 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
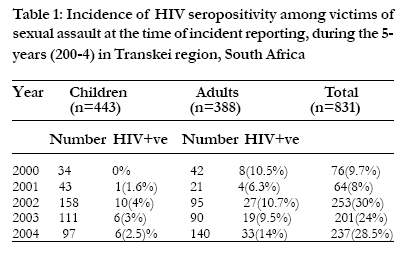
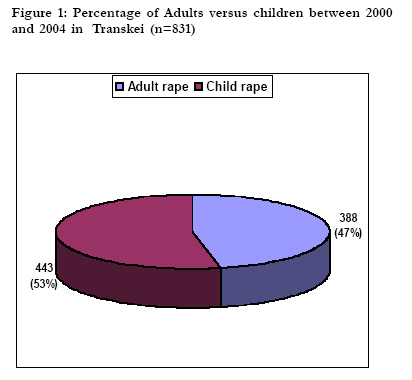
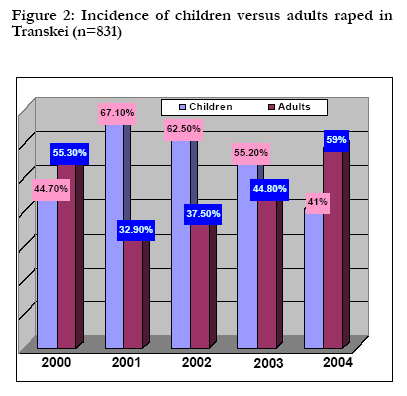
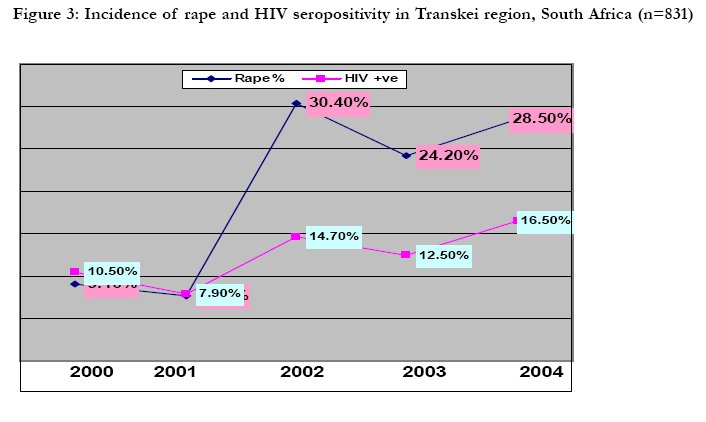
African Health Sciences, Vol. 5, No. 3, September, 2005, pp. 207-212 Incidence of HIV infection at the time of incident reporting,in victims of sexual assault, between 2000 and 2004, in Transkei, Eastern Cape, South Africa BL Meel Department of Forensic Medicine, University of Transkei, Correspondence author: BL Meel Department of Forensic Medicine, University of Transkei, Umtata 5100. E-mail: meel@getafix.utr.ac.za Code Number: hs05036 Abstract Background: HIV/AIDS epidemic and sexual assault have emerged as the most serious public health problems in South Africa.
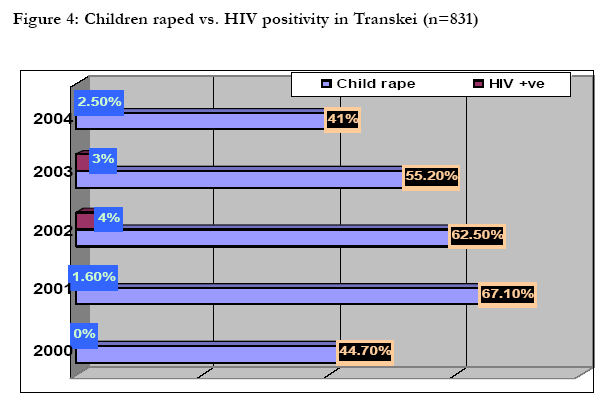
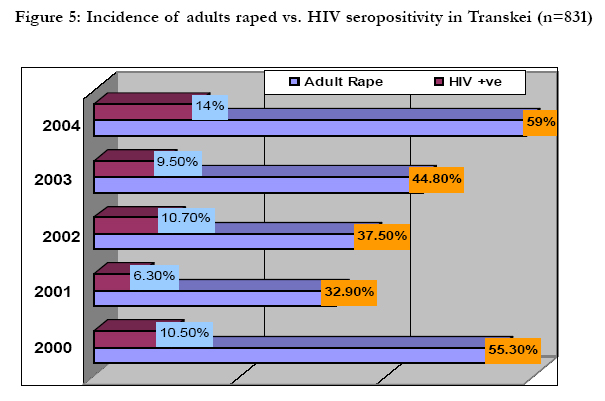
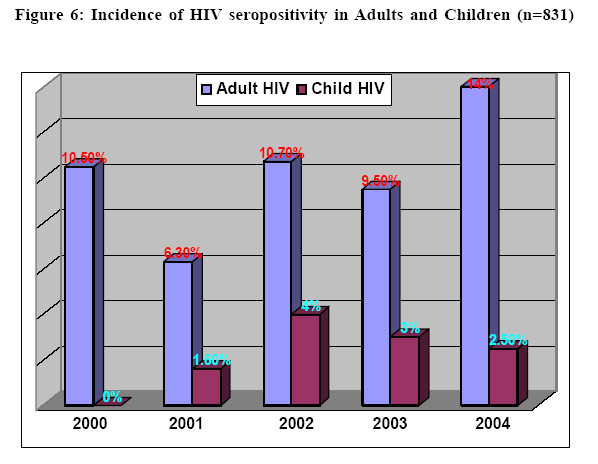
The country has about 5-million HIV infected individuals. About a million women are raped every year. Sexual violence is ubiquitous; it occurs in every culture, in all levels of society and in every country of the world. Data from country and local studies indicate that, in some parts of the world at least, one woman in every five has suffered an attempted or completed rape.1 South Africa has been facing the dual epidemics of HIV/AIDS and sexual violence, and these will continue to claim the lives of many South Africans.2 The combination of high prevalence of sexual assault and HIV infection in South Africa places women and girls at high risk of exposure to HIV.3 In this country, one of the driving and most violent forces behind the AIDS epidemic is rape. By one estimate, there are more than one and a half million rapes in the country each year.4 The incidence of rape in South Africa is one of the highest in the world. One in four South African women will experience rape; 380,000 cases of rape occur annually. Rape is fueling the AIDS epidemic.5 South Africa is host to the highest number (5.3 million) of HIV-infected people in the world.6 The impact of possible infection with human immunodeficiency virus (HIV) in survivors of sexual assault has not received its due attention even after two decades of the epidemic. South Africa has one of the highest HIV/AIDS infection rates in Africa. Transkei, a former black homeland, now a part of the Eastern Cape Province, has a large number of HIV/AIDS sufferers. The myth of the ‘HIV/AIDS virgin cure’ is prevalent in the community.7, 8 An investigation into the prevalence and characteristics of child sexual abuse in the Northern Province of South Africa has shown a prevalence of 54.2%. 9 The largest group of perpetrators (33%) were school teachers.8 In 2000, 52,550 cases of rape and attempted rape of women were reported to the South African police, 21,438 (41%) of which were of minors under the age of 18 years and of these 7898 (15%) were under the age of 12 years (mostly between 7 and 11 years). 10 The HIV prevalence in the Eastern Cape is 23.7%. This is mainly in those that have consensual heterosexual intercourse. Transmission through sexual contact accounts for 75-85% of the infections with HIV.11 A recent study by the author showed that 90% of rape victims were HIV negative at the time of the incident. 12 The purpose of this study is to determine the incidence of HIV among the victims of rape at the time of the incident, and to highlight the problem of rape in the region. Patients and Method This is a retrospective study done in Sinawe Centreover 4-years from 2000 to 2004. This unit is a component of the Nelson Mandela Academic Health Complex. It caters to a population of about 300,000 in the districts of Umtata, Mquanduli, Ngqeleni, Libode, Tsolo and Engcobo. The female population is assumed to be about half. The Sinawe Centre was established in 1999, and began to function in 2000. It is a ‘One Stop Centre’ providing multi disciplinary management of victims of rape. It is open from Monday to Friday from 08h00 to 16h00. On weekends and after hours, the victims were examined in the Gynaecology Outpatient Department and followed up in Sinawe Centre. It is a policy of the centre to provide HIV testing after counselling to all the victims. Blood for HIV screening is taken with the consent of the victims. Post-exposure Prophylaxis (PEP) was started at the beginning of 2003, and is offered to all the victims except those who came later than 72 hours after the incident. Subsequent follow up was advised after 1 week, 4 weeks, 12 weeks and 6 months. Initially, zidovudine (AZT) and lamivudine (3TC) were given for a week. HIV test results were usually received within a week. Those who were seronegative continued with PEP. All the victims were able to contact the doctor by phone anytime during the treatment. Following the 1998 South Africa Demographic & Health Survey and the WHO, we defined childhood sexual assault (CSA) as those occurring before 15 years of age (Department of Health, South Africa1999; WHO Multi-Country Study Core Team 2000). ResultsThere were 831 cases of sexual assaults (rape) reported in last 5-years (2000-2004). Of them, 443 (53.3%) were children under 15-years of age (Table 1 & Figure 1). There has been increase in adult rapes from 55.3% in 2000 to 59% in 2004. The adult rapes have significantly come down to 21 in 2001, but at the same time child rapes were doubled to 43. However, incidence of rape of children has been tapering off from 67.1 in 2001 to 41% in 2004 (Figure 2). There has been increasing in rapes from 76(9.7%) in 2000 to 237(28.5%) in 2004, and HIV infection from 8(10.5%) to 39(16.2%) in the same period (2000-2004). The peak year of rapes 253 (30%) was 2002, and HIV infection 39 (16.5%) was 2004 (Figure 3). A total of 114 (13.7%) tested positive for HIV, and 23 (2.7%) were children less than 15 years (Table 1). The HIV infection has increased among children from 0% in 2000 to 2.5% in 2004, with peak (4%) in 2002 (Figure 4). The incidence of adult rapes, and HIV infection were also increased in the last five- years (2000-2004) (Figure 5). HIV infection among children is climbing down, but in adult it is climbing up in this study group (Figure 6). There is significant difference in HIV seropositivity among children compared to adults, p<0.05, and Paired t=3.45 with 3df. Discussion There are no reliable data available regarding the number of rapes, and HIV infection in those victims in Transkei region. HIV/AIDS carries with it a stigma and discrimination, the same way rape is associated with social isolation. Therefore it is difficult to estimate the number of rape victims, and the consequences such as pregnancy, HIV seroconversion and contraction of other sexual transmitted infection (STIs). Women need reliable HIV prevention methods that they have the power to control and use without their partner’s knowledge. Unfortunately, such a method is not available. A high proportion of women is illiterate in this area, and survives solely on the income of their male partners. A quarter of women have been sexually abused by current or former partners. The gender based social and economic inequalities often made it impossible for women to negotiate for safer sex.13 There were 831 cases of sexual assaults (rape) reported in last 5-years (2000-2004). Of them, 443 (53.3%) were children under 15-years of age (Table 1 & Figure 1). Among 13-17-year-old females in the rural Transkei area of South Africa, 28% report first sex as forced. 14 In many of the HIV heavily affected countries; young people represent the most rapidly growing component of new HIV/ AIDS infections, with girls outnumbering boys. The reason for this vulnerability include factors relating to poverty, lack of information, lack of economic and social empowerment, and lack of protective methods.15 There has been an increase in adult rapes from 55.3% in 2000 to 59% in 2004 (Figure 2). Although sexual assault of children is down from 44.7% (2000) to 41% (2004), the overall number has increased from 34 (2000) to 97 (2004). The total number of rapes has increased by more than three times among children and adults during from 2000 to 2004 (Table 1). However, the cause of this increase is difficult to establish. Children are generally easy victims of rape especially by their relatives, and sometimes by their father or guardian. It is difficult to reveal the truth of rape, because the bread winner is often the perpetrator of rape. Low social and economic position puts young women at a disadvantage in sexual negotiations because they are more dependent on their partners for survivals.16 There were 76 (9.1%) rapes reported in 2000, which increased to 237 (28.5%) in 2004. In the same period the HIV infection among the victims of rape also increased from 10.5% (2000) to 16.5% (2004) (Figure 3). The prevalence rate of HIV infection in this study correlates well with two recent national population based studies of HIV sero-status. The first, the Mandela Foundation- Human Sciences Research Council (HSRC) study in 2002, focused on South Africans of all ages. HIV prevalence rate of those between 15-24 years were 12% for females.17 The second study, by Pettifor et al (2004), showed the prevalence rate in the same age group women as 15.5%.18 . This more than three-fold increase in the rapes, and 1.5 times increase in the HIV infection in this area, are the major causes of concern (Figure 3). Rapes are fuelling the HIV infection and viceversa. There are many factors influencing the risk of man becoming sexually violent. Some of these factors are related to the attitude, beliefs and conduct of the individuals involved, while others are deeply rooted in social environment.12 The widespread rape and forced sexual abuse of children is a serious social and health issue. In this study majority (53%) of victims were children. One of the motives behind this antisocial and unhealthy epidemic is the strong belief in a myth of achieving a cure for a person’s HIV infection through sexual intercourse with a virgin.7 On the other hand in the absence of a cure for HIV, the infected person is constantly looking for alternatives towards a cure, and therefore they are forced to follow the prevalent myths in the community. Use of substances such as alcohol could lead to sexual compulsivity and likely to report sexual risk practices.19 There has been an increasing incidence of HIV seropositivity among women in this study. In 2000, 10.5% of women were found to be HIV positive, and it has increased to 14% in 2004 (Figure 5). Eight out of every 10 women who are HIV positive in the world are in Sub-Saharan Africa.20 A 1998 survey by the Centers for Disease Control (CDC) revealed that only 1.1% of women who were victims of sexual assault agreed for HIV testing and 0.5% of them were sero-positive.21 It is difficult to estimate the HIV sero-conversion secondary to rape. Two cases (one child and other adult) were confirmed in this study. One of the victims who sero-converted was 13 years old. PEP defaulting is not uncommon among rape victims. Majority (84.5%) did not report for the second test, and only 3.3% reported for third test.22 Most victims had not been on PEP as they have reported later than 72 hours, and never returned for follow up. Therefore it is difficult to ascertain the true number of sero-conversions, but the risk of HIV transmission from a sexual assault is estimated to be greater than 0.2%.23 HIV infection is certainly increasing among adults and children in this region (Figure 6). A recent study (2005) by the author showed that HIV, Hepatitis B and syphilis are mostly prevalent in the 11 to 20 year age group.24 Transmission through sexual contact accounts for 75 to 85 percent of HIV infection.25 The risk of contracting HIV infection from one act of unprotected consensual vaginal sex with an HIV positive partner is approximately 0.1%.26 Rape may increase the risk of HIV transmission compared with consensual sex because trauma is more likely.27 Since the beginning of 2003, PEP is being provided to all victims of sexual assault in Eastern Cape Province. This is a justifiable step to curb the HIV epidemic, but the follow up is poor. The probability of infection through sexual contact, although it varies greatly, appears to be lower than that of infection through other routes of exposure. The variability observed among and within routes of HIV exposure depends partly on the viral dose and also on whether the virus is transmitted directly into blood or onto mucus membrane. Victims should consider getting a baseline HIV test immediately after the assault. The mandatory HIV testing of the alleged perpetrators could avoid the 28-day PEP. This will also be helpful for the perpetrators, as they could avail the opportunity of PEP in case the victim is found to be HIV positive. Being diagnosed with a life-threatening illness can be very scary for an already traumatised raped woman. Every sixth rape such victim was found to be HIV positive in this study. ConclusionThere is an increasing incidence of HIV infection among victims of sexual assaults at the time of reporting. Sexual assaults and HIV infection are inseparable and have a close relationship. It is important to emphasize that to control the HIV epidemic; there is a need to control of the rising incidence of rape in this region. An intensive support system should be in place to deal with the breaking news of HIV infection to victims of rape. AcknowledgementThe author wishes to thank Dr.George Rupesinghe, Senior Specialist, Family Medicine, Mthatha General Hospital for assistance given during the preparation of this manuscript. References
Copyright © 2005 - Makerere Medical School, Uganda |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}