 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
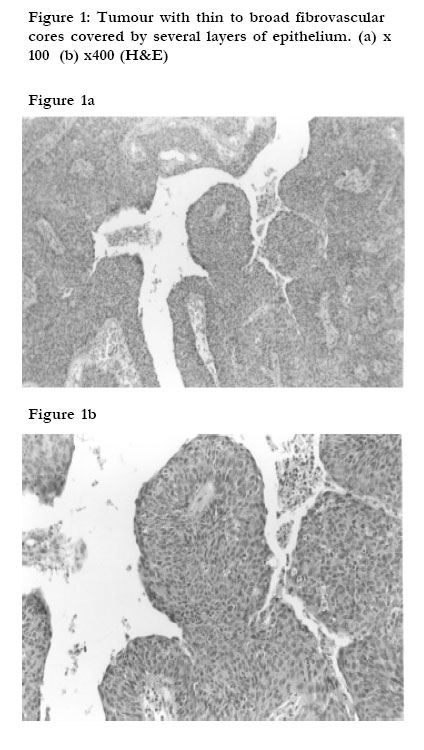
African Health Sciences, Vol. 5, No. 4, December 2005, pp. 291-294 Papillary squamous cell carcinoma of the cervix in Uganda: a report of 20 cases Michael Odida Department of Pathology, Faculty of Medicine,Makerere University Code Number: hs05050 Abstract Background: Non-glandular papillary carcinoma of the cervix are uncommon tumours. In Uganda where cervical carcinoma is very common, no cases of papillary squamous cell carcinoma of the cervix has been reported. Introduction Non-glandular papillary carcinoma of the cervix are uncommon tumours with rather sketchy literature 1-7. In Uganda where cervical carcinoma is very common 8, 9, no cases has been reported although a number of neoplastic cell types of squamous cell carcinoma were documented 10. Since an earlier report from Uganda indicated a large proportion of undifferentiated tumours of the cervix 8, it is worthy to find out if cases of papillary tumours could have been misdiagnosed as they are sometimes difficult to diagnose6. In this paper, 20 cases encountered in the Department of Pathology during a period of six years are presented. Methods Cases of cervical carcinoma diagnosed in the Department of Pathology, Makerere University from 1968 to 1973 were retrieved. During this period, the Department of Pathology provided free histopathology services for all hospitals and other health units in Uganda 11. For each case new sections were made and stained with Haematoxylin and eosin (H&E). All cases with poor or small inadequate histological sections were excluded. Each case was then examined by the author without reference to the original diagnosis. Cases with features of squamous differentiation 12 and forming papillary patterns were noted. Clinical information, including patients’ particulars were obtained from the histology request forms. Results Of the cervical carcinoma cases diagnosed in the Department during this period, histological materials were available for 656 cases. Sixty six cases were excluded, leaving 590 cases for review. Out of the 590 cases reviewed, 20 were papillary squamous cell carcinoma. Ages were indicated in 16 cases and ranged from 22 to 70 years (mean 46.3 years). The main presenting symptom was abnormal vaginal bleeding in most patients. Other symptoms were offensive vaginal discharge and abdominal pain. The duration of symptoms varied from one week to one year with an average of 20 weeks. Grossly, the tumuors were very friable and bled profusely. Microscopically, two variants were recognized: i) Tumours with thin to broad fibrovascular cores covered
by several layers of epithelium showing various degrees of
atypia (15 cases). The epithelial cells were basaloid and their
long axes were orientated perpendicular to the surface (figure
1a and 1b). In two cases, there were focal areas of
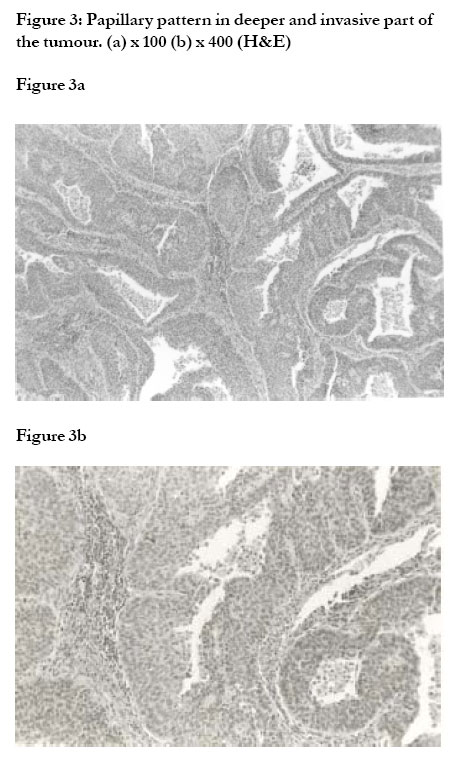
keratinisation. In the deeper and invasive parts of the tumour, the papillary pattern was still apparent (figure 3). Invasion of the stroma was associated with nonspecific chronic inflammatory infiltrate. No invasion of the fibrovascular core was noted in all 20 cases. Cytological changes suggestive of human papillomavirus (HPV) infection was not present in all 20 cases. Discussion There have been relatively few reports on non-glandular papillary carcinomas of the cervix, with no cases reported from Uganda where cervical cancer is very common 8,9. The present study is the first to document the occurrence and clinicopathological features of paipillary squamous cell carcinoma of the cervix in Uganda. Clinically most of the cases were older women (mean age 46.3) and a great proportion presented with abnormal vaginal bleeding, similar to cases reported by Randall et al6and Koenig et al7. The results of the present study suggests that papillary squamous cell carcinoma of the cervix is a distinct clinicopathological entity. This is supported by a previous detailed report of papillary squamous cell carcinoma of the cervix which was given by Randall et al6, who described nine cases. They suggested that papillary squamous cell carcinoma of the cervix should be considered a distinct clinicopathological entity, separate from verrucous carcinoma. This conclusion was supported by clinical behavior and microscopic appearance of the papillary lesions. Three of the patients had metastases, a phenomenon which usually does not occur with true verrucous carcinoma5. Besides, the papillae of papillary squamous cell carcinoma are lined by dysplastic cells, in contrast to verrucous carcinoma which are lined by cytologically benign epithelial cells. They noted that most of the early cases of malignant papillary lesions of the cervix were in fact verrucous carcinomas, with few cases of true papillary squamous cell carcinoma. The results of this study showed two variants of papillary squamous cell carcinoma of the cervix. One variant was composed of basaloid epithelial cells and the patients were all aged 40 years and above. The other variant was composed of intermediate cell types and all except one patient were aged less than 40 years old. Previous evidence supporting the views that papillary squamous cell carcinoma of the cervix as a distinct entity with variants came from Koenig et al7. They reviewed 32 cases and divided them into three groups, viz. predominantly squamous (nine cases), mixed squamous and transitional (16 cases) and predominantly transitional (seven cases). All cases demonstrated a papillary architecture with fibrovascular cores lined by multilayered, atypical epithelium resembling high grade squamous intraepithelial neoplasia of the cervix. In 20 cases with adequate histological materials, stromal invasion occurred in 18. They concluded that papillary squamous cell carcinoma of the cervix is a distinct clinicopathological entity and display a morphologic spectrum. An interesting observation is that the tumour cells of papillary squamuos cell carcinoma are similar to cells in some conventional non-papillary squamous cell carcinoma of cervix 10, 12. A possible explanation could be that the tumour cells in papillary carcinomas produce some factors which induces papillary desmoplasmic reaction. The findings of Randall et al6, that some of their cases showed papillary structures only in the superficial parts of the tumours suggest that some of these factors may sometimes be operating only in the tumour surfaces. Papillary carcinomas exhibit peculiar morphologic variants in differentiation. In the present series, the tumour cells showed features of squamous differentiation. Some of the cases were composed of basaloid like cells while others were of intermediate cell type. The findings of the present study lent further support that these papillary tumours of the cervix are actually variants of squamous cell carcinomas. All the cases reported by Randall et al.6, had squamous differentiation. Cases with transitional morphology have also been reported by Koenig et al.7 and Ng 18. Although some of the cases of Koenig et al. 7 showed features of transitional epithelium, application of immunohistochemical staining showed the vast majority of these tumours displayed the cytokeratin profile of squamous cell carcinoma of cervix. These findings support the hypothesis that squamous cell carcinoma of the cervix are heterogenous group of tumours like the non Hodgkin’s lymphomas10. Papillary squamous cell carcinoma of the cervix may be difficult to diagnose. None of the cases reported in these series had been diagnosed as papillary squamous cell carcinoma. This difficulty had been reported by Randall et al 6. In addition, it was observed that invasion may be difficult to demonstrate histologically unless deep biopsies are obtained. A high index of suspicion on the part of the clinician and an awareness of papillary squamous cell carcinoma by the pathologist are required to make an accurate diagnosis. Presently there is no precise definition of papillary squamous carcinomas. Ng 18 suggested that papillary tumours should be diagnosed only if papillary or anastomosing frond-like architectural pattern was seen in >70% of the tumour tissue. Although the suggestion is good, it would be better it was based on many cases with well defined criteria. Data on the behavior of papillary squamous carcinoma of the cervix are few. In the present series, no follow-up data were available because of lack of a system for tracing patients 11. Two studies from U.S.A 6,7 showed that these tumours probably have the propensity of late recurrences and possibly late metastases. In the cases reviewed by Koenig et al. 7, of the three patients who presented with advanced disease, the one who received chemotherapy survived for 33 months, compared to three and four months respectively for the other two patients. They thought that there may be a role for chemotherapy in treating these tumours. The role of human papillomavirus (HPV) in squamous cell carcinoma of the cervix have come from many studies 13-17. Whether papillary squamous carcinoma of the cervix is associated with HPV is not clear. In the present series, none of the cases had features of HPV infection. Randall et al 6 found no cytologic changes associated with viral replication that is koilocytosis. Koenig et al 7 found changes suggestive of HPV infection in six cases. In summary, the results of this study show that in Uganda, papillary squamous cell carcinoma of the cervix does occur with morphologic variants. It is suggested that additional studies to further characterize the clinicopathologic features of these tumours and their response to different therapeutic agents be carried out. Acknowledgement I thank Dr. Rolf Schmauz of the Institute of Pathology, Papenburg, Germany for his constructive criticism and providing facilities for the study. I would also like to acknowledge the use of facilities provided by Sida/SAREC under the Makerere University-Karolinska Institute Research Collaboration when this paper was being prepared. References
Copyright 2005 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs05050f1.jpg] [hs05050f3.jpg] [hs05050f2b.jpg] [hs05050f2a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}