 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 5, No. 3, September, 2005, pp. 188-197 Gender power imbalance on women’s capacity to negotiate self-protection against HIV/AIDS in Botswana and South Africa Tabitha T. Langen* *Department of Population Studies, University of Botswana Correspondence author:Tabitha T. Langen* Department of Population Studies, University of Botswana Private Bag UB 00705 Gaborone. Botswana Email: langenit@mopipi.ub.bw Telephone: +267 3552718 Code Number: hs05034 AbstractBackground: Gender power imbalance, which translates into a power imbalance in sexual interactions, is increasingly being recognized as a factor in fueling the spread of HIV/AIDS by increasing the number of unsafe sexual encounters. A variety of related and overlapping behaviour change theories and paradigms have been used to inform the development of HIV/AIDS prevention programmes and interventions. In general, they recognize the complexity of human behaviour and the myriad psychological, sociocultural and structural factors that play a role. More recently, increased attention has been given to the idea of looking beyond individual behaviours to the contextual factors (conditions) that make people vulnerable to HIV infection and influence behaviour. These include, but are not limited to, social norms, gender inequalities and poverty. The influence of gender-based dynamics within the sexual relationships of men and women on reproductive issues is becoming increasingly recognized in the literature. Gender power imbalance translates into a power imbalance in sexual interactions which increases vulnerability to HIV1 . The cultural view which makes it inappropriate for women to suggest condom use to their partners, especially in societies where condoms may be associated with prostitution, promiscuity and disease, women often find it difficult to ask men to use condoms for fear of appearing promiscuous2 , or having asked decide not to persist in asking. The ideas of masculinity associated with risk-taking and sexual conquest, expose men to an increased risk of infection by having multiple partners, thus becoming the vectors for transmission of HIV/AIDS to their partners. These cultural norms and expectations tend to be stumbling blocks to effective HIV prevention. In many societies also the male partner is considerably older than the female, further unbalancing the power differential. Age difference between partners is a form of power imbalance in relationships particularly in patriarchal societies such as those found in Botswana and South Africa where age and seniority are of considerable importance in social life. Here, the older members of a family expect and usually obtain great respect from their juniors. An older brother for example always takes precedence over his younger brother, whose services he can freely command and children are taught to honour and obey their parents and seniors without hesitation or question, and to submit to their authority, under penalty, if need be, of severe chastisement3. This regard for one’s elders is extended beyond the family and kin to relationships between men and women. Many women enter into a relationship with the mind that people senior to themselves in age or rank should always be treated with deference or respect and that failure to show them the prescribed forms of etiquette, or to carry out their reasonable requests, may be regarded as reprehensible and punishable. This means that in relationships where one partner is relatively older than the other, the younger member is bound by tradition to honour, obey and submit to the authority of the older partner. In addition, many men seek younger and younger partners, who are even more physically vulnerable, in the mistaken belief that they can rid themselves of the virus, or that a very young girl will not infect them. These inequalities make it difficult for women to discuss sexual matters with their much older sexually experienced partners, and to successfully negotiate safe sex on equal footing with their partners. Unequal parties are not in a position to negotiate when they have sex, how often and how they can protect themselves from sexually transmitted infections and HIV. Abuse is yet another form of power imbalance in gender relations. Literature4 asserts that underlying all abuse is a power imbalance between the victim and the offender. There are basically three types of abuse that have been identified in the literature, namely physical, emotional and financial/ economic abuse. Physical abuse is the type of abuse which involves physical contact between the victim and the abuser, including threats of violence against the victim. Examples of threats include holding a gun to the head or a knife to the throat of the victim while denouncing the victim’s value5. Physical abuse between intimate partners has been documented throughout history. In 2400 B.C. if a woman was verbally abusive to her husband, he engraved her name on a brick and knocked out her teeth with it6. Emotional abuse is that indirect psychological maltreatment, the implicit nonphysical abuse that victims experience at the hands of their abusers. Included under this type are verbal attacks and humiliation carried out as mechanisms to control and communicate worthlessness of the victim by the abuser. These verbal degradations, harassment, and belittling are some of the strategies used to control or overpower another person in a maladaptive relationship. An analysis of patriarchy as a condition of abuse7 explains why women appear to accept psychological abuse to some extent. There is also financial/economic abuse which refers to restricting of financial resources by the abuser such as in doling out small amounts of money to an economically dependent victim, forcing the victim to ask for more, and in cases where the victim is working or earning cash, is forced to deposit their earnings into the abuser’s bank account or the cash is taken away from the victim against their will. For the abusers, money tends to be an extension of their power8. The sense of powerlessness intensifies as the abused begin to recognise that they cannot prevent or end the damage and pain the abuse has caused them. An abusive relationship is earmarked by a decrease of freedom on the part of an abused person. The abusive partner may limit the social life of the abused, tell them whom they can be friends with, or impose strict financial restraints. In an attempt to control the abused and keep the abuse silent, the abusive partner often makes all of the major decisions. The abused begin to feel as if they have no life of their own, as though they have no voice to speak; and if they did speak, no one would pay any attention. Abusers often try to manipulate the people they are abusing into either thinking the abuse is their fault or to keep the abuse quiet. There are also socio-economic inequities such as great gaps between women and men in education, income, status and other factors which allow individuals to be self-supporting and autonomous. As a result, many poor women who are alone, uneducated and powerless, must depend on a man to support them and their children. There has been a surge in the analysis of gender issues over the past decades within coalition groups, academic and policy circles. Journals such as the Journal of Family Violence; Journal of Social Issues; Law and Human Behaviour; and Crime, Law and Social Change are examples of some of the venues where this discourse is currently taking place among academics. The agendas of the United Nations such as the World Conference on Women in Beijing, China in 1995; the Convention on the Elimination of all Forms of Discrimination Against Women, a convention adopted by the United Nations General Assembly in 1979; the Southern African Development Community Declaration on Gender and Development endorsed by Heads of States at the summit held in Malawi in 1997; extensive research done by Women and Law groups in Southern Africa and other international bodies on changing family forms, reflect a major interest in the elimination of gender power imbalance and any forms of abuse, particularly that which is related to gender. There is also a growing global understanding that the AIDS epidemic is less about epidemiology and more about social factors such as gender inequality which rests on power relations. Organizations dealing with AIDS victims and their families around the world are beginning to recognize that the inequality between men and women fuels the crisis by increasing the numbers of unsafe sexual encounters. However, despite the acknowledgement of the importance of gender inequality in driving and determining the impact of the HIV/AIDS epidemics, and the local, regional and international efforts to create gender awareness, to eliminate all forms of gender inequality and inequity, as well as efforts to criminalize abuse and make it punishable by law, gender power imbalances, including abuse which inhibit individuals’ ability to protect themselves against sexually transmitted infections and HIV, continue to thrive between intimate partners. Unprotected sexual intercourse with an infected partner, owing to the inability to demand condom use from a partner, can directly result in HIV transmission. Therefore, understanding the factors that affect women’s ability to protect themselves against infection may enable the identification of factors adaptable to policy manipulation; and manoeuvring these factors in the desired direction may lead to a reduction in the number of infections including HIV/AIDS. The aim of this study is to examine the influence of gender power imbalance and other factors on women’s ability to suggest condom use to their intimate partners in Kwa Zulu Natal Province of South Africa and Botswana, thereby protecting themselves against sexually transmitted diseases, including HIV/AIDS. Specifically the study aims at investigating the extent to which women are able to negotiate self protection against sexually transmitted infections, finding out from women, in their own words, what happens when they suggest condom use to their partners, as well as male response to the suggested condom use, and to make comparisons between the two selected study areas. MethodsThe study was cross-sectional, with the research conducted during the months of July and December 2003 by the author with the help of twelve research assistants in Kwa Zulu Natal Province of South Africa and Botswana. Preference for these two countries over others in the Southern region of Africa stems from the fact that Botswana has the highest prevalence of HIV infection in the world – 35.4% of pregnant women in Botswana were HIV-positive in 20029; and South Africa has the largest number, 5.0 million, of adults and children infected with HIV/AIDS10. Furthermore, Kwa Zulu Natal Province currently has the highest prevalence of HIV infection in South Africa11. With such high rates of HIV prevalence, cooperation, mutual understanding and respect between intimate partners are necessary in order to achieve successful execution of HIV preventive strategies. The target population was that of sexually active women aged 18-49 years who were, or had been in intimate relationships within the last 12 months before the survey. Two urban districts/areas and four rural districts/ areas were selected for this study. The sampling frame from each of the selected areas consisted of the enumeration areas demarcated for the last censuses of Botswana (2001) and South Africa (1996). These enumeration areas were treated as clusters. The clusters were sampled with probability proportional to size. Two thousand households were randomly selected from within clusters. Before the respondents were interviewed, they were assured of confidentiality and that the information obtained from them would be used only for the study and that they would not be required to supply their names and addresses in the interview. With this assurance and feeling secure in their anonymity, the women opened up and shared their experiences with the interviewers without fear of any reprisals. In this survey the questionnaire was used to collect information on social, economic and demographic characteristics of the woman. Women who were not, or had not been in intimate relationships within the past 12 months were not eligible for further questioning, and having eliminated them resulted in the sample of 2658 eligible women. The schedule also asked women if they had experienced various forms of physical, emotional and financial abuse from their intimate partners within the last twelve months; as well as information on whether the woman had suggested condom use to her partner within the same period. The questionnaire included open-ended questions meant to find out from women in their own words, what happened when they suggested condom use to their partners and if they did not suggest condom use, to find out why they did not. Responses to these ques-tions provided a wealth of information on what happens when women suggest condom use, as well as reasons why women do not suggest condom use to their partners. For those women who had more than one partner within the last 12 months, information was sought about the partner the woman had been with longest. Independent variables are divided into:
The dependent variables are:
Diagnostics In multiple regression analysis independent variables should not be highly correlated with each other. If two variables co-vary it becomes difficult to disentangle their independent effects on Y, the dependent variable. The correlation matrix was used to diagnose co linearity among the independent variables. Explanatory variables are not highly correlated with each other. Each independent variable was also regressed on all the other independent variables and the R2 examined. The largest coefficient of multiple determination lies a good distance away from 1.0. Tolerance [1-R2] and Variance Inflation Factors [1/(1-R2)] suggest that strong multi-co linearity is absent. Two independent variables are said to interact in determining a dependent variable when the effect of one depends upon the value of the other. No significant interactions were detected. Definition of terms used
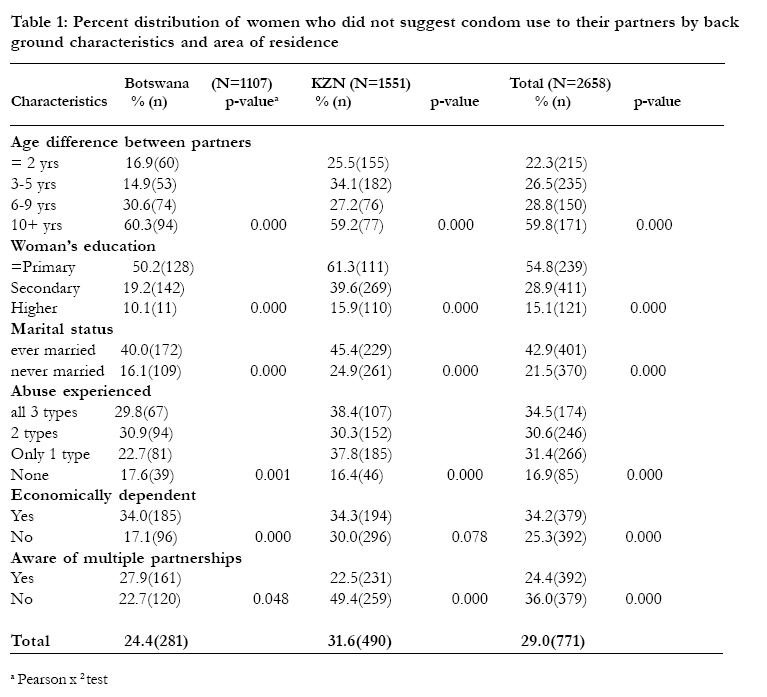
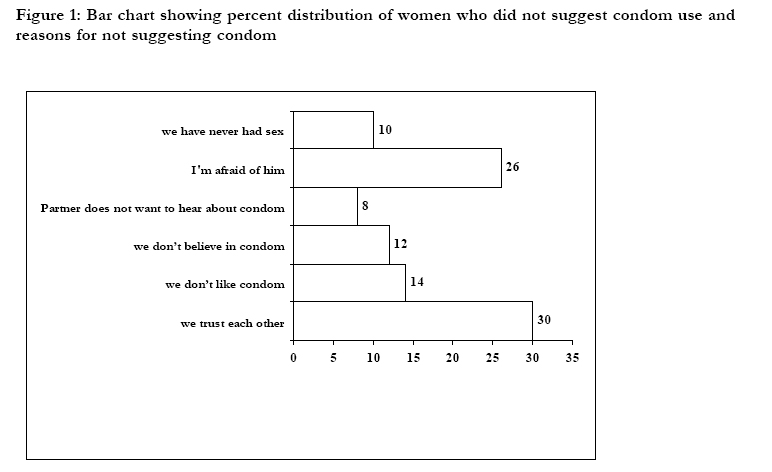
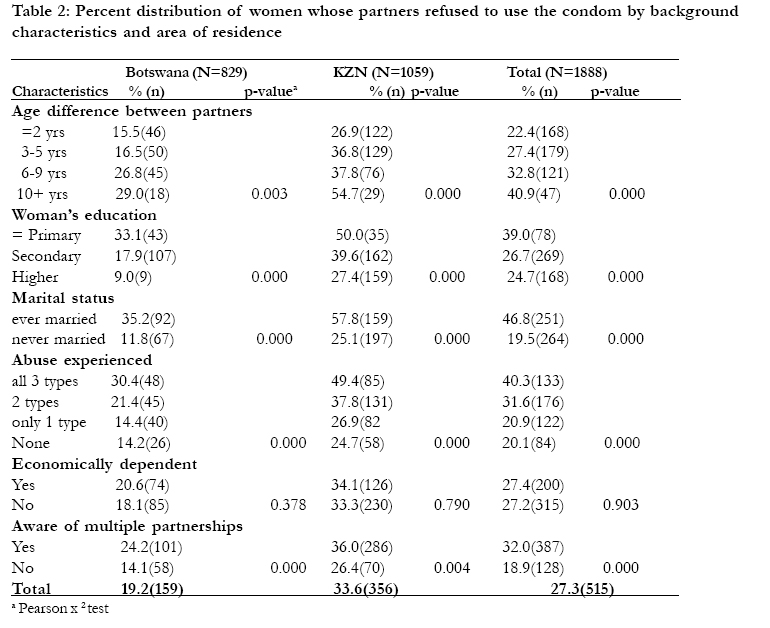
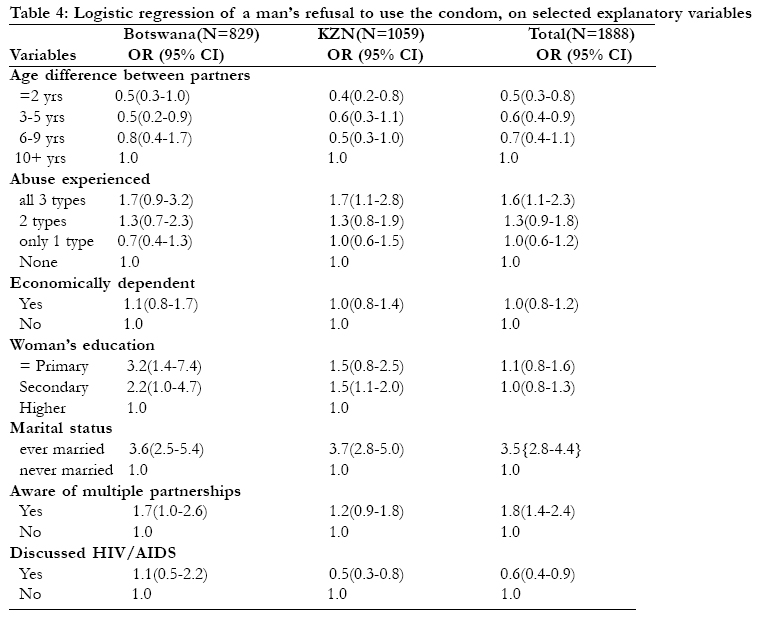
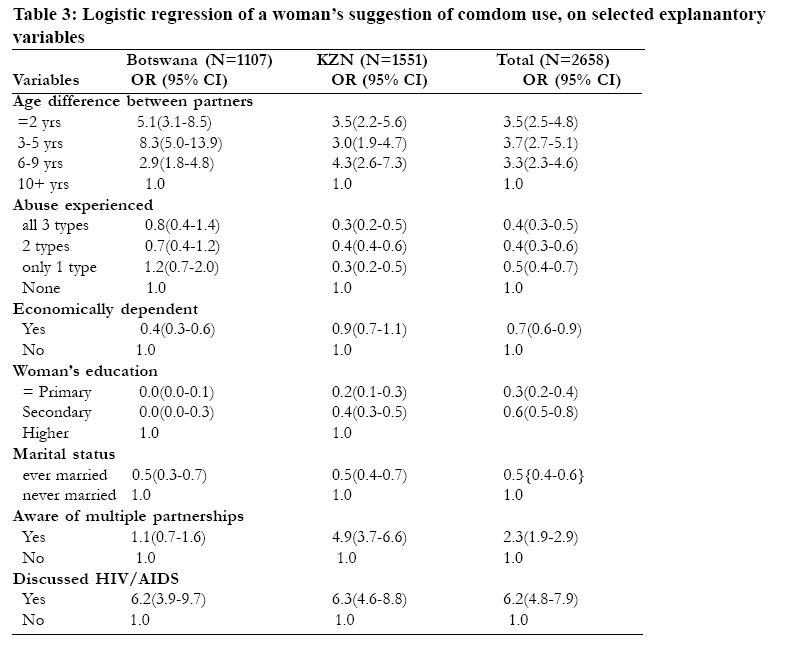
Descriptive analysis was used to summarize the data using proportions and percentages. The Pearson x2 test was used to determine whether differences in women’s inability to suggest condom use (or man’s refusal to use the condom) by categories of background characteristics were significantly different. Logistic regression models were used to determine the predictors of women’s inability to suggest condom use (and men’s refusal to use the condom) in Kwa Zulu Natal and Botswana. All background characteristics analyzed were coded as indicator variables and included in multivariate logistic models. The results were presented by the odds ratios, the 95% confidence intervals and the p-values. The SPSS data analysis software was used. Although the survey aims at investigating the extent to which gender power imbalance affects women’s capacity to protect themselves against sexually transmitted infections, the survey is only a sample concentrating only in Kwa Zulu Natal Province of South Africa and selected districts in Botswana and may not necessarily be representative of each of the countries selected. With more funding available it would have been ideal to conduct a representative national survey in each country. Nevertheless the results of this study could be a microcosm of the proceedings in the Southern African region and serving as a pilot study could raise important issues relating to gender power imbalance and the proximal HIV preventive practices. Results Descriptive statistics The mean age of women in the sample was 27.3 years whereas that of their partners was 31.9 years. About 65% of the respondents had never been married before. In both areas there were about 10% more males reported as having attained the education level above secondary school than females. The speakers of the local language were 69% more than those who speak Afrikaans or English at home and this reflects the reality in the two countries as people who speak English/Afrikaans at home constitute the minority in these areas. About 11% of the sample population was 10 years younger than their male partners and 30% were at least 6 years younger. The age difference between partners was wider in Botswana than in Kwa Zulu Natal Province. In both areas the percentage of employed male partners was almost twice that of employed women. Where a woman reported that she did not suggest condom use because they were already using it or the partner had already suggested its use, that was recorded as having suggested condom use. Table 1 indicates that out of the total sample of 2658 women interviewed, only 71.0% suggested condom use to their partners during the twelve months before the survey. The remaining 29.0% women, despite living in an area where the incidence of HIV infection is rated the highest in the world, did not suggest condom use to their intimate partner within the last twelve months before the survey. In the overall sample the highest proportion of women who did not suggest condom use to their partners is among women whose partners are 10 years or more older than them followed by women educated only up to primary school level. Married women also constitute a large proportion of women who did not suggest condom use to their partners. In Kwa Zulu Natal Province it is primary educated women who exhibit the highest percentage of those who did not suggest condom use to their partners followed by those who are 10 or more years younger than their partners. The inability to suggest condom use to intimate partner seems to have an inverse relationship with education in that it tends to decline with an increase in education. Reasons reported by respondents for not suggesting condom use to their intimate partners are shown in Figure 1. Responses such as: “I’m scared to talk about that subject with my partner because he’ll say I’m having an affair; he might think that I don’t trust him; we trust each other; he would kill me if I were to talk to him about condoms; and our religion/culture does not allow us to use the condom” constituted the bulk of answers received from women who did not suggest condom use to their partners. These results seem to suggest that women who do not freely communicate suggestion of condom use to their partners may be afraid that increased partner communication bout sexuality may disrupt power balance in intimate relationships, leading to marital discord, suspicions of infidelity, and even intimate partner violence. Table 2 indicates that 27.3% men refused to use the condom despite being asked by their women partners. The proportion of men who refuse to use the condom is higher in Kwa Zulu Natal than it is in Botswana, and it is mostly married women in both countries whose partners refuse to use the condom. Among women who suggested condom use to their partners, 19 reported that they experienced violence from their male partners upon suggesting condom use to them. One 27 year old woman from Kwa Zulu Natal Province of South Africa with a 31 year old partner said: “He really got upset with me and we got into a huge argument and he ended up silencing me with a few beatings.” Another one from Botswana said “He gave me a good hiding and told me to forget the condom”. High incidences of rebuttal from male partners, upon suggesting condom use to them, were also reported by severely abused women and women educated only up to primary school level. Logistic regression resultsThe bivariate analysis results in Tables 1 and 2 above have shown that there are differences in condom use suggestion by women and in condom use refusals by men crossclassified by selected background characteristics. But it is not known to what extent the individual variables jointly affect women’s ability to suggest condom use to their partners. Thus it is necessary to use the logistic regression technique to provide a clear perspective on the net effects of the relationship between the dependent and independent variables. The analysis shows that gender power imbalance variables significantly influence a woman’s ability to suggest condom use to her partner. The odds in favour of condom use suggestion for women in relationships where the age difference is less than 5 years are almost 4 times as large as those for women with partners 10 or more years older than they are. This relationship is statistically significant in both Botswana and Kwa Zulu Natal Province, all things being equal. The analysis shows that while abuse significantly influences women’s ability to suggest condom use to their partners in KwaZulu Natal, in Botswana it is of no significance. Also while economic dependency is an important predictor of women’s capacity to negotiate self-protection in Botswana, in South Africa it is not. Nonetheless the overall model indicates that the odds for suggesting condom use to an intimate partner among women who experienced all 3 types of abuse are 61.8% lower than those for women who experienced no abuse at all. The overall model depicts gender power imbalance variables as statistically significant predictors of women’s inability to suggest condom use to their partners. The above scenario assumes that abuse influences women’s ability to successfully negotiate condom use. However, some studies have suggested a reversal of the above relationship in the form of women being at risk of emotional, sexual and physical abuse as a consequence of negotiating condom use 12. To find out if negotiating condom use puts women at risk of abuse in this study, abuse was turned into a dependent variable and was regressed on suggestion of condom use and the results showed that negotiation of condom use is not a statistically significant predictor of abuse in this study. To find out to what extent women’s ability to protect themselves against HIV and sexually transmitted infections is influenced by the socio-demographic and sexual risks behaviour variables as a group; and to examine whether the addition of these variables makes a significant contribution to the prediction of women’s ability to suggest condom use, the null hypothesis that the coefficients on all 4 added variables are equal to zero, was tested. The log likelihood from the full model containing all variables (2546.998) was compared with that of a simpler model containing only the gender power imbalance variables (3011.284). ??H = - 2(loge & K-H – log e & K ) which resulted in 928.572. With 5 degrees of freedom (because there are five more parameter estimates in the full model than in the model containing only the gender power imbalance variables) the results were highly significant (p=0.000) and so the hypothesis that all four variables are zero was rejected. This suggests that the additional variables depicting the socio-demographic and sexual risks aspects are very important. Therefore it was concluded that the woman’s education, her marital status, being aware of the man’s multiple partnerships and discussion of HIV significantly influenced women’s ability to suggest condom use. Ever married women included women currently married, women who were not married but were living with their partners as though they were husbands and wives, as well as those who were separated, divorced and widowed. Some of the women in this group reported that they did not suggest condom use to their partners because they wanted to get pregnant and to have children as expected of a married woman. Some women who had been married for a long time expressed an element of great trust in their spouses, hence their nonsuggestion of condom use to their partners. Marriage to them seems to have provided them with a sense of security which appeared lacking among women who had never been married before. The odds for suggesting condom use among ever married women are about 50% lower than those for women who have never married before. It seems that men find it much easier to refuse to use the condom when their female partner is 10 or more years younger than them as shown in Table 4. Married women, and women who are aware that their partners had relationships with other women besides themselves, are more likely to have their suggestion of condom use fall on the deaf ears of their male partners. However, when partners talk, the probability of a man refusing to use the condom is significantly reduced. (Table 3) Discussion The purpose of this study was to investigate the influence of gender power imbalance and other factors on women’s capacity to suggest condomuse to their intimate partners, thus protecting themselves from sexually transmitted infections, as well as the probability of the male partner refusing to use the condom. The study showed that it is women whose partners are 10 or more years older than them, women who are abused, and those who are economically dependent on their partners who are less likely to suggest condom use to their partners. The study suggests that powerlessness and dependency diminish the abused woman’s ability to make healthy decisions, including negotiation for safer sex in order to protect herself against sexually transmitted infections. Women who are educated only up to primary school level, married and do not have an open communication with their partners on matters related to sex and HIV are also less likely to suggest condom use to their partners. The study also showed that men are more likely to refuse to use the condom when the age difference between them and their female partners is wide (10+ years difference), if they are in a married relationship, and where there is no communication about HIV/AIDS between them and their partners. What is more disturbing is the finding that it is men who have multiple partners who are significantly more likely to refuse to use the condom. The need to focus on women’s education, promoting the self confidence they need to protect themselves, irrespective of age difference between partners and cultural expectations, as well as the need to encourage men to replace risk-taking with taking responsibility was emphasized by the results of this study. Across all levels of society, there is a need to see a social paradigm shift that transforms relationships between women and men, from the one of dominance of one by the other, as is the case in patriarchal societies, to respect and consideration for one another as equals. Policies that promote healthy behaviour and HIV prevention must incorporate some fundamental changes. Given that male behaviour is one of the main determinants of HIV infection in women, the participation of men in prevention activities is clearly essential. Ensuring that sexual health is understood to be the business of men as well as women is also critical. Educational messages that simply tell people to “use a condom” do not address the power imbalance between men and women. HIV/AIDS programmes should simultaneously focus on men and acknowledge women’s need for support and resources. Effective HIV/AIDS programmes need to encourage men and women to talk about sexuality and safety, while also promoting the fundamental link to the safety and well-being of their partners and children Finally, high profile men, such as heads of states, politicians, sports figures, and other celebrities, must accept and advocate for men’s responsibility in promoting and safeguarding sexual health. Also informing women of their rights increases their bargaining power in sexual and other matters. AcknowledgementsThis study was funded by the University of Botswana research grant allocation no: R149 in 2003. The author would like to thank all the research assistants who helped with data collection in South Africa and Botswana, but most of all sincere gratitude goes to all the women who shared these intimate details of their lives with us. The views expressed in this report are those of the author and do not reflect in any way the views of the organization which funded the project. References
Copyright © 2005 - Makerere Medical School, Uganda |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}