 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 5, No. 3, September, 2005, pp. 213-218 Health system constraints to optimal coverage of the prevention of mother-to-child HIV transmission programme in South Africa: lessons from the implementation of the national pilot programme Tanya M Doherty*1, David McCoy1, 2, Steven Donohue3 1 Senior Researcher, Health Systems Trust, Code Number: hs05037 Abstract Background: It is three years since the government of South Africa began implementing a PMTCT programme. Over this period
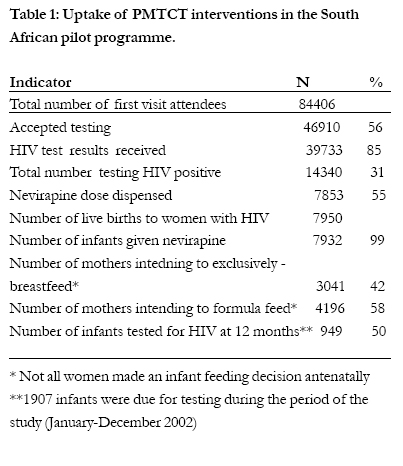
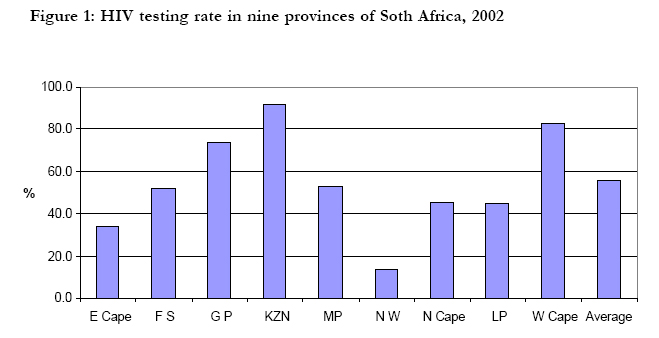
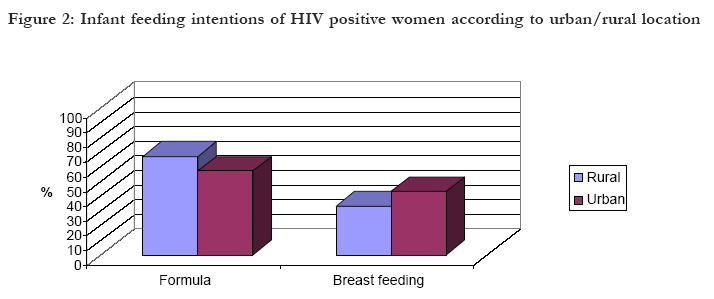
of time attempts have been made to scale up this programme across all provinces under routine health service conditions. South Africa is one of the countries worst affected by the HIV/AIDS epidemic 1 . Annual sentinel site HIV prevalence studies in antenatal clients have been ongoing since 1990 and reveal the explosive growth of the HIV epidemic from a prevalence of less than 1% among pregnant women in 1990 to 26% in 2002 2 . In 5 of the country’s 9 provinces at least 25% of pregnant women are now HIV positive. Based on calculations derived from these prevalence figures, it was estimated that in 2002, 69 000 infants were infected with HIV at birth and a further 20 000 would become infected through breastfeeding 3 . At the end of 2000, a decision was made by the National Department of Health of South Africa to implement a pilot programme for the prevention of mother to child HIV transmission (PMTCT). A total of 18 pilot sites, 2 in each of the 9 provinces, were purposively selected to include an equal representation of urban and rural sites, as well as a mix of primary and secondary level facilities. These were to serve as research and learning sites to assess the feasibility of, and requirements for implementing PMTCT services more widely. The package of care for the pilot programme included offering all antenatal clients voluntary counselling and rapid HIV testing, infant feeding counselling, single dose nevirapine to those women identified as HIV infected, and their infants, and free formula milk for a period of 6 months for women choosing not to breastfeed. The programme also stipulated that all infants should be followed up and tested for HIV, with a rapid antibody test, at 12 months. A research framework was developed to allow for an independent national evaluation of the pilot programme. This paper reports on the findings of this evaluation and identifies health systems challenges to effective implementation and optimal coverage of this programme. MethodsThe overall aim of this evaluation was to assess the performance and uptake of the components of the PMTCT programme in the eighteen pilot sites. A pilot site consists of a tertiary or district hospital and its associated community health centres and clinics. The 18 sites involved in this study consisted of; 5 tertiary hospitals, 15 district hospitals, 8 community health centers and 29 clinics. The evaluation utilised a cross-sectional design that incorporated quantitative and qualitative research methods. Data was collected monthly between January and December 2002 at district and provincial levels by HISP (Health Information System Programme) staff who were employed as consultants to support the PMTCT information system. Programme data was entered into and analysed using the District Health Information System (DHIS) Software. A visit to one site in each of the provinces was made by the researchers in order to observe programme functioning and to conduct semi-structured interviews with health workers implementing the programme. The use of routine data for this evaluation posed problems as there were some difficulties with data quality. Data was collected from registers designed by the National HIV Directorate and in some cases provincial HIV directorates. Registers were completed by health workers at the sites and data was collated by district and provincial information officers. The researchers had little control over the data collection tools, data entry or data flow. Every attempt has been made to validate routine provincial data collected. This was done through review of registers during site visits and attendance at national steering committee meetings where provincial data was presented. ResultsRoutine programme data from the pilot sites is presented in Table 1. Between January and December 2002, 46910 (56%) of the 84406 first antenatal clients agreed to an HIV test. Uptake of HIV testing differed greatly across provinces ranging from 14 to 92% (Figure 1). In all provinces, except KwaZulu-Natal, counselling and testing was designed as an ‘opt in’ model whereby individual counseling and testing was offered to all women and undertaken after individual consent. In KwaZulu-Natal, which achieved an HIV test acceptance rate of nearly double the national average, counselling was considered a routine part of antenatal care and all women received individual counselling and were then offered an HIV test which they could “opt out” of if so desired. This approach is likely to have contributed to the extremely high rate of testing uptake in this province. Another factor that was found to contribute to testing uptake rates was the availability of lay counselors. The provinces with the smallest drop off between first antenatal visits and women accepting HIV testing; namely Gauteng, KwaZulu-Natal and the Western Cape, all prioritised the utilization of lay counsellors, either by directly employing them or by contracting NGOs to employ them. Provinces with low HIV testing uptake such as the North West (14%) and the Eastern Cape (34%) are still struggling to employ lay counsellors and many of the pilot facilities still rely on nurse counselors with a heavy workload. The procurement and supply of test kits also impacted on testing uptake rates. Interruptions in the supply of testing kits to many facilities particularly in the Free State, Eastern Cape and Mpumalanga were reported during the study period. These interruptions resulted in missed opportunities for HIV testing. At this early stage of the programme the procurement of test kits was done through national tendering processes and provinces had little control over the ordering of supplies Overall 39733 (85%) of women who tested received their test results and 14340 (30%) of the women who tested had HIV positive test results, of whom 7853 (55%) were dispensed nevirapine. The rate of uptake of nevirapine did not differ dramatically across sites and was generally sub-optimal. The evaluation found several reasons for the low recorded nevirapine coverage. Most importantly under-estimation of the coverage could occur if a woman chose not to disclose her HIV status to labour ward staff, yet self-administered her nevirapine dose. This dose, although administered would not be recorded in the routine data. Interviews with health workers at the sites revealed that some HIV positive women are reluctant to disclose their HIV status in delivery rooms that lack privacy, or to staff that have not been involved in their antenatal counselling and care. The various systems of unique patient identifiers, usually in the form of stickers, that have been developed for this programme to assist health workers to identify HIV positive women have often been found to be stigmatizing and are removed from maternity cards. During the evaluation period, 7950 infants were born to women identified as being HIV positive. Although it is not possible to determine precisely the expected number of births to women with HIV during this period, due to the variable time lag between testing and delivery, this is a lower than expected number of HIV positive deliveries and confirms the fear that many HIV positive women are not being identified in labour and that missed opportunities for nevirapine prophylaxis are occurring. However, 7932 (99%) of babies born to identifiable HIV positive women received nevirapine syrup. Infant feeding counselling takes place during antenatal care and involves offering HIV positive women the option of exclusive breastfeeding with early weaning at 4-6 months or free formula milk for a period of six month. At discharge, 58% (4196/7237) of HIV positive women expressed an intention to practice exclusive formula feeding, and 42% (3041/7237) of HIV positive women intended to practice exclusive breastfeeding. Figure 2 shows infant feeding intentions according to rural/ urban location of the sites. It is clear that the predominant choice of infant feeding across both locations is formula milk. Of concern is the higher rate of intention to formula feed in rural sites (67%) compared with urban sites (57%). Very little information is known about the actual infant feeding practices of HIV positive women due to the poor follow up rates under these routine programme conditions. Provincial variations in infant feeding intentions were noted during site visits. For example, in KwaZulu-Natal and the Free State more than 60% of HIV positive women intend to exclusively breastfeed; whilst in the Western Cape and Gauteng, more than 80% of HIV positive women intend to exclusively formula feed. These large differences between provinces, with similar urban-rural locations of sites, was found to be due to provincial or facility policies on infant feeding as well as differences in the prioritization of infant feeding counselling training. In KwaZulu-Natal and the Free State enormous efforts have been underway to ensure that all staff involved in PMTCT have undergone the WHO/ UNICEF HIV and infant feeding counselling training course. Several operational problems with the distribution of free formula milk were noted during site visits. In almost all of the sites there were reports of formula supplies running out and difficulties with the procurement of supplies due to national tenders with the manufacturing company. Furthermore, health workers reported that many mothers returned to the facilities to fetch more supplies before their scheduled return dates. There were suspicions amongst health workers that women were selling the tins and in some sites this led to them decreasing the number of tins given to women at each visit as a disincentive for them to sell the tins. This resulted in women having to collect tins fortnightly instead of monthly. Interviews with health workers revealed great concern and confusion over what to advise women to feed their infants when the free formula supply ends at six months. The solution adopted in many areas was to transfer infants to the PEM (protein-energy malnutrition) scheme in order for them to continue to receive free milk. This will have serious financial implications for the PEM scheme. A total of 1907 infants who were born during the first year of the programme were due for 12 month HIV testing between January and December 2002. Of these, 949 (50%) were tested. The national policy to test infants at 12 months was made due to fears that waiting until 18 months for the first test would result in a large loss to follow up. Infants that test HIV positive at 12 months or are still being breastfed should be brought back to the clinic for a repeat test at 18 months. The rapid antibody test was chosen due to the high cost of PCR tests and limited laboratory infrastructure at the time the programme was introduced. Infant follow up varied across provinces from 10% to 78%. Of the infants who were tested, 170 (18%) tested HIV positive. Given the small number of infants tested and the testing method utilized (rapid antibody test at 12 months in a predominantly breastfeeding population) this figure cannot be considered an accurate reflection of the vertical transmission rate. Although the impact of the programme on preventing infant HIV infection cannot be determined from this routine programme data, a prospective cohort study commissioned by the Department of Health has recently been completed and will provide information on the operational effectiveness of the programme. DiscussionThis evaluation yields useful insights for the planning and implementation of a scaled up PMTCT programme in South Africa and other sub-Saharan African countries. The low coverage of key components of this programme found in South Africa is consistent with other studies showing an overall low uptake of PMTCT services in Africa 4 . Compared to a similar programme in Botswana, South Africa achieved a higher rate of HIV test acceptance amongst antenatal clients 5. However, there is room for improvement. Obstacles to testing uptake included inadequate numbers of lay counselors, the opt-in strategy for counseling which separated PMTCT from routine antenatal care and disruptions in the supply of rapid test kits to sites. Variations in the uptake of testing between provinces emphasize the importance of a well functioning health system, particularly strong management capacity, as a basis for the introduction of this new programme. For example, provinces with active provincial and district managers were able to develop structures to employ lay counselors to support the programme, to integrate HIV testing into routine antenatal care and to ensure reliable supplies of test kits. Experience in other African settings has shown that the active involvement of health managers and a district approach leads to more successful implementation of PMTCT6. It is a concern that only 55% of eligible women were recorded as being dispensed nevirapine. Other studies have found similarly low coverage 7, 8 . The use of routine programme data to determine nevirapine coverage is limited due to the time lag between providing the drug (usually at 28 weeks) and labour. As the programme is scaled up, a different approach to collecting this data is needed. Furthermore, attention needs to be paid to creating an environment within the labour ward setting where women feel comfortable disclosing their HIV status to health workers. In this evaluation, non-disclosure of status was found to limit access to nevirapine prophylaxis. A recently published qualitative study from Cote d’Ivoire9 that sought to understand women’s reasons for not participating in PMTCT follow up visits, found that negative experiences that women had had or expected to have during their interactions with health workers contributed to non-participation in PMTCT prophylaxis. Positive relationships between women and health workers are essential to prevent missed opportunities for PMTCT participation and innovative methods are needed address attitudes of health staff and fears amongst women. Infant feeding intentions of HIV positive women reflect facility and provincial policies, level of staff training and infant feeding counseling skills. It is clear from this evaluation that there are serious operational problems with the provision of free formula milk. The high rate of intentions to formula feed in rural areas suggests that either infant feeding counselling is not taking into consideration the home circumstances of mothers and the WHO10 AFASS guidelines (acceptable, feasible, affordable, sustainable and safe), or that the provision of free milk within a context of extreme poverty could be an incentive for women to choose this option when it may not be the most appropriate choice. It was evident from interviews with midwives and nurses that the provision of free formula does not necessarily ensure exclusive formula feeding or infant nutritional safety due to problems with the sustainability of supplies, confusion amongst health workers over how to counsel mothers on infant feeding choices and how to handle situations when mothers run out of supplies early. Some of these concerns and others are described in a recent report11 on UNICEF’s experiences with the distribution of free formula milk to HIV infected mothers in Africa. This report was released following the decision by UNICEF to stop supporting the provision of free formula milk in UNICEF-supported African PMTCT programmes. Evidence from this evaluation suggests the need for a similar review in South Africa and a subsequent re-consideration of the current infant feeding policy to determine whether it does more harm than good in this setting. A large proportion (50%) of the infants born to mothers who received nevirapine were not followed up and tested. The HIV status of these infants is therefore unknown and could vary from the results of infants that were followed up and tested. It is not possible to draw any conclusions on impact or effectiveness of the programme from this data. The high loss to follow up rate also means that the majority of infants born to HIV positive women will have their HIV infection status determined for the first time when they present with HIV disease and are not receiving routine medical care recommended for HIV infected children such as prophylactic co-trimoxazole. They also do not access other medical interventions that might benefit their health, such as nutrition support. Earlier infant testing with a more reliable test (such as a PCR), together with other forms of com-munity-based support may improve postnatal follow up. More importantly, it may allow health care staff to reaffirm with mothers the relative risks and benefits of different infant feeding practices on the health of their child. Despite this intervention being affordable in most developing countries and relatively simple in design, it is being introduced into already struggling health systems with severe human resource crises. Unless the health systems constraints identified in this evaluation are addressed any new health programme will struggle to reach optimal effectiveness. The pilot programme in South Africa has demonstrated that while the provision of nevirapine to HIV positive pregnant women and their newborns is a relatively simple and feasible medical technology, good coverage, high quality care and follow up of mothers and infants is much more difficult. The low uptake of HIV testing and poor coverage of nevirapine observed in this programme is inadequate, especially given the high HIV prevalence. A strengthening of the health system infrastructure, in particular management capacity, is required if PMTCT is to serve as a vehicle to improve broader maternal and child health services, and as an entry point into comprehensive HIV/AIDS treatment and care. AcknowledgementsThe authors would like to acknowledge the co-operation of individuals in the national and provincial Departments of Health who facilitated access to the research sites and were supportive of the evaluation. We also appreciate the efforts of the front line health workers who are implementing this programme and who allowed us to visit their facilities. This research was funded by the National Department of Health, South Africa. References
Copyright © 2005 - Makerere Medical School, Uganda |

{kind=link}
{kind=link}
{kind=link}