 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
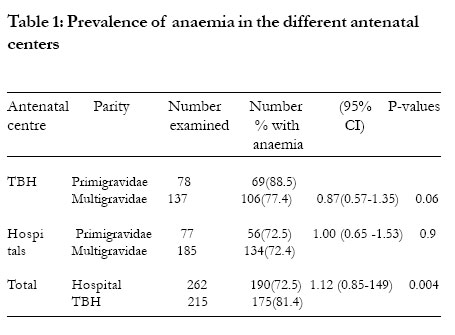
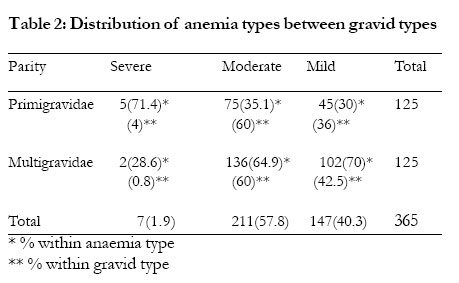
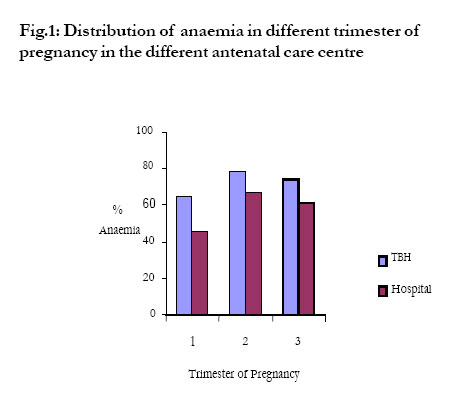
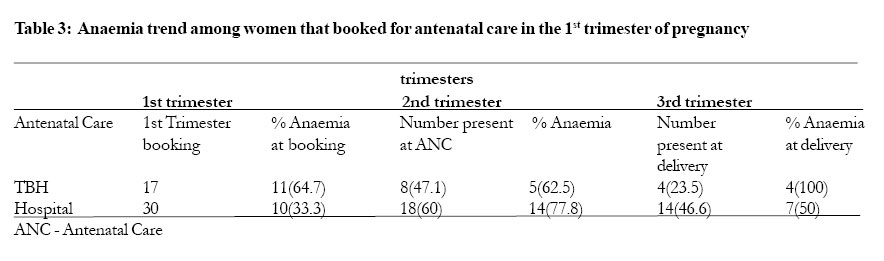
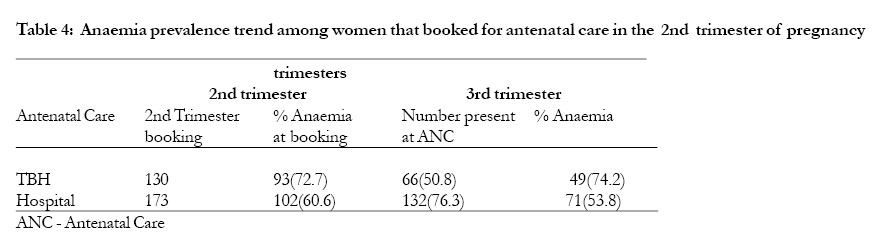
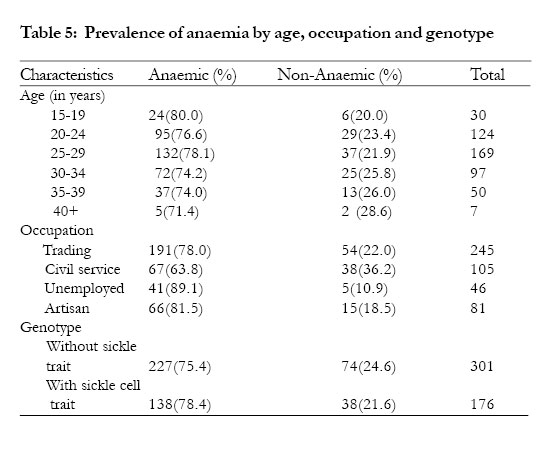
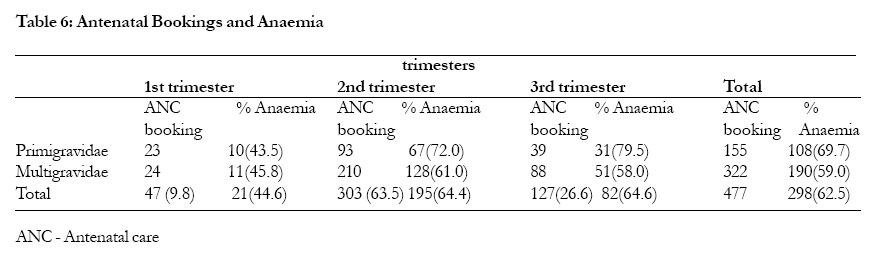
African Health Sciences, Vol. 5, No. 4, December 2005, pp. 295-299 Anaemia in pregnancy: a survey of pregnant women in Abeokuta, Nigeria Idowu O.A1., Mafiana C.F1., and Sotiloye Dapo2 1 - Department of Biological Sciences, University of Agriculture, Abeokuta, Nigeria Code Number: hs05051 Abstract Background: Anaemia in pregnancy is a common problem in most developing countries and a major cause of morbidity and mortality especially in malaria endemic areas. In pregnancy, anaemia has a significant impact on the health of the foetus as well as that of the mother. 20% of maternal deaths in Africa have been attributed to anaemia Keywords: Pregnant women, anaemia, antenatal care, multigravidae, primigravidae Introduction Anaemia in pregnancy is an important public health problem worldwide. WHO estimates that more than half of pregnant women in the World have a haemoglobin level indicative of anaemia (< 11.0gldl), the prevalence may however be as high as 56 or 61% in developing countries 14. Women often become anaemic during pregnancy because the demand for iron and other vitamins is increased due to physiological burden of pregnancy. The inability to meet the required level for these substances either as a result of dietary deficiencies or infection give rise to anaemia 13. Anaemia ranges from mild, moderate to severe and the WHO pegs the haemoglobin level for each of these types of anaemia in pregnancy at 10.0 – 10.9g/d1 (mild anaemia) 7 – 9.9g/dl (moderate anemia) and < 7g/ dl (severe anaemia) 15. Prevalence of anaemia can be as high as 61% in developing countries 14 with a high incidence and severity occurring among primigravidae living in malaria endemic areas8. Studies in Nigeria have shown that malaria is still a major problem among pregnant women 6,8. In pregnancy, anaemia has a significant impact on the health of the foetus as well as that of the mother. 20% of maternal deaths in Africa have been attributed to anaemia 4. Foetuses are at risk of preterm deliveries, low birth weights, morbidity and perinatal mortality due to the impairment of oxygen delivery to placenta and foetus 1,2,4. The management and control of anaemia in pregnancy is enhanced by the availability of local prevalence statistics, which is however not adequately provided in Nigeria. Therefore, this study aims at providing prevalence statistics of anaemia in pregnancy and to assess the effectiveness of antenatal care in preventing anaemia among pregnant women in Abeokuta Nigeria. Methods Study area/Centres The study was conducted in Abeokuta, Ogun State, Nigeria in three centers namely: Federal Medical Centre Idi-Aba, Ogun State General Hospital Ijaye and Araromi Traditional Birth Home Iberekodo; all in Abeokuta. Ethical clearance and consent Sample collection All quatitative data was entered in computer and analysed using SPSS version 10.1 for windows. Descriptive statistics were computed for all relevant data. Association between anaemia and pregnancy was tested using chi-square. All significance are reported at P<0.05. Women that were anaemic at one trimester or the other during pregnancy Results Four hundred and seventy-seven (477) women were enrolled in the study, 262 from the Federal Medical Centre and Ogun State General hospital (77 were primigravidae and 185 were multigravidae). Two hundred fifteen pregnant women were also enrolled from Araromi Traditional Birth Home (TBH); (78 primigravidae and 137 multigravidae). A total of 155 primigravidae and 322 multigravidae were enrolled. Anaemia was recorded in 365 (76.5%) of the enrolled women at one trimester of pregnancy or the other; Of these 125 were primgravidae and 240 multigravidae, constituting a prevalence of 80.6% and 74.5% anaemia among primigravidae and multigravidae respectively. Percentage anaemia was higher among women in the TBH (81.4%) than those in the hospitals (72.5% Table 1). Severe anaemia was recorded in 7(1.9%) women, 5(71.4%) of whom were primigravidae. Moderate anaemia was predominant as shown in Table 2. In the different trimesters of pregnancy, women in the TBH were observed to exhibit, a higher prevalence of anaemia than those receiving antenatal care in the hospitals. However, percentage anaemia was highest in the second and lowest in the first trimesters of pregnancy in the different antenatal centers (P>0.05) as shown in Figure. Tables 3 and 4 show the trend of anaemia among women that booked for antenatal care in different trimesters of pregnancy in the different antenatal centers. In the hospital, 10 women were anaemic at 1st trimester booking; only 5 of them were seen at delivery with 3(60%) still being anaemic, however, of the 102 anaemic cases recorded at 2nd trimester booking, 84 were seen at delivery with anaemia still recorded in 67(79.8%). At the TBH, 4 of the anaemic women that booked in the 1st trimester were seen at delivery and all were still anaemic. Among the 2nd trimester booking, anaemia was still recorded in 40(81.6%) of the 49 women seen at delivery. Women in the 15 – 19 years age group constituted the highest percentage of anaemic cases (80%) followed by 25 –29 years age group (78.1%) compared to the other age groups, Table 5. All cases of severe anaemia were recorded in women less than 30 years of age. Anaemia were found to be more prevalent (78.4%) among carriers of sickle cell traits than those without such traits (75.4%) this difference is however not statistically significant, Table 5. Unemployed women were more anaemic (89%) while those in civil service were least anaemic. Antenatal care (ANC) bookings and anaemia A higher percentage of women registered for antenatal care in the 2nd trimester of pregnancy 303 (63.5%) as against 47(9.9%) and 127 (26.6%) registrations in the 1st and 3rd trimesters respectively. At ANC booking, 298 (62.5%) were already anaemic. 44.6% prevalence was recorded among those that registered in the 1st trimester, 64.4% and 64.6% in the 2nd and 3rd trimesters respectively P< 0.05. Anaemia at booking being highest among those that booked in the 3rd trimester, however prevalence of anaemia was generally higher among primigravidae (69.7%) than multigravidae (59.0%) P< 0.05 except in the 1st trimester as shown in Table 6. Of the 7 cases of severe anaemia recorded in this study, 4 (all primigravidae) were already severely anaemic at ANC booking, 3 of which booked in the 3rd trimester and 1 in the 2nd trimester of pregnancy. There was no record of severe anaemia at ANC booking among multigravidae. Generally there was a high level of absenteeism at the antenatal centers with women failing to keep ANC appointments especially at the TBH (Tables 3&4). Absence of symptoms of ill health and financial constrains were the major reasons given by these women for late booking and inconsistency in keeping ANC appointments. Discussion The prevalence of anaemia recorded in this study (76.5%) is an indication that anaemia during pregnancy is a major problem in Nigeria especially among primigravidae. The prevalence and severity of anaemia recorded in this study differs from that recorded by Ogbeide11. This variance may be attributable to the inclusion of women patronising the traditional birth home in this study who were found to have a higher prevalence of anaemia compared to those attending the hospital for antenatal care (Table 1). The reason for the difference recorded in prevalence between the hospital enrolled and TBH enrolled women may be connected to the care given to the women in these centres which in the hospital included the use of folate and routine haematological examination to determine blood level and the immediate medical management of anaemic cases. This however differs from the care given at the TBH, which was mainly in the consumption of herbal preparation made from tree barks, leaves and roots of undisclosed plants. The iron supplementation necessary to prevent deterioration of anaemic condition during increased physiological burden of pregnancy 7 is lacking among women in the TBH, this may have contributed to the higher prevalence recorded in this center.This study confirms that severe anaemia is more common among primigravidae compared to multigravidae as also recorded by Nagaraj, (2003). This is because malaria, a major cause of anaemia in pregnancy in endemic areas 3 is known to be more severe among primigravidae 9. This is an indication that primigravidae are more at risk of maternal death as a result of severe anaemia. The peak of anaemia recorded in this study (2nd trimester) coincides with the period when haemodilution is at its peak. This may have contributed to the high prevalence recorded in the 2nd trimester, indicating that anaemia is further aggravated by haemodilution. However, this result is at variance with the report of WHO 16 in which anaemia is said to be significantly higher in the 3rd trimester of pregnancy than the first two trimesters. The prevalence of anaemia at delivery in both centers (Tables 3 & 4) show that there is no significant impact of the antenatal care on the anaemia status among the pregnant women especially those at the TBH; this may be attributable to the low level of compliance to the use of prescribed medications especially among women in the hospital. This is an indication that these women do not necessarily overcome anaemia but only slip from one type of anaemia to another either as a result of haemodilution, infection, and dietary deficiencies or as a result of appropriate medical management of anaemic cases. A higher prevalence (81.5%) of anaemia recorded among teenage mothers (15-19 years) conforms to the observation of 11,12. Antenatal booking were found to be late among these pregnant women as only 9.9% booked for ANC in the 1st trimester of pregnancy, this may have contributed to the high prevalence of anaemia recorded in this study since early antenatal care results in better monitoring and early detection of anaemia and its correction by appropriate supplementation 10. This may have also contributed to the high percentage of anaemia recorded at the time of antenatal booking. The high level of anaemia recorded in this study among unemployed pregnant women may indicate that poverty borne out of unemployment may have contributed significantly to the high level of anaemia as the women cannot afford to book early for antenatal care, eat nourishing food and prevent possible infection. However, the patronage of TBH is not necessarily due to poverty but to cultural beliefs, which are being inculcated into these women by their mothers, and mothers-in-law who also patronized TBH for antenatal care in their own time. Conclusion This study has shown that anaemia in pregnancy is still a major health problem in Nigeria identifying primigravidae as being more at risk than multigravidae. So also are women using TBH for antenatal care, pregnant teenagers and women that book late for antenatal care. The use of TBHs being a common practice in Nigeria indicates that the traditional health providers need to be enlightened on the need to include the use of iron and folate supplements in the management of their pregnant patients. Educating women on early ANC booking and compliance with the use of prescribed medications should also be emphasized. Acknowledgment We sincerely appreciate the management and staff of the Federal Medical Centre(FMC), Ogun state General hospital and Chief Araromi for their support in the course of this study. References
Copyright 2005 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs05051t6.jpg] [hs05051t2.jpg] [hs05051t1.jpg] [hs05051f1.jpg] [hs05051t3.jpg] [hs05051t5.jpg] [hs05051t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}