 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
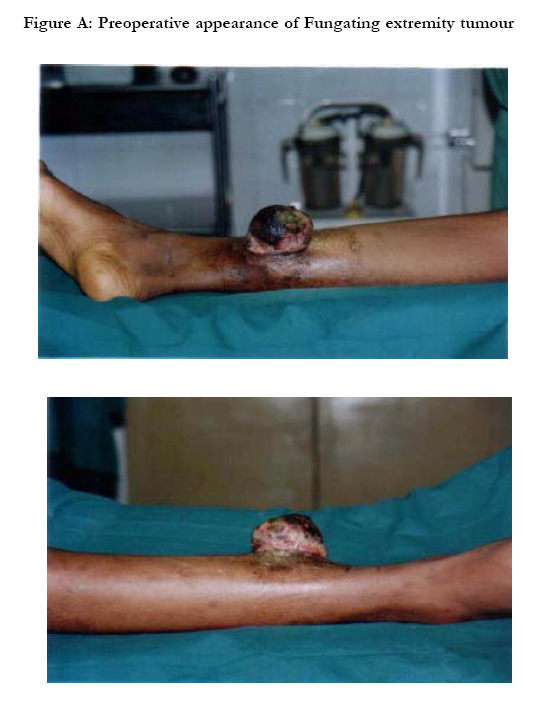
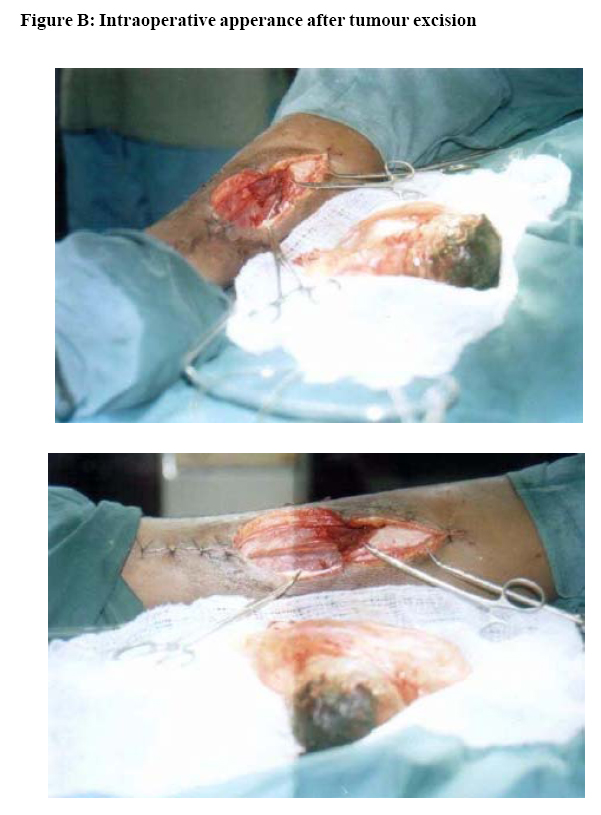
African Health Sciences, Vol. 5, No. 3, September, 2005, pp. 261-264 CASE REPORTS Extremity haemangiopericytoma, a case report from Nigeria Lateef O. A Thanni Department of Orthopaedics and Traumatology, College of Health Sciences, Olabisi Onabanjo University, Sagamu, Ogun State Correspondence author : Lateef O. A Thanni Department of Orthopaedics and Traumatology, College of Health Sciences, Olabisi Onabanjo University, P.M.B. 2022 Sagamu, Ogun State Email : loathanni@yahoo.com Code Number: hs05044 AbstractHaemangiopericytoma is an uncommon soft tissue sarcoma of vascular origin. It occurs more frequently in the extremities than elsewhere in the body although it can arise in any organ. Wide surgical excision is the mainstay of treatment. However, adjuvant radiotherapy and chemotherapy are desirable because the malignant nature of this tumour is frequently unpredictable. Adjuvant therapy is recommended for metastases, recurrence and incomplete resection. Long term follow up is essential in all cases as recurrence can occur several years after treatment. Where little or no experience with managing this tumor exists, it is important to be aware of its clinical behaviour and the treatment options, hence this case reports. Key words: haemangiopericytoma, sarcoma, tumour, radiotherapy, chemotherapy IntroductionHaemangiopericytomas are soft tissue sarcomas of vascular origin, comprised of pericytes1. Stout and Murray first described the tumour in 1942 in the lungs2 but it can occur anywhere in the body. The tumour has been reported to occur in the extremities, pelvis3, head and neck4, back, retroperitoneum and abdomen5. Primary central nervous system occurrence has also been reported6. Manifestation in bone is extremely rare but has been reported in a foot bone7. This special tumor always shows a questionable prognosis and, by histological investigations, it cannot be decided if we are dealing with a benign or malignant tumour growth8. Enzinger and Smith9 have suggested that malignancy can be predicted from a large tumour size, presence of necrosis, increased cellularity and over 4 mitoses per high power field. However, clinical tumour behaviour and the occurrence of distant metas tasis may be the only way to confirm the malignant nature of the tumour. Metastasis or local recurrence may occur after several years. This is the first report of extremity haemangiopericytoma from our center. Where little or no experience with managing this tumor exists, it is important to be aware of its clinical behaviour and the treatment options, hence this case report. Case Report A 22 year old male patient was seen in March 2002 with a 3 month history of spontaneous right leg swelling. There was associated pain while walking but no pyrexia. It was slowly progressive in size until 2 weeks before presentation when a rapid increase in size was noted. There was no weight loss. Examination revealed a healthy looking male patient with a 5cm by 5cm swelling on the posteromedial aspect of the right leg. It was firm, non tender and non pulsatile. Overlying skin was not warm and there was neither palpable popliteal lymphadenopathy nor significant inguinal lymphadenopathy. Radiological examination of the affected leg showed soft tissue swelling but normal right tibia. Chest X-ray was normal. White blood cell count (WBC) revealed a relative lymphocytosis of 78% and neutropenia of 22% (total WBC 8500 per cumm). He was HIV negative.The patient thereafter defaulted for 5 months. By this time, the swelling was 12cm by 12cm when an incisional biopsy was done. The biopsy, on histological examination, showed cellular connective tissue neoplasm comprising proliferating spindle cells interspersed by prominent focally dilated vascular channels. There was low mitotic activity but mild pleomorphism but no area of necrosis. A diagnosis of haemangiopericytoma was made. Excision of the tumour was performed about 7 months after initial presentation. A fungating soft tissue tumour was found, figure, attached to the lower fleshy part of the soleus muscle. The tumour was excised enbloc with overlying skin and a wide portion of the attached soleus muscle. The dorsal part of Achilles tendon was preserved. The posterior tibial neurovascular bundle was intact. The wound healed primarily but a month postoperatively, a painful tender swelling developed in the scar and discharged pus from which pseudomonas specie was isolated. The swelling resolved with oral ciprofloxacin. He was referred for radiotherapy but did not commence this until about 9 months later. He was reported to have died suddenly of pulmonary complications while undergoing radiotherapy. Autopsy was reportedly not performed. Discussion Prediction of the clinical behaviour of haemangiopericytoma is considerably difficult. This may be because it is a heterogeneous entity with specific component variants that are yet to be identified. Lipomatous haemangiopericytoma is a benign variant that has more recently been described10. Identification of such variants will make management decision easier. Wide surgical excision is the treatment of choice11,12,13. However because of the unpredictable malignant behaviour of the tumour, adjuvant therapy is desirable. Haemangiopericytoma is poorly radiosensitive but radiotherapy has been used with some success11,14. Primary and metastatic tumours are chemosensitive11. Chemotherapy with methotrexate, actinomycin D, Cyclophosphamide and vincristine in various combinations has also been used with success11. Combined radiotherapy and chemotherapy is to be recommended for metastasis, recurrence and inadequate excision. Patient should be followed up regularly because of local and distant tumour recurrence15. Recurrence can occur several years after treatment, as long 26 years later16. Pulmonary metastasis can be fatal due to complicating pneumothorax17 and haemothorax18. It is possible that the patient in this report died suddenly of such complications despite the fact that the tumour showed little mitotic activity and no area of necrosis. The delays in making a diagnosis and getting adjuvant radiotherapy, occasioned by the patient’s default in hospital attendance may have contributed significantly to the adverse outcome. References
Copyright © 2005 - Makerere Medical School, Uganda |

{kind=link}
{kind=link}