 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
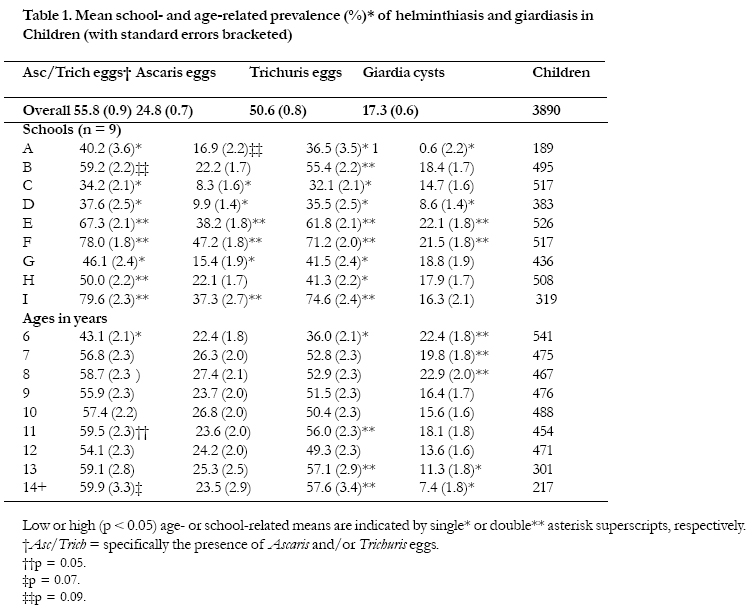
African Health Sciences, Vol. 5, No. 3, September, 2005, pp. 276-280 ERRATUM Paradoxical helminthiasis and giardiasis in Cape Town, South Africa: epidemiology and control Vera J. Adams1 , Miles B. Markus2, Joanita F.A. Adams3 , Esme Jordaan1, Bronwyn Curtis1, Muhammad A. Dhansay1, Charlie C. Obihara4 , John E. Fincham1 1 Medical Research Council of South Africa, Cape Town, South Africa. Corresponding Author: John E. Fincham Medical Research Council of South Africa P. O. Box 19070, Tygerberg South Africa 7505 E-mail: john..ncham@mrc.ac.za Phone: +27 21 938 0482. Fax +27 21 938 0832 Code Number: hs05047 Abstract Background: South Africa has endorsed a World Health Assembly (WHA) resolution calling for control of soil-transmitted helminths (STHs). In Cape Town, services and housing that exist in old-established suburbs should minimise the prevalence of intestinal parasitic infections, even when residents are poor. Where families live in shacks in densely-populated areas without effective sanitation, more than 90% of children can be infected by STHs. The humoral immune response to worms theoretically favours infection by Mycobacterium tuberculosis and HIV. Key words: Ascaris; Enterobius; HIV/AIDS; hookworm; IgE; Trichuris; tuberculosis Introduction World Health Assembly (WHA) resolution 54.19 of May 2001 calls for control of soil-transmitted helminthiasis and schistosomiasis, mainly because of the huge burden of subclinical morbidity that these diseases cause in children and women1-4, although worm infestation is also associated with serious clinical disease and mortality1,3,5. WHA member states, including South Africa, were urged to implement regular, non-selective deworming of school-age children and young women by 2010 in areas where the prevalence of worm infestation is 50% or more. As of January 2005, South Africa was still drafting national guidelines for the control of soil-transmitted helminthes (STHs) and schistosomiasis, in line with the WHA resolution. Direct responsibility for service delivery to the public lies with provincial health departments in nine provinces. However, participation by the education services as well as non-governmental organisations and the public, private and research sectors, is crucial in order to increase capacity, spread responsibility, generate con.dence and monitor progress. In terms of this overall process, no regular, synchronised, sustained, schoolbased deworming has yet been carried out in South Africa; but treatment is available at health facilities for pre-school children and symptomatic cases. In the Western Cape province of South Africa, research projects to help resolve practical, operational and legal issues around school-based deworming have made progress5-9. Surveys at 46 primary schools serving oldestablished, mainly Afrikaans- speaking, urban and rural communities within a 150 km radius of Cape Town have revealed a median school-based STH prevalence of 41% (range 7%-83%)5-8. In newer, slumlike areas in the city that have been formed by a rapid influx of mainly Xhosaspeaking people from the Eastern Cape province, more than 90% of children can be infested by Ascaris and/or Trichuris5,9. The existing parasitological background emphasizes the need for current information for traditional, mainly Afrikaans-speaking communities in Cape Town where the average income of families is low but services that are required for non-medical prevention of infection by STHs and intestinal protozoa have been in place for a long time (e.g. > 25 years). Based on this need, a cross-sectional study was undertaken at all the primary schools in a traditional area (as defined above). A general objective was to achieve broad-based estimates of the prevalence of helminthiasis and giardiasis by obtaining faecal samples from a high percentage of children attending all the schools in the community. Specific objectives were to define gender-, age- and school-related prevalence of infection; make a preliminary epidemiological assessment of possible sources of infection and means of transmission; alert health services to the need for control measures and the threat from protozoal pathogens, as necessary; and warn that co-endemic TB10 and HIV/ AIDS10,11 may use the immune response to intestinal parasites opportunistically2,3,8,12,23. MethodsThe study was based on nine primary schools serving a community of ~40 000 people, which is representative of a large proportion of mainly Afrikaans-speaking, traditional inhabitants of Cape Town. The study area lies in the southern part of the suburb of Parow. The community was targeted because although families living there are relatively poor, a comprehensive range of services and good housing have been in place for >25 years. The existing services include clean water, flush toilets, garbage disposal, clinics, electrification and macadamized roads. When the study was undertaken, there were 5607 pupils in the schools, the confirmed TB case rate in the community was 320/100 000, and 5.2% of women attending antenatal clinics were seropositive for HIV10. The intention was to obtain broad-based estimates of the prevalence of infection by STHs and Giardia by obtaining faecal samples from a large majority of the schoolchildren by non-selective sampling. Therefore, all the children were invited to provide faecal specimens. In addition to determination of the effectiveness of existing, non-medical preventive services, this approach was aimed at meeting the specific objectives of analysis of prevalence in relation to gender, school and age and consideration of potential sources of infection, African Health Sciences Vol 5 No 3 September 2005 aspects of transmission, and possible explanations for data trends. Permission to undertake the study was obtained from the Ethics Committee of the South African Medical Research Council, and was approved by the school committees, parents or guardians. Children participated voluntarily. Each child was given a thread-topped, sterile container identified by a numerical code, in which to place a faecal specimen. School nurses, researchers and parents assisted children. The only reasons for exclusion were a sample that was too small to use or damage to the code label that made it unclear. A standard formol-ether concentration technique was used to process the specimens24. For quality control, two experienced microscopists worked independently to detect the presence of worm eggs and Giardia cysts in faecal subsamples. The influence of gender, age and school as independent variables on the presence or absence of eggs and cysts in faeces as dependent binary variables (1= present and 0 = absent) was determined by logistic analysis of variance (SAS version 9.1). Wald chi-square statistics were used to test for differences in mean prevalence for age and school. Nine discontinuous age classes were based on the number of birthdays elapsed. A probability of less than 5% was interpreted as signi.cant (p < 0.05). All children in the schools, including those who did not provide faeces, were dewormed with mebendazole (Vermox®, Janssen-Cilag) after the faecal samples had been collected. Current sewage processing and disposal methods used in Cape Town were ascertained by means of correspondence with the city’s Wastewater Department and discussion with personnel. The city follows national guidelines that were first published in 1997 and amended in 200225. ResultsA large majority of children provided faecal samples. Overall compliance was 72.6% (4069/5607), with a school-based range of 67.9% -78.3%. The usable samples were from 1935 boys, 1936 girls and 19 individuals for whom gender was not recorded (n = 3890), after 179 specimens had been discarded because damage to labels had obscured the code and/or the quantity of faeces was too small. Results for boys and girls were combined because gender did not influence the prevalence of Ascaris, Trichuris or Giardia significantly, whereas age and school did. The data and significant differences (p < 0.05) are summarized in Table 1. Concurrence between microscopists was 100% for detection of Ascaris and Trichuris eggs and exceeded 96% for all other results. The overall infection rates for STHs and Giardia, based on a single faecal sample from each child, were 55.8% (SE 0.9%) and 17.3% (SE 0.6%), respectively. The true prevalence of giardiasis will exceed that detected because the cysts are shed intermittently 26, 27. School-related prevalence differed for Ascaris, Trichuris and Giardia. In five schools, STH prevalence ranged from 50.0% to 79.6%, which indicates the need for school-based deworming according to WHA criteria. In the other four schools, the STH prevalence range was 34.2%-46.1%. Age-related prevalence of ascariasis did not differ in children between six and 14 years old, whereas that of trichuriasis was higher in those who were 11, 13 and 14 years and 14-yearolds. Eggs of the dwarf tapeworm (Hymenolepis nana) were present in 2.2% (SE 0.23) of all samples, with a school range of 0.3%-4.6%. Enterobius eggs were seen in 25 faecal specimens, which underestimates prevalence because perianal sampling is necessary26,28. Hookworm-like eggs were detected in three specimens (prevalence 0.08%; SE 0.05), all of which also contained eggs of other STHs. Four children passed Trichostrongylustype eggs in their faeces (prevalence 0.1%; SE 0.05). Enquiry-based research revealed that in Cape Town, sewage sludge is processed according to national guidelines that do not specify destruction of worm eggs or protozoal cysts as a requirement25. Total sludge production is about 53 000 tons per year on a dry basis. About 32 000 tons (~60%) is partially dried (solids content ~14%) and sold to farmers on condition that it must be ploughed into the ground for growing cereals or grass but not other crops. This component will contain viable helminth eggs and protozoal cysts. The remainder is either pelletised at temperatures between 120oC and 350oC (~16 000 tons, i.e. 30%), or composted at temperatures exceeding 75oC for five days inside the rows (~5 000 tons, i.e. 9%). Temperatures in the pelletising processes will destroy eggs and cysts, but some could survive composting if the maximum temperature does not reach all parts of the product. More than 90% of the water component of sewage, comprising ~550 megalitres a day, is discharged into rivers as liquid effluent, and will contain helminth eggs and protozoal cysts. The rivers flow into the sea within the city limits, sometimes close to recreational beaches. About 6% of raw sewage is pumped directly into the sea, mostly through long pipelines. The salinity of sea water is such that it should sustain the viability of helminth eggs, and probably protozoal cysts as well. DiscussionMany communities throughout South Africa do not have the public health services or quality of housing that are available at the study site5,8,9. This reinforces the need to implement WHA resolution 54.19 wherever the prevalence of STHs is high. The resolution does not cover Enterobius or Hymenolepis, both of which occur in the community studied and elsewhere in the country28. Therefore, control measures should cater for all endemic helminths. Additionally, pathogenic intestinal protozoa can sometimes be an even more serious health threat than worms, both locally and on other continents. In Cape Town, an outbreak of amoebiasis occurred 14 kilometres from the centre of the city in 198429. In South Milwaukee in the USA, the largest epidemic of waterborne infectious disease ever recorded in a well-developed country affected 403 000 people in 1993. The causative organism was Cryptosporidium and the source was leakage of sewage into the water supply30. Infected people developed diarrhoea of varying severity, several immunocompromised individuals died and the overall cost was enormous. The occurrence of Cryptosporidium in South Africa has frequently been shown whenever appropriate staining techniques31 have been used. Trends in the STH infection rates at the study site indicate that classical exposure to embryonated eggs in soil through behaviour characteristic of gender and age was probably not the main source of infection. On the contrary, involuntary exposure through contamination of food and possibly drinking water, by STH eggs and Giardia cysts appears to be taking place. This would explain why there was no gender difference in prevalence, and why the prevalence of ascariasis did not differ significantly with age. That trichuriasis was significantly more prevalent in older children is not contradictory because the adult worms live in the host for about three years26. This has a cumulative effect through new infections imposed on those already present. Ascaris adults have a much shorter lifespan of about one year26. The significantly higher prevalence of giardiasis in younger children may be the result of resistance developing with ongoing exposure26,27. In Cape Town, there is clearly a need for in-depth analysis and monitoring of sources of infection by intestinal pathogens because a large proportion of the city’s population lives under conditions similar to those at the study site, or at greater exposure to infection where there is overcrowding and promiscuous defaecation9. The national guidelines on recycling of sewage are intended to ensure utilisation of the sludge as an organic fertiliser and re-use of the water after purification because both components are valuable resources25. Since the use of products that will contain embryonated STH eggs is allowed, they could be a source of helminthic and protozoal infections if utilised for growing vegetables or fruit to be eaten raw. It is important to obtain comparative data by conducting parasitological surveys in affluent suburbs of Cape Town where the prevalence of intestinal helminths and protozoa is not known. The results will show whether regular treatment of the entire population of the city with effective anthelminthics is necessary, as well as general implementation of non-medical control measures that are affordable and sustainable. Mechanical transfer of eggs and cysts from human faeces or sewage to food and/or water could be happening on a significant scale. It is generally known that flies, cockroaches and rats are problems in the city. Flies are ubiquitous, especially in summer, and are likely to be vectors.32-35 Rats in Cape Town could be reservoir hosts of the dwarf tapeworm Hymenolepis nana and may host strains of Giardia that infect humans26. There are also many dogs in the city. They can be important disseminators of some STH eggs and protozoa but are probably not a significant risk in respect of zoonotic protozoal pathogens37 . Strong winds are a feature of the climate in the south-western Cape and may blow embryonated STH eggs about as a component of dust, as has been reported from Japan36 . Eggs transferred by wind could originate either from human faeces in places in the city where people defaecate on the ground because they cannot access functional toilets9, or from sewage products used as fertiliser. The detection of hookworm-like eggs and Enterobius eggs during this study are both of importance, for different reasons. The Mediterranean-type climate in the south-western Cape may be highly suitable environmentally for Ancylostoma duodenale if it were to be introduced by migrants or visitors from places where it is endemic. This threat needs to be monitored because hookworm can be a major cause of anaemia, especially in pregnant women1 , 3,4. Enterobius vermicularis (pinworm) is not a soiltransmitted helminth and is particularly important within families, especially af.uent ones26. This is partly because the light eggs are easily disseminated by air movement within the household. Familial stress because of irritability caused by sleep disturbance secondary to perianal pruritus is characteristic of enterobiasis26,28. In terms of the criteria agreed under WHA resolution 54.19, it can be concluded that non-selective, regular, synchronized deworming should be implemented in five of the nine schools in the study area. However, even when the prevalence of worm infestation is less than 50%, it can be recommended that regular deworming should probably be implemented, based on the possibility that HIV/AIDS and TB might use the dominant humoral immune response to helminthiasis opportunistically in terms of faster infection dynamics and disease progression. This kind of immune pro.le may also impair vaccination 2,3,8,12-23. There is strong serological evidence from the study site for this reasoning. New research has revealed that 15% of a random sample of children (n = 359) had Ascaris eggs in their faeces but 48% had elevated Ascaris-speci.c IgE in serum (C.C. Obihara, unpublished data). Elevated Ascaris-speci.c IgE indicates a competent immune response to either larval stages or adult worms. After destruction of the original parasites, it is likely to be boosted by a new challenge when Ascaris is endemic. Hence, Ascaris-speci.c IgE it is inevitably more frequent than eggs in faeces, and egg-positivity may indicate immunological incompetence in some individuals21,23. Regular, non-selective deworming could minimise humoral immune dominance and thereby reduce the threat of HIV/AIDS and TB. This kind of effect should be particularly important with regard to immunisation against HIV before sexual activity starts11,22,23. In poorer, more recently formed city communities and in rural areas, the need is greater because between 70% and >90% of school-age children in the south-western Cape have been found to be infected by worms5-9, and giardiasis is widespread 6,7,27. Potential vaccines that are intended to elicit a cellular immune response against HIV may be particularly vulnerable to reduction in ef.cacy when helminthiasis is highly endemic22,23, especially when used prepubertally11. Like helminths, intestinal protozoa can elicit a predominantly humoral immune response26. Control of worm infestation in southern Africa as advocated by the WHA1-4, should not be delayed pending assessment of the extent to which helminthiasis may interact with various coendemic diseases, or whether regular deworming may modulate the amount of allergy in communities38,39. Adjustments in policy and practice can be made when necessary, based on monitoring of results and new research findings. AcknowledgementsThe late Professor Albert D. Beyers of the Department of Medical Biochemistry, University of Stellenbosch, South Africa, made a fundamental contribution to the planning and initiation of this study. Anthelmintic tablets (mebendazole; Vermox®) were donated by Janssen-Cilag Pharmaceuticals. References
Copyright © 2005 - Makerere Medical School, Uganda |

{kind=link}