 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
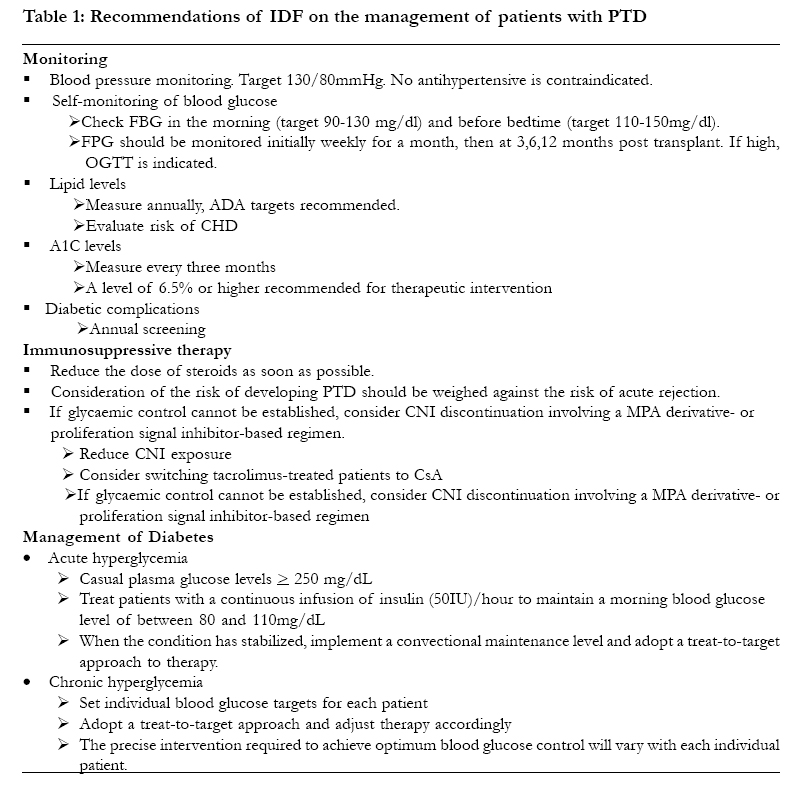
African Health Sciences, Vol. 5, No. 3, September, 2005, pp. 255-260 PRACTICE POINTS Natural history and epidemiology of post transplantation diabetes mellitus Olutayo C. Alebiosu 1 and Olugbenga E. Ayodele2 1 Olutayo C. Alebiosu, Supernumerary Consultant, Department of Medicine, University of Cape Town, Republic of South Africa. Correspondence author: Dr. Olutayo C. Alebiosu, Supernumerary Consultant, Department of Medicine, J-Floor Old Main Building, Groote Schuur Hospital, Observatory 7925, University of Cape Town, Republic of South Africa. Tel: +27-21-4045007, Fax: +27-21-4486815. Email: dralechristo@gmail.com Code Number: hs05043 AbstractObjective: High patient mortality continues to be the major threat to the success of solid organ transplantation despite improvements in the control of immunologic phenomena post-transplantation with improvements in grafts survival. Post transplantation diabetes mellitus (PTD) occurring commonly in patients receiving immunosuppressives has been identified as a major culprit. Keywords: Current concepts, Definition, Diabetes, Epidemiology, Pathogenesis, Post transplantation, Management. IntroductionPost transplantation diabetes mellitus (PTD) is a complication of solid organ transplantation, excluding pancreatic and islet cell transplantation. Despite the importance of this clinical condition, there was no consensus definition until recently. Evidence suggests that PTD has serious consequences for transplant recipients and threatens transplant outcomes. This condition increases the risk of graft – related complications such as graft rejection, reduced graft function, graft loss and infection1,2,3 and reduces the survival of transplant recipients4,5. It is also a major determinant of the increased cardiovascular morbidity and mortality seen in transplant recipients6. Following kidney transplantation, the costs of developing PTD have been estimated to be $12000 – $13000 higher than for those without diabetes by the end of the first year with these costs rising to $19000 - $22000 by the end of the second year7. This paper reviews the current concepts of post transplant diabetes. Research design and methods A Medline literature search limited to research / review articles in English language, spanning 1984 January – 2004 June on post transplantation diabetes mellitus or hyperglycemia was done. In reviewing the materials obtained, emphasis was on the definition, natural history, epidemiology and management of the condition. Definition of post transplant diabetes mellitus Until recently there was no consensus regarding the definition of PTD, but the term excludes pancreatic and islet cell transplantations. A recent guideline defined the condition as the occurrence of DM requiring insulin post transplantation8. Some workers defined the condition as fasting hyperglycemia exceeding 7.8mmol/L and the need for insulin therapy9. Others used an oral glucose tolerance test (OGTT) to define PTD10. Post transplantation diabetes mellitus is a heterogeneous condition of abnormal glucose tolerance with a variable onset, duration and severity. The definition and diagnosis of the condition has recently been based on the revised definition of diabetes mellitus and IGT recently adopted by the American Diabetes Association11,12. A recent guideline defined the condition as the occurrence of DM requiring insulin post transplantation7. Post transplantation diabetes mellitus is thus defined as a fasting plasma glucose (FPG) = 7.0 mmol / L (126 mg / dL) with no calorie intake for at least 8 hours and / or a 2 hour plasma glucose during an OGTT (2 hr PG) = 11.1mmol / L (200 mg / dL), or a casual plasma glucose = 11.1 mmol / L (200 mg / dL), on 3 or more occasions over a period of at least 3 months8. Natural history and epidemiology of post transplantation diabetes mellitusPost transplantation diabetes mellitus develops insidiously in kidney, liver or heart transplant patients during the first 6 months of transplantation on the average, but the incidence increases progressively with time13-16. Similar to the natural history of type 2 diabetes mellitus patients, patients are exposed to the damaging effects of uncontrolled hyperglycaemia during this asymptomatic period. Post transplantation diabetes mellitus, however, may resolve spontaneously without therapy17. Differences in diagnostic criteria of PTD have resulted in wide variations in the reported incidence of PTD. Such differences included non-exclusion of pre-existing diabetes mellitus, non-inclusion of OGTT in the definition and definitions based only on the patients’ requirements for insulin. Another reason is that at times patients are observed for short periods, which underestimates the true occurrence of the condition. Generally, the risk of developing PTD has been shown to increase progressively post transplant, with the condition being diagnosed in some patients up to 15 years after transplantation18. A retrospective analysis of Medicare beneficiaries in the United States showed that the cumulative incidence of PTD among 11,659 patients was 9.1, 16.0, and 24.0 % at 3, 6, and 36 months respectively5. Other reasons for variation may probably be related to differences in population demographics between studies: African – Americans and Hispanic populations have higher rates of both type 2 and PTD, related to genetic and, perhaps, pharmacokinetic factors, as there is reduced clearance of methylprednisolone in African – American compared to Caucasian men with PTD1. Generally, incidence rates of PTD have ranged between 2.0% and 57.1 %1,19. Recent systematic review of literature found that PTD was observed in 13.5% of patients after kidney, liver or heart and lung transplantation7. The incidence of PTD has been demonstrated to show a bimodal pattern corresponding to the early kidney transplantation era using high dose corticosteroids in the 1960s and to the introduction of tacrolimus in the 1990s. In a recent analysis, the type of immunosuppressive regimen used was found to explain 74 % of the variability in the incidence. The risk factors predisposing to the development of PTD after kidney, liver and heart transplantation include age, recipient’s ethnicity, immunosuppressive regimen and family history of diabetes7,12,20,21. Recipient’s age over 40 years is associated with increased prevalence of PTD. In a study by Cho et al, only the age at transplantation was associated future development of PTD on multiple logistic regression19. All patients over the age of 40 years developed PTD and the relative risk of age > 40 years in the development of PTD was 2.8 (95 % CI 1.39 – 5.66)19. Non-white patients experienced a twofold increase in the risk of PTD (RR – 3.3, 95 % CI 1.6 – 7.0). Hricik et al reported that African Americans were more susceptible to PTD than Caucasians despite similar doses of corticosteroids and lower trough level of tacrolimus23. Another well established risk factor in the development of PTD is the immunosuppressive therapy used with corticosteroids being associated with the greatest risk24,25. The incidence of PTD depends on the dose administered and the duration of therapy. Hjelmesaeth et al in a singlecenter prospective cohort study involving a total of 173 consecutive previously nondiabetic renal transplant recipients, 167 of which underwent a 75 g OGTT ten weeks after transplantation showed that the actual daily prednisolone dose was strongly associated with the development of PTD24. The calcineurins (CNIs) cyclosporine and tacrolimus have also been associated with an increased risk for PTD with the latter being up to five times more diabetogenic than cyclosporine5,26,27. Tacrolimus was found to be an independent risk factor for PTD in a recent analysis of Medicare beneficiaries in the United States receiving kidney transplants between 1996 and 2000 (RR 1.53; p < 0.0001)5. The cumulative incidence of diabetes after transplantation at 3, 12 and 36 months for patients receiving tacrolimus were 13.5, 22.1, and 38.1 % respectively compared with 7.8, 14.2, and 21.9 % for those not receiving tacrolimus5. Tapering off of prednisolone but not cyclosporine A (CsA) also significantly improved glucose tolerance during follow-up period24. There is strong evidence that individuals with a family history of diabetes among first degree relatives have an increased risk of developing PTD28,29. Hathaway et al in a prospective study including 86 patients followed for at least 18 months post transplantation reported that a family history of diabetes was an independent risk factor for PTD (OR 5.00)28. Other not too-well established risk factors that have been associated with increased risk of PTD include abnormal glucose regulation pretransplantation or other components of the metabolic syndrome (for example, hypertriglyceridemia, hypertension, and hyperuricemia), acute rejection, higher body mass index (obesity), transplantation with a cadaveric kidney and transplant infection with hepatitis C virus particularly when patient is on tacrolimus8,13,30-32. Health implications of posttransplantation diabetesDiabetes is the most common cause of end stage renal disease in Europe, United States and Japan. The development of the condition post transplant is associated with impaired long-term graft function and survival in transplant recipients. The development of PTD has been reported to be associated with a significant decrease in renal graft survival at 3 and 4 years, compared with recipients with no diabetes (3yr -71% vs 86%, p<0.05; 4yr 54% vs 82% p<0.05,; 12 yr - 48% vs 70%, p=0.04) 1,2. A recent meta-analysis has also revealed that the development of PTD was associated with a 63% increased risk of graft failure and a 46% increase in the risk of death-censored graft failure (p<0.0001 vs no diabetes for both comparisons) 5. In liver transplant recipients, the incidence of acute rejection episodes was found to be higher in patients who developed PTD (50 vs 30% in the control group)16. It has also been shown that the long term survival of kidney transplant recipients who developed PTD is reduced compared with those without PTD (8.1 years vs 11.0 years)4. Post transplantation diabetes predisposes transplant recipients to cardiovascular disease and increases the risk of death from cardiovascular complications6. Death resulting from ischaemic heart disease is 20.8 times higher in transplant recipients with diabetes than in the general population34. PathogenesisAlthough the degree of diabetogenicity varies, immunosuppressants account for the greater majority of PTD35 . Corticosteroids have the greatest risk of PTD after kidney24, liver and heart36 transplantation. PTD due to the effects of corticosteroid therapy is related to both the dose and duration of treatment. The main pathogenesis is the development of insulin resistance evident as an increase in glucose production by the liver and a decrease in glucose uptake by the peripheral tissues1,9,24,36. Insulin response to oral glucose is also reduced following corticosteroid administration. In the case of calcineurin inhibitors, both cyclosporine (CsA) and tacrolimus have diabetogenic effects, though the balance of evidence across all organs suggest that tacrolimus is more diabetogenic than CsA. The main mechanism underlying the diabetogenic effects of cyclosporine and tacrolimus are due to a number of mechanisms including pancreatic beta-cell toxicity, decreased insulin synthesis and decreased insulin secretion4. Drachenberg et al reported cytoplasmic swelling, vacuolization, apoptosis and abnormal immunostaining of islet cells in patients treated with CsA or tacrolimus37. Islet cell damage appears to be more severe in tacrolimustreated group than the CsA-treated group37. Cyclosporine A inhibits both DNA and mRNA synthesis and tacrolimus disrupt the transcription of insulin mRNA4. ManagementPretransplantation Patients should be screened for risk factors for PTD enumerated earlier. Because transplant patients also have an increased risk of developing cardiovascular disease, they should be screened for cardiovascular risk factors and metabolic syndrome8. The information so obtained will help in selecting the appropriate immunosuppressive therapy. Selection of an appropriate immunosuppressive regimen should take into account individuals diabetes risk profile and the relative diabetogenicity and risk for diabetes of each immunosuppressant, balancing minimal risk of diabetes with effective immunosuppression. Patients should be counseled on the importance of weight control and exercise since they are prone to weight gain post transplant which potentially increases their risk of developing PTD38,39. Post transplantation Fasting plasma glucose should be monitored in patients post transplant at least weekly in the first 4 weeks after transplantation, then at 3-, 6-, and 12-month intervals and annually thereafter8. In patients at risk of developing PTD, the dose of corticosteroids should be reduced as soon as possible since this has been shown to improve patient’s glucose tolerance. This reduction, however, should be balanced against the possible increased risk of graft rejection associated with such reduction25. Patients who develop PTD on tacrolimus can be switched CsA which is less diabetogenic. Table 1 summarizes the recommendations of IDF on the management of patients with PTD11. ConclusionPost transplantation diabetes mellitus is a heterogeneous condition of abnormal glucose tolerance with a variable onset, duration and severity. Differences in definition have resulted in wide variations in the reported incidence. The most important risk factor predisposing to the development of PTD is the immunosuppressive drugs. Patients with PTD have poorer outcomes including impaired graft function and survival. *This paper was written while the lead author was in the University of Cape Town, Republic of South Africa, sponsored by the World Diabetes Foundation / International Diabetes Federation Fellowship grant (June-August 2004). References
Copyright © 2005 - Makerere Medical School, Uganda |

{kind=link}