universal infection control practices and continuing education issues. The survey respondents were assured of confidentiality. A total number of 85 questionnaires were handed-in by the researchers and responses were retrieved by hand about a week later. This was done to avoid the problems with postal services. Measurements of variables: For the purpose of ease of analysis the attitude of OHCWs to HIV/AIDS patients was grouped into two: those with scores 0-3.0 as ‘poor’ and those with scores four and above were regarded as ‘good’. Ability to identify HIV/AIDS risk factors was grouped into ‘good’ (scores 15-28; >50%) and ‘poor’ (scores 0.0-14; <50%) while ability to recognise oral manifestations of HIV/AIDS lesions was also grouped into ‘good’ (scores 4-6;/50%) and ‘poor’ (scores 0-3; [50%). The questions raised in the questionnaire were simple, basic and general knowledge for all categories of OHCWs. We assumed that both groups are exposed to similar conditions (equal variance). Data AnalysisThe data were entered into EPI INFO (6.04b version) 12 and was then exported to SPSS (9.0 version)13 for analysis. Quantitative data were analysed using simple proportions, chi-square and t-test. The level of probability was set at 95% confidence interval (p<0.05). All “Don’t know” category in all the tables were excluded from the analysis. Confounding factors such as age and sex were control for by comparing parameters based on same age group and gender for level of significance. ResultsThe response rate was 93%. Fifty three per cent of the sample was male and 47% female. Table 1 show that occupations of the oral health care workers in the public sector in Osun state. There were 30 (71.4%) male and nine (24.3%) female dental surgeons making a total of 39 (95.7%) dental surgeons. Dental therapists formed the smallest group (6%). The majority of the sample (73%) was in the 25-40 year age group and the mean age was 37.3 years. Just over half of the males (52%) in the government dental practice for less than ten years, while 70% of the females were in practice for between 11 and 20 years. There was a statistical significant difference in years of practice among the OHCW in Osun state (t = 25.99, df= 78, p<0.001). The majority of the OHCW in Osun State did not have additional qualification(s). Thirty-four (81%) males and 24 (65%) of females had no added qualifications. Statistically significant gender difference was observed among OHCW aged 25-40 years (p=0.001) with regard to the identification of risk factors and the oral manifestation associated with HIV/AIDS. The contrary was the case for those more than 40years and above (p>0.05). Just over 80% of the female respondents could not identify the common risk factors of HIV/AIDS, compared to 45% of males (Table 2). There were 3 (3.8%) males and 6(7.6%) females with poorest attitude to HIV/AIDS patients, whereas there were 15 (19.0%) males and 2 (2.5%) females with best attitude to HIV/AIDS patients. Table 3 shows the attitude of OHCW to HIV/AIDS patients. Just over a quarter reported that they believed that HIV/AIDS patients are immoral people; nearly 40% of respondents would not like to embrace HIV/AIDS patients, 46 (58.2%) while 66% reported that they would like to treat or assist in management of HIV/ AIDS patients. More than a third of the respondents (65%) felt that an OHCW should continue to work after he/she has been infected with HIV. There was a significant difference between the gender and attitude of OHCW towards HIV/AIDS patients (p< 0.05). AS shown by table 4, age group matching of OHCWs attitude reveals that the level of significance between male and female was more for those in group 25-40yrs than among those in group 41-60 yrs. It appears that male OHCW have better attitude towards the HIV/ AIDS patients than the females. Assuming that the males and females were exposed to similar conditions there was a significant difference between the practice of OHCW based on the gender (p = 0.02). Male OHCW comply more with the principles of infection control than the females. (Mean score males = 18.62, Females =15.43). In this study, it was found that 68 (86.1%) felt the availability of preventive measures was inadequate and 11(13.9%) felt it was adequate Table 5 shows the use and practice of infection control among OHCWs in Osun state. More males (19; 24.1%)compared to five (6.3%) female uses eye wear. Also, 10 (12.7%) male respondents compared to 6 (7.6%) females believe that oversize gloves gives better protection. Discussion There were 42 (53%) males and 37 (47%) females among the respondents and their ages ranged from 25 - 60years with mean age of 37.3years. Over seventy per cent had no additional postgraduate qualifications. Nearly half of the sample was dental surgeons (49.4%). There was a significant gender difference with respect to both the identification of the risk factors and the oral manifestations of HIV/AIDS among the OHCWs whose age range from 25-40 years. This could be that those OHCWs in this age range that form the bulk of the study population are likely to be deficient in their knowledge of HIV/ AIDS that could have assisted them in recognising the oral manifestations and HIV/AIDS risk factors. These young OHCWs might have left school not quite long ago and it would be expected that the OHCWs in this group had a better formal education on HIV/AIDS especially since the disease was discovered in 1981. This could be that the curricula of such schools might have not dealt well enough on the disease. In alternative seminars/workshops/ conferences on HIV/AIDS would have also augmented any possible deficiency in knowledge on HIV/AIDS if they have participated in such. A significant association was found between OHCW gender and their attitude to HIV/AIDS patients. A greater proportion of the male respondents indicating a better attitude towards HIV/AIDS patients than their female counterparts. This concurs with findings in literature that suggested that more males comply with infection controls measures than their female counterpart6 this compliance would have encourage them to have willingness in assisting/treating HIV/AIDS patients. Significantly more males complied with universal cross-infection control principle than the female respondents. This finding was not expected as females usually exhibit greater anxieties regarding treatment and management procedures 6 . It has been previously reported that increased compliance with the cross-infection control practices positively influences the willingness of health care workers to treat HIV/AIDS patients 14 Sixty six per cent of the sample reported that they are willing to treat HIV/AIDS patients and this is slightly higher than other reports 6, 7,9,19. Of concern is the fact that 79% of the females reported that they were unwilling to treat HIV/AIDS patients, while male respond ents were more willing (45%). This is far less than satisfactory against a background of better understanding, clear guidance and unequivocal recommendations regarding the treatment of these patients in clinical practice. A number of factors may be at play here and include issues around lack of confidence in infection control procedures; ill-informed concerns about the risks associated with treatment of high-risk patients; financial considerations relating to cross-infection measures and staff resistance 6 . Attendances of courses have been shown to be a significant factor in the willingness of health care workers to treat high-risk patients. This may be due increased knowledge gained at such courses. The concept of universal precautions (all patients treated as infectious) continues to be a difficult one for oral health care workers to grasp, despite the fact that many would have treated HIV positive patients without being aware of it16. It is therefore imperative that where oral health care workers are not confident about their infection control practices that they seek advice or attend educational programmes to improve their knowledge. Reported infection control practices also showed a lack of compliance. For example only a quarter of the males and 6% of the females reported that they were eye protection. In addition, there appeared to be inadequate surgery cross-infection procedures, infrastructure and equipment. Conclusion and recommendationsThis study showed that there were significant gender difference in attitudes, behaviour and practices of oral health care workers with males faring better than the females. All the OHCWs training institutions in Osun state should make universal infection control and management of patients with HIV/AIDS an important aspect of their curriculum. This will enable the oral health professionals within the state to improve on their practices of infection controls and knowledge on HIV/AIDS. Preventive measures should be made available to the OHCWs in Osun state for their use by the employer. Also the National AIDS Control Programme, Health Control bodies, Health educators and other organizations should make an effort to improve the attitude and practice of OHCW regarding the management of patients with HIV/ AIDS. This could be achieved through organizing workshops, seminars and continuing education programmes on issues pertaining to risks, transmission and infection control. References
Copyright © 2005 - Makerere Medical School, Uganda |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}