 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
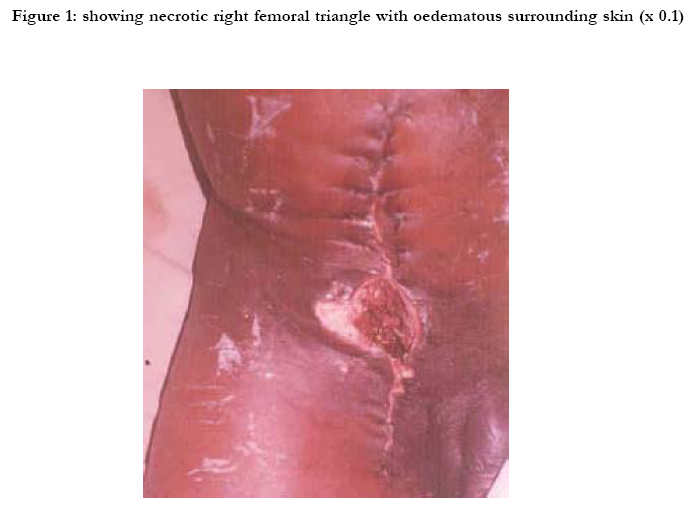
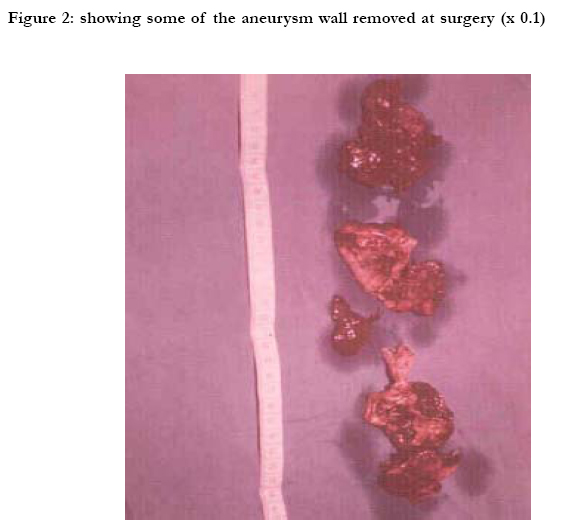
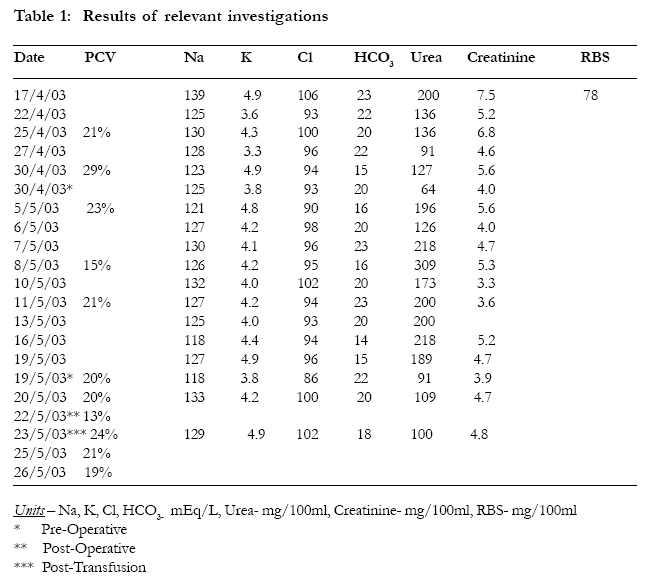
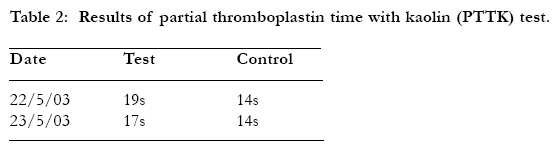
African Health Sciences, Vol. 5, No. 3, September, 2005, pp. 265-269 Ruptured false iliac artery aneurysm - a case report from Nigeria *A. A. Musa1 , C. O. Alebiosu2, O. Akiode3 and A.M.O. Shonubi4 1Department of Surgery, Olabisi Onabanjo University Teaching Hospital, Sagamu, Nigeria, Correspondence author: Dr. A. A. Musa Department of Surgery, Olabisi Onabanjo University Teaching Hospital, PMB 2001, Sagamu, Nigeria Email: alwajud 1423@ yahoo.com. Mobile: 0234 – 8023250865 Code Number: hs05045 SummaryA 23year old male Nigerian presented to the Nephrology unit of the Olabisi Onabanjo University Teaching Hospital, Sagamu, Nigeria with features of chronic renal failure secondary to chronic glomerulonephritis. He was referred to the surgical department of the hospital on account of severe torrential uncontrollable bleeding from an infected cannulation site. He was maintained on regular hemodialysis but developed femoral triangle sepsis at the cannulation site and aneurysm of the external iliac artery. The aneurysm later ruptured with severe jet exsanguinations bleeding. Exploration revealed a-4cm rent in the external iliac artery that was sutured with 6/0 prolene, interrupted, using clamp and suture technique. Perfusion was satisfactory in the immediate post-operative period. The patient was transfused with 11 pints of blood within 12 hours and had an uneventful post-operative period. Keywords: Haemodialysis, False iliac artery aneurysm, Femoral triangle Sepsis, Nigeria. Introduction Modern haemodialysis requires repeated reliable access to blood vessels capable of providing rapid extracorporeal blood flow. This necessity for reliable access to the circulation is the Achilles’ heel of modern haemodialysis1. Native and synthetic arteriovenous fistulas remain the preferred method of maintaining long-term haemodialysis access1 . The optimal vascular access is unquestionably the autologous arteriovenous fistular 2. Vascular access can also be gained through the use of catheters inserted into major vessels such as the subclavian vein, superficial jugular vein or femoral vein3. The advantages of vascular access using a catheter are avoidance of cardiac overload by blood shunting and the ability to start dialysis without blood access surgery Vascular access dysfunctions (thrombosis and infection) are the most common3 complications encountered in the care of end-stage renal disease patients 1,4. Butcher knife injury was a common cause of death by rapid exsanguinations. This usually results from perforation of the femoral artery in the femoral triangle. This injury is no longer common. Femoral aneurysms have been reported occurring due to trauma to vessel 4 We report a case of profuse bleeding from ruptured aneurysm of the external iliac artery following cannulation for haemodialysis. The objective of this paper is to highlight another cause of false iliac artery aneurysm and its management. Case report A 23year old polytechnic student, male, Nigerian was first seen at a private hospital in January, 2003 and managed as a case of chronic renal failure secondary to hypertension having been ill for 9 months. He had associated headache, fever, repeated seizures and was thought to have uremic encephalopathy. On presentation to the physician at the Olabisi Onabanjo University Teaching Hospital, Sagamu, Nigeria four months later, additional history of leg swelling of 4 months duration was obtained. A diagnosis of chronic renal failure secondary to chronic glomerulonephritis was made. He had his first hemodialysis within a week of presentation. On the second day of dialysis he started bleeding from the cannula site on the right thigh loosing about 800mls of blood. The cannula was removed on the third day on account of continued bleeding. The bleeding did not stop despite removal of catheter. This was initially attributed to bleeding tendency secondary to chronic renal failure. Pressure packing was applied. A new cannula was inserted on the left side and he received the second and third sessions of hemodialysis. Broad-spectrum antibiotics were commenced for what was thought to be extensive cellulitis involving the thigh and extension to the penis. Pus discharge cultured from the cannula site grew Staphylococcus aureus sensitive to ofloxacin. The right lower limb gradually became more swollen than the left and the inguinal cellulites persisted. The fourth dialysis was done on the 14/05/03. He lost further 700ml of blood from the initial cannula site on the right side on the 19/05/03. The surgical team were invited to review the patient, with torrential bright red bleeding which was not controllable by pressure. A diagnosis of femoral arterial bleeding to rule out bleeding arteriovenous fistula was made. There was no peripheral pulsation in the right lower limb before surgery. It was also edematous cold and dusky. The patient was prepared for an emergency exploration, control of bleeding and possible vascular repair as a combined team of surgeons. Under general endotracheal anaesthesia, exploration was carried out. Operative findings were oedematous dusky skin over the inguinal region extending up to the right costal margins, severe jet bleeding, circular cannulation site measuring 4cm in diameter at the right femoral triangle with necrotic tissue at the base. Via a 20cm long longitudinal incision over the line of femoral artery, incising the inguinal ligament, exploration revealed massive blood clot in the inguinal region of about 1 litre and huge friable-ruptured aneurysmal tissue. Figs I & II. There was intramuscular haematoma and a 3cm laceration of the anterior wall of the external iliac artery 4cm above the inguinal ligament. The external iliac vein and femoral vein were intact. The rent in the external iliac arterial wall was repaired with one layer suturing using 6/0 prolene interrupted suture. Perfusion was satisfactory in the immediate post-op period. The peripheral pulsations returned almost immediately after the vessel repair and the capillary refill was satisfactory. Patient made uneventful post-op recovery. A total of 11 units of blood were given to the patient in less than 12hours. Patient was commenced on Clexane along with Ceftriaxone. Discussion Access for haemodialysis are usually through arteriovenous fistula, and major renal cannulations 5. Access via major vessels for short-term angioaccess for haemodialysis may be obtained by insertion of catheters into the subclavian, internal and external jugular veins or femoral vein 6. Various complications may follow creation of shunts for arteriovenous access in haemodialysis. These include thrombosis, bleeding, skin erosion, catheter related infection and false arterial aneurysm5. False aneurysm of the femoral / external iliac arteries is often iatrogenic and could occur following percutaneous cannulations, or graft dysfunction 5, 7 The pathogenesis is that it occurs when a punctured site does not seal and a perivascular haematoma forms with a central area that remains fluid. The incidence of false aneurysm of femoral / external iliac artery is increasing from 0.6-1.0% 5,7,8. However, that of anastomic false aneurysms occurs with an increasing incidence of 1.5% to 3.0% 9,10. Aetiologic factors include host vessel degeneration, femoral triangle sepsis, prosthetic dilation and suture deterioration. Other risk factors include use of large-bore catheters, female gender, use of anticoagulant and thrombolytic agents and inadvertent cannulation of deep femoral or superficial artery 1,11. In this patient, the possibilities include femoral triangle sepsis and inadvertent cannulation of the external iliac artery. External iliac aneurysms are often symptomatic and grow rapidly especially when there is femoral triangle sepsis. It may present as a groin mass, which may be pulsatile. May thrombose and rupture spontaneously and bleed profusely 12,13 which was likely to be the case in this presentation. Colour flow duplex ultrasonography and angiographic studies are useful in the diagnosis of the ones that have not ruptured 14. Whenever they occur treatment is surgical exploration usually through a long longitudinal groin incision over the femoral artery. Control of bleeding is gained by proximal and distal clamping and starting the patient on anticoagulant. The aneurismal wall can be resected and the laceration on the arterial wall can be repaired using 6/0 prolene by interrupted suturing. Our patient had the above procedure and the perfusion was satisfactory in the immediate post operative. There was immediate return of peripheral pulses and capillary refill in the right lower limb. Another method of repair is the use of ultrasound probe to compress the aneurysm and the track; this results in thrombosis 15-18. We were unable to use this method because of lack of such facilities in our hospital. The largest series reported is from the Cleveland Clinic where successful and satisfactory closures were recorded in 94 of the 100 patients with post catheterisation aneurysm 15,16,19. Nonetheless, some could spontaneously thrombose and the tract sealed up without any residual complications. But be that as it may, for infected, rapidly expanding, very large and ruptured ones, surgery remains the best procedure of choice as in the case reported. Tables 1 and 2 show the biochemistry of the patient. The prolonged PTTK (Partial Thromboplastin Time with Kaolin) reflects the bleeding disorder of uraemia. Using the Cockcroft–Gault formula, the creatinine clearance of the patient was about 7.6mls/min at presentation. This did not change much after the dialysis sessions offered to the patient. Thus it can be inferred that the patient presented late to the nephrologist. A recent study showed that most renal patients in our hospital presented late 20. Given the fact that early referral to the nephrologist is likely to result in optimal pre-dialysis care, the recommendation is now that referral of a patient to a renal team should occur at a serum creatinine of 1.5mg%(132.6Umol/L) in women and 2.0mg%(176.8Umol/L) in men 21. Economic and clinical considerations strongly argue in favour of early referral of chronic uraemic patients. Early presentation will allow for appropriate and adequate preparations such as instituting measures aim at delaying renal failure progression, creation of arterio-venous fistula and prevention of complications. This case has been presented to call the attention of nephrologists to the possibility of a likely occurrence of such cases in our environment in view of the urgent attention it deserves. References
Copyright © 2005 - Makerere Medical School, Uganda |

{kind=link}
{kind=link}
{kind=link}
{kind=link}