 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 5, No. 3, September, 2005, pp. 219-226 Heart disease among children with HIV/AIDS attending the paediatric infectious disease clinic at Mulago Hospital S. Lubega1, G.W. Zirembuzi2 P. Lwabi3 1. Paediatrician, Department of Paediatrics and Child Health/ Uganda Heart Institute, Mulago hospital. Correspondence author: Dr Sulaiman Lubega Department of Paediatrics and Child Health, Uganda Heart Institute, Mulago Hospital Kampala Email: lubsk2001@yahoo.com Code Number: hs05038 AbstractBackground: There are very few published studies of heart disease in HIV infected children living in sub-Saharan Africa, a region with more than 50% of the world’s population of HIV infected patients. HIV/AIDS is an important cause of childhood morbidity and mortality affecting more than 1.3 million children worldwide and 0.1 million children below 15 years in Uganda by the end of year 2001 1. The currently available anti-retroviral (ARV) drugs and treatment of opportunistic infections have converted HIV infection into a chronic illness 2. All body systems, including the cardiovascular system, may be affected by HIV disease 2. There are still very few HIV infected children accessing anti-retroviral therapy at the moment in developing countries because of financial constraints. Since ARV drugs do not eliminate the HIV from the body, their use may simply postpone the development of heart disease, yet some of these drugs like zidovudine are cardiotoxic themselves and have been associated with heart disease 3,4. As pulmonary diseases in HIV disease are more effectively prevented and treated, the proportional morbidity and mortality of heart diseases among children with HIV/ AIDS increases 5,6. Most of the published studies about heart disease in HIV/AIDS have been done in adults. The few published studies of heart disease among HIV infected children have used small sample sizes (of less than 50) 8-12 or were highly selective (including only children with symptomatic HIV disease or those who were very sick) 8,10,11. In many clinical situations, HIV infected children are not routinely evaluated by echocardiography. Previous studies have shown that heart diseases in HIV/AIDS patients are usually subclinical but may be severe. When the signs and symptoms of cardiac dysfunction are present, they are non-specific and often attributed to non-cardiac pathologies especially pulmonary disease 7,8. Objectives
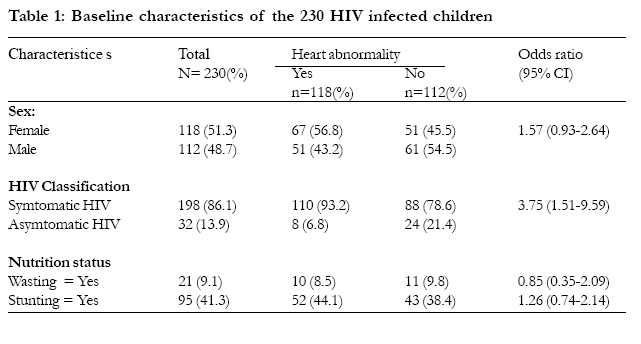
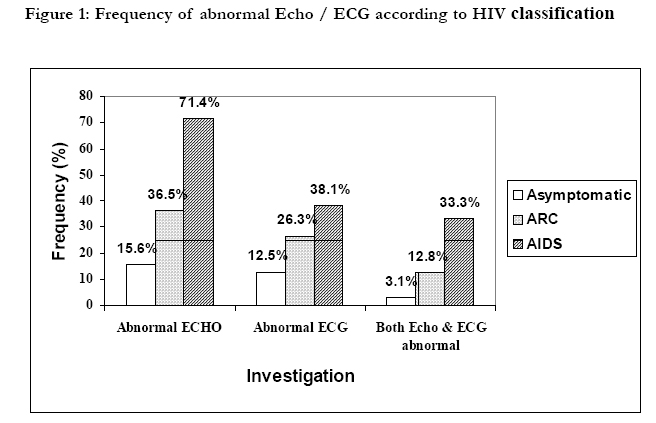
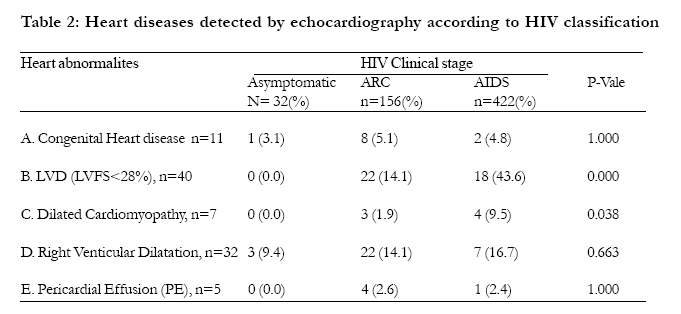
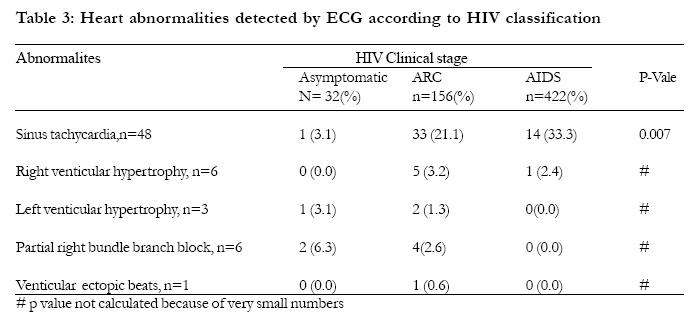
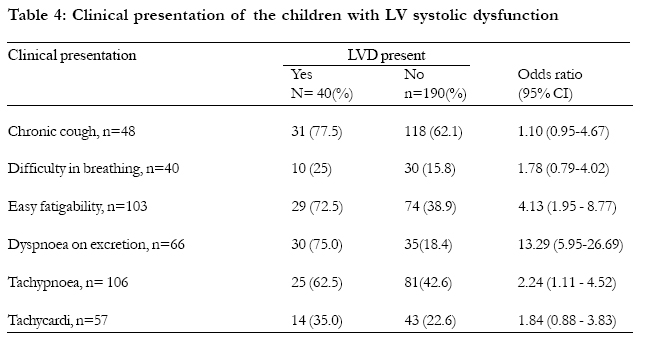
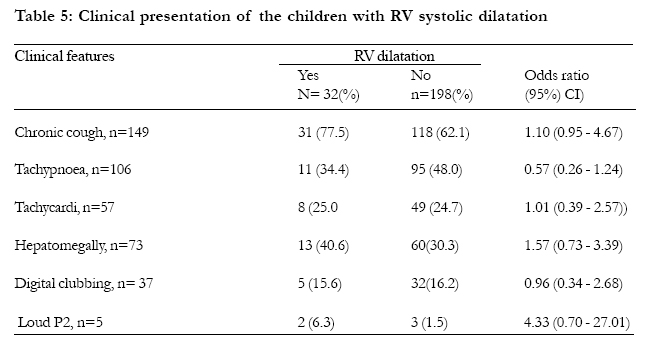
Methods Patients and Study centre Two hundred thirty (230) HIV infected children were recruited by simple random sampling in a crosssectional study between September 2002 and February 2003. All children had confirmed HIV status and were attending the Paediatric Infectious Disease Clinic (PIDC) at Mulago hospital on out patient basis. Only one child was on ARV drugs (zidovudine, lamivudine and nevirapine) for 2 weeks before being recruited in this study. All the children were evaluated clinically in PIDC and investigated by electrocardiography (ECG) and echocardiography (echo) in Uganda Heart Institute, which is also in Mulago hospital. Echocardiography (2-Dimesional, M-mode and Doppler evaluation)A cardiologist using the Hewlett Packard Sonos 1000 model echo machine did M-mode and 2dimensional echocardiography following the criteria of the American Society of Echocardiography. The transducer frequency was 3.5 or 5 MHz depending on the need. The subcostal view was got with the patient lying supine and was used mainly to assess anatomic relations and presence of congenital abnormalities. Parasternal and apical views were obtained with the patient in the left lateral or supine position depending on what gave the best view. Long parasternal views with M-mode were used for measuring the heart chamber dimensions in diastole and systole. Left ventricular fractional shortening (LVFS) was automatically computed by the machine and is the quickest and, for clinical purposes, usually sufficient to assess left ventricular function. All measurements were done twice and an average taken for intra-rater reliability. It was not possible to assess ventricular diastolic function because of time limitation. Doppler and color flow studies were done to study valve and orifice pressure gradient and directionality of blood flow. Continuos Doppler recordings were obtained, with the sample volume located between the tips of the valve. Regurgitation was considered mild if the back flow seen on colour Doppler did not reach the middle, moderate if the flow reached the middle, and severe if it exceeded the middle of the receiving chamber. Mode of diagnosis on echoLeft ventricular systolic dysfunction was defined as left ventricular fractional shortening <28%. Dilated cardiomyopathy was defined as left ventricular systolic dysfunction with bi-ventricular or left ventricular enlargement. Pericardial effusion (PE) was diagnosed when the effusion measured more than 4mm. Prolapsed mitral valve was diagnosed on the basis of: (i) thickening of the valve; (ii) left atrial systolic dislocation of one or both mitral leaflets from the mitral valve ring plane. Electrocardiography (ECG)The 12-lead standard ECG was done using the Hewlett Packard M1700A3412A08047 ECG machine. Heamoglobin(Hb) estimation was done using a colorimeter in the PIDC. Data AnalysisData was entered using EPI-1NFO 2000 and analysed using SPSS 10.0 computer software packages. Tests of significance were the Chi-square or Fisher exact test (whenever the expected frequency in one of the cells was less than 5) and odds ratios for categorical variables, and Analysis of variance or Student’s t-test for continuous variables. Differences between groups were considered significant at p<0.05. Ethical considerationPermission to carry out the study was obtained from the Department of Paediatrics and Child Health (Mulago hospital), Makerere University, Faculty of Medicine Research and Ethics Committee and Uganda National Council for Science and Technology. Informed consent was obtained from the caretakers of the children who participated in the study. ResultsTwo hundred and thirty (230) HIV infected children were recruited, of whom 112 were males and 118 were females. The children had a mean age of 6.8 years (range 10 months to 16 years, SD = 3.6 years). The mean haemoglobin concentration of all the children was 11.85g/dl (SD=1.66g/dl). There was no statistically significant difference between the mean age and mean haemoglobin of the children with and without heart abnormalities. Thirty-two children (13.9%) had asymptomatic HIV disease, 156 (67.8%) had mild to moderately symptomatic HIV referred to as AIDS related complex (ARC) in this study while 42 (18.3%) had late symptomatic HIV disease (Acquired Immune Deficiency Syndrome -AIDS). Table 1 shows the baseline characteristics of the 230 children studied. Heart abnormalities were significantly more common among children with symptomatic HIV compared to those with asymptomatic HIV disease (p=0.001). Prevalence of heart disease: Of the 230 children studied, heart abnormalities were detected by echo in 92 (40.0%) and by ECG in 61 (26.5%). Both echo and ECG were abnormal in 35 (15.2%) children. Overall, heart abnormalities were detected in 118 (51.3%) children by echo and/or ECG. Figure 1 shows that echo abnormalities were significantly more frequent in children with AIDS than in those with ARC (p=0.000), and more in children with ARC than asymptomatic HIV disease (p=0.037). ECG abnormalities were also significantly more common in children with AIDS than asymptomatic HIV disease (p=0.028) but not between children with AIDS and ARC or ARC and asymptomatic HIV disease. Types of heart abnormalities detected:Of 230 HIV infected children studied, 40 (17.4%) had left ventricular systolic dysfunction (LVD), 32 (13.9%) had right ventricular (RV) dilatation, 11 (4.8%) had congenital heart diseases (CHD), 7 (3.0%) had dilated cardiomyopathy (DCM) and 5 (2.2%) had Pericardial effusion (PE) (Table 2). Only LVD and DCM were significantly associated with having AIDS. Most of the abnormalities were found in children with ARC and AIDS. Among the children with CHD, 8 had atrial septal defect (ASD) while 3 had prolapsed mitral valve disease. No patient had vegetations seen on the heart valves. Doppler and colour flow mapping: Three children had pulmonary hypertension indirectly measured by doppler as tricuspid regurgitation of ≥30 mm Hg. All these children had symptomatic HIV disease (1 had ARC and 2 had AIDS). Of these, 2 had RV dilatation on echo but normal ECG while the third had RVH on ECG but no RV dilatation detected on echo. These 3 children were diagnosed to have cor pulmonale. Mild mitral regurgitation was found in 2 out of the 3 children with prolapsed mitral valve disease. Electrocardiographic findings:Sinus tachycardia was the most frequent ECG abnormality detected and was found in 48 (20.9%) out of the 230 children studied (Table 3). Other abnormalities were rare. The frequency of sinus tachycardia among children with ARC (21.2%) and AIDS (33.3%) was significantly higher than that of children with asymptomatic HIV disease (3.1%) [p=0.015, p=0.001 respectively]. This difference remained significant even after controlling for temperature and haemoglobin concentration. The frequency of sinus tachycardia in children with ARC and that in children with AIDS was not significantly different (p=0.100). Of the 6 patients with right ventricular hypertrophy (RVH), 1 had cor pulmonale while another 3 had RV dilatation on echo. Clinical presentation of the children with heart diseases: Clinically, only 5 children were suspected to have heart disease before the investigations. One of these had muffled heart sounds due to a moderate pericardial effusion (the child with endomyocardial fibrosis), another had a history of paroxysmal nocturnal dyspnoea, while the other 3 had loud pulmonary component of the second heart sound due to cor pulmonale. All the children had normal blood pressure and jugular venous pressures. The position of the apex beat was normal in all children including those with heart dilatation detected on echo. None of the children had hyperactive precordium, or heart murmurs. Three of the children studied had pedal oedema and this was thought to be nutritional because these children were wasted, had hypo-albuminaemia, and had normal ECG and echo. Of all the clinical features, only easy fatigability, dyspnoea on exertion and tachypnoea were significantly associated with LVD (Table 4). On logistic regression, only dyspnoea on exertion remained significantly associated with LVD. Only one of the children with LVD had a history of paroxysmal nocturnal dyspnoea. None of these children had oedema or gallop rhythm. Of the 40 children with LVD, 7 had either left ventricular dilatation or global heart dilatation and were thus diagnosed to have dilated cardiomyopathy (DCM). Almost all the children with DCM had easy fatigability, dyspnoea on exertion, cough, tachypnoea, tachycardia and hepatomegally. None of the clinical features shown in table 5 was significantly associated with RV dilatation. All the 3 children with cor pulmonale had symptomatic HIV disease and had a history of chronic cough, easy fatigability, digital clubbing and loud pulmonary component of second heart sound. Pericardial effusion (PE) One child with PE had muffled heart sounds on clinical examination and this child had moderate pericardial effusion and right ventricular endomyocardial fibrosis on echo. The other 4 children with PE were identified only on echo. None of the children with PE had a pericardial rub or tamponade. One of children with PE had chest pain and this child also had pneumonia confirmed on chest X-ray and was being investigated for PTB. DiscussionWorldwide, the extent of, and factors associated with cardiac abnormalities in pediatric HIV are yet to be fully known. Few studies 8-13 of cardiac abnormalities in HIV infected children have been published and most of these studies have been based on echo and ECG findings. Prevalence and type of heart abnormalities detected:The prevalence of heart abnormalities detected by echo alone among HIV positive children in this study was 40%. This prevalence falls within the range of 18% to 78% reported by previous studies 8-12. And the abnormalities detected were significantly more prevalent in children with AIDS (71.4%) compared to those with ARC (36.5%) or asymptomatic HIV disease (15.6%). The higher prevalence of heart abnormalities among children with AIDS is possibly due to the higher occurrence, during this stage of illness, of infections like Epstein-Barr virus, Cytomegalovirus, and Cryptococcus neoformans 14, and malignancies like Kaposi’s sarcoma 15 that are known to cause heart disease. Congenital heart disease (CHD) was found in 5% of all the children studied, a figure that is slightly higher than that from previous studies 2-3% 8,12,17 and higher than that found in the general population of 0.8% 16. The commonest congenital heart abnormality detected in this study was atrial septal defect and none of the children had a ventricular septal defect while previous studies 8,12,17 reported ventricular septal defect as the commonest. Our study found left ventricular systolic dysfunction (LVD) in 17% of HIV infected children, a prevalence that is within the range of 5% to 65% found in previous studies 9-12,18,19, and similar to other studies the occurrence of LVD was significantly associated with HIV disease progression. Prospective studies 10,22 have shown that LVD may progress to dilated cardiomyopathy (DCM). The prevalence of DCM in this study (3.0%), was lower than that reported by Sherron (45%) 10 and Lipshultz (16%) 12. The prevalence of RV dilatation of 14% in this study is slightly lower than that obtained by Kavanaugh-McHugh 23 of 18% and much lower than that reported by Bannerman et al.8 of 48%. Bannerman et al. 8 studied HIV infected children who were admitted in hospital most of whom had cough and respiratory distress unlike the current study. The prevalence of cor pulmonale in children with HIV in this study of 1.3% is lower than that reported by previous studies of 4% to 48% 8,10,23. Pericardial effusion (PE) was seen in 5 out of the 230 children (2.2%) and all these children had symptomatic HIV disease. Previous studies 9-12 have reported PE in 14% to 60% of HIV infected children while Starc et al. 18 found no PE in 201 children with HIV, majority of whom having symptomatic HIV disease. Chest X-rays of all children with PE showed cardiomegaly. Similar to previous studies, none of the children with HIV had rheumatic heart disease. The relationship between rheumatic heart disease and HIV infection is yet to be determined. The prevalence of ECG abnormalities detected in this study was 26.5%, which is lower than that previously reported by Issenberg et al. (55%) 10 and much lower than that of Lipshultz et al. 12 (93%) who used 24-hour ambulatory ECG in addition to the standard 12 lead ECG. Sinus tachycardia was the commonest ECG abnormality detected similar to other studies10,12. The frequency of sinus tachycardia among children with ARC (21.2%) and AIDS (33.3%) was significantly higher than that of children with asymptomatic HIV disease (3.1%) even after adjusting for haemoglobin concentration and fever in a multivariate analysis. The autonomic imbalance and neuropathy, which are present in early HIV infection and progress with worsening HIV disease 9, are possible explanations for the sinus tachycardia. Other ECG abnormalities were rare and asymptomatic. In general, previous studies 6-13 that recruited only children with symptomatic HIV disease or were prospective in nature or used children who were admitted in hospital reported higher prevalence of LVD, RV dilatation, pericarditis and ECG abnormalities compared to the current study. Clinical featuresAll the children with CHD were asymptomatic and detected only on echocardiography. In our study, easy fatigability, dyspnoea on exertion, tachypnoea were significantly associated with LVD. Dyspnoea on exertion was the only clinical feature independently associated with LVD on logistic regression. Eight HIV infected children with LVD previous studied by Stewart 20 all had chronic cough, tachycardia, tachypnoea, hepatosplenomegaly and difficulty in breathing. The clinical features of the children with RV dilatation in this study were non-specific. Bannerman et al. 8 previously found that RV dilatation and hypertrophy were significantly associated with chronic cough, respiratory distress and cyanosis. All the 3 children with cor pulmonale in this study had chronic cough, easy fatigability, loud P2 and digital clubbing, and had received a full course of anti-tuberculous drugs at least once with little or no improvement. Of the 5 children with PE in this study, only one child with moderate PE and endomyocardial fibrosis was clinically suspected before echocardiography on the basis of muffled heart sounds. One of the children with PE had disseminated Kaposi’s sarcoma. Four of the 5 children with PE had chronic cough and were being investigated for pulmonary tuberculosis, but none of them had fibrinous strands in the PE on echo that are characteristic of tuberculosis 24. Conclusions
The Austrian government through Horizont 3000 and the Nuffield foundation funded this research. We are grateful to the staff of the Department of Paediatrics & Child Health, Makerere University, PIDC and Uganda Heart Institute for their assistance during the research. References
Copyright © 2005 - Makerere Medical School, Uganda |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}