 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
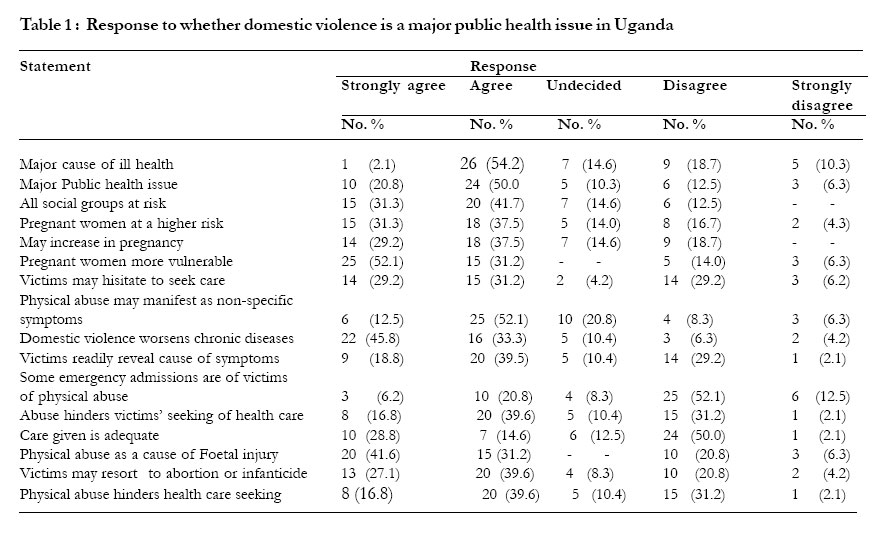
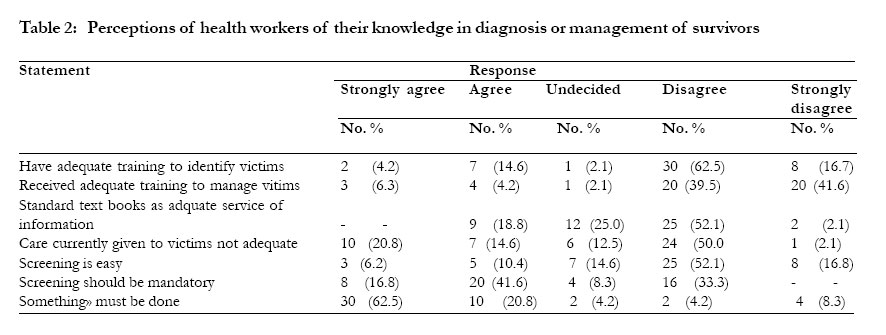
African Health Sciences, Vol. 5, No. 4, December 2005, pp. 315-318 Perceptions of health care providers in Mulago hospital on prevention and management of domestic violence Dan K. Kaye,1 Florence Mirembe1, Grace Bantebya. 2 1Dept. of Obstetrics and Gynaecology, Makerere University Medical School, P. O. Box 7072, Kampala, Uganda. 2Department of Women and Gender Studies, Makerere University, P.O .Box 7062, Kampala, Uganda. Code Number: hs05055 Abstract Objective: To explore knowledge, attitudes and practices of health workers in Mulago hospital towards domestic violence prevention and management, especially violence during pregnancy. Introduction The American College of Obstetricians and Gynaecologists defines domestic violence as ‘any act that is intended, or perceived to be intended, to cause physical, or psychological harm by people related through blood, intimacy or law’.1 Women are more likely to suffer violence from family members or intimate partners than from strangers.2 Domestic violence forms a pattern of behavior and control which takes a variety of forms. These include physical assault, psychological abuse (threats, intimidation, degrading humiliating behavior), sexual coercion and controlling behavior (isolation from family or friends and restriction of freedom of movement or control over resources).1,2 Domestic violence affects women’s ability to engage in safe sexual relations free from coercion or disease, make choices regarding pregnancy or fertility regulation, go through pregnancy safely or seek appropriate healthcare for self or family.4. There were many reports of domestic violence in local newspapers in Uganda (such as The New Vision and The Monitor Newspapers) and radio stations frequently air programmes on domestic violence. Despite this, many cases are unreported or undiagnosed 1-4 which leads to perpetuation of the cycle of violence. Sexual abuse increases risk of acquisition of sexually transmitted infections, unwanted pregnancy and unsafe abortion.4 A cross-sectional study on domestic violence in women attending antenatal clinic in Mulago hospital on their firs visit found a prevalence of 57.1%.5 Little was known about perceptions of health workers in Mulago hospital regarding management or prevention of domestic violence, especially during pregnancy. The objective was to explore knowledge, attitudes and practices of health workers in Mulago hospital towards domestic violence. Methods From 5th to 25th March 2000, a purposive sample of 48 health workers were identified the Obstetrics and Gynaecology department. Respondents consisted of 16 doctors, 15 midwives, 10 nurse-midwives and 7 undergraduate medical students, selected to represent views of all cadres of staff. A self-administered questionnaire was given to each to determine their perceptions of management of domestic violence. This questionnaire consisted of 22 statements on knowledge about domestic violence in pregnancy as well as attitudes and practices regarding screening for domestic violence and management of survivors. Respondents were requested to respond on a 5-point Likert scale whether they agreed, disagreed or were undecided about the statements. Analysis was made in terms of frequencies and percentages. To obtain indepth information about the reasons behind perceptions, in-depth interviews were conducted with 12 purposefully-selected staff of the department, who did not participate in answering the questionnaire. They included 3 post-graduate medical students (2 female, 1 male), 2 gynaecologists, 5 nurse-midwives of varying ranks (2 enrolled, 2 registered, 1 health visitor) and 2 undergraduate students. The area of discussion was domestic violence and linkage to reproductive ill-health, attitudes to screening for domestic violence in pregnancy, practices (survivor management) and availability of information on domestic violence. Thematic content analysis, through systematic comparison of emerging codes and categories (meaning units) across data texts, using the Easy Text (EZ) software for data retrieval was used as described by Creswell.6 Results Respondents had inadequate knowledge of domestic violence: its consequences, management or prevention (Table 1 and 2). Many health workers neither knew how to, nor did routinely screen for domestic violence. Few believed that victims might hesitate to seek care, 43.6% did not perceive domestic violence as a major cause of ill health, while more than 24% did not perceive it as a major public health issue. Many respondents neither knew that domestic violence is common in pregnancy, nor associated it with reproductive ill-health. In the study whereas 58.4% approved routine screening, only 16.6% perceived this is easy, though 83.3% thought something must be done urgently. In the in-depth interviews, all participants reported having seen cases of domestic violence during pregnancy, mainly those with physical injuries, admitted to antenatal wards. Nine respondents were uncertain about what care had been provided, and did not know what optimum care the patients should receive. Ten respondents had the view that “survivors are the ones to blame”. The common view was that domestic violence was a common practice, and some referred to it as normal. Probed as to when they considered it abnormal, the common view was that violence ceased to be normal if physical injuries resulted, as exemplified by one respondent, a 23 year-old housewife: “It is normal to discipline the wives, but the disciplining should not be excessive as to result in injuries.” Respondents for in-depth interview were uncertain whether domestic violence increases in frequency during pregnancy, but agreed that injuries are more severe and likely to cause more damage. Whereas all agreed that counseling skills are necessary in healthcare, none had ever received skills on counseling and none had ever referred patients/survivors for such counseling. However, all agreed that survivors require counseling. On sources of information on domestic violence, newspapers were cited as their main source. None had ever-received information on domestic violence during their pre-service or in-service training. All were of the view that domestic violence does not appear in their standard text-books, which made it difficult for them to update themselves with such information. Some respondents had come across newsletters with information on domestic violence, but could not recall the contents. From in-depth interviews, none of the respondents offered survivors counseling, referral to social workers or linkage to the judicial services. Underlying reasons for knowledge, attitudes and practices were cultural stereotypes, lack of training and inadequate knowledge. Personal negative attitudes, lack of technical competence, cultural stereotypes or institutional constraints act as barriers which limit ability or willingness to assist survivors. Discussion The findings indicate that health workers had limited knowledge on domestic violence, and didn’t know that it was a problem of great public health importance. Gazmararian et al,7 in a review of 13 studies found a prevalence of domestic violence in pregnancy of 1 to 11%. Therefore, domestic violence is commoner than many obstetric complications such as pre-eclampsia or diabetes mellitus. Several respondents could not relate patients’ symptoms to violence. Most health workers didn’t know how to screen for, identify, diagnose or manage survivors. In the study only 18.6% of respondents felt they had adequate knowledge to identify victims; while only 10.5% felt they had received adequate pre-service or in-service training. This knowledge deficit is compounded by scarcity of information of domestic violence in standard textbooks. As a result, few respondents felt that care given to survivors was adequate. Most health workers had some knowledge on the consequences of physical assault in pregnancy. This is probably due to the fact that domestic violence may result in physical trauma, which appears in standard medical textbooks. Physical abuse may lead to ruptured uterus, abortions, fetal death, premature membrane rupture, preterm labour, abruptio placenta, low birth weight or maternal death.7 Such lesions may result from direct trauma to the abdomen.3,4,7 Typical injuries occur on the face, head, neck, breasts and abdomen, rather than the periphery of the body.1-3,7 The type of lesion depends on the severity of injury, the frequency of injuries, use of and type of weapon used and any concurrent destructive behavior.1-4,7 The health care system is the only institution that interacts with almost every woman at some point in her lifecycle. This provides healthcare providers, who come into contact with survivors, with a unique opportunity to identify and help them.1,2 In an American study, 88% of women battered during pregnancy had history of battering prior to conception.8 Domestic violence tends to increase both in severity and frequency in pregnancy.9 A qualitative study from Zimbabwe found that violence ongoing before pregnancy increases in pregnancy.10 But even those who seek healthcare don’t get optimal benefit. Guilt, shame, anxiety, fear of more abuse and restriction of movement may be reasons why survivors may not seek care or fail to reveal their symptoms.2 Regarding practices, health workers did not know what is expected of them. A review of patients’ views in the United Kingdom gives an insight of what their expectations are11: “Patients want a doctor who listens, who sorts out their problems, who provides personally delivered care that addresses their problems….whom they trust and who has skills to assist them in making strategic life decisions; …who advocates for them and coordinates care given by other team members. They also want to see this same doctor at every opportunity”. It is possible that survivors who seek healthcare but don’t report all their problems are only waiting for health workers to broach the subject, and get disillusioned if no such help is forthcoming. Motsei12 summarized barriers to identifying and helping survivors as: 1). Patient factors (reluctance to reveal cause of their injuries or symptoms, or imagining health professionals will not help) 2). Health professional barriers (lack of awareness or means to identify the problem, believing that violence is not a health issue or is culturally acceptable; blaming the woman or not knowing how to intervene). 3). Institutional barriers (lack of an institutional framework with clinic services, counseling staff or management protocols). One well-recognized barrier to provision of optimum care to survivors is that health workers themselves lack knowledge and skills. This is partly due to inadequate training or lack of such information in standard medical textbooks. The lack of information on domestic violence is universal. Parsons and Moore13 reviewed 48 obstetrics and nursing text books published between 1990 and 1996. Using a 12-point score of information related to domestic violence, they found that only 37% of physicians’ texts and 63% nursing text had any content on domestic violence. How can health workers improve quality of care for survivors? Patients present to health workers on many occasions without health workers making the right diagnosis of the cause of injuries. This leaves patients frustrated as they do not get the desired help. In medical practice skills, knowledge and attitudes/ perceptions are all important elements of clinical expertise. McFarlane et al14 found that routine asking of 3 assessment questions in a private setting identified one in 6 women who had history of abuse in pregnancy. This formed the basis of the Abuse Assessment Screen, (a tool that has been found to be valid and reliable), and increased prevalence of abuse from a self-reported rate of 8% to over 29% in the same population. Norton et al15 found that the Abuse Assessment Screen had higher detection rates than when the same questions are incorporated into standard interview. Unfortunately, patients don’t readily reveal presence of the problem. The cause of this could be that survivors think health workers can identify the problem, will ask/ enquire about the problem or would disregard information about violence. Some health workers often blame survivors, so the survivors cannot easily trust them. Conclusions Health workers lack knowledge, have negative attitudes and provide sub-optimal care to domestic violence survivors. This is evidenced by limited knowledge and failure to identify the problem despite often glaring injuries. The reasons for this are: they don’t know how to, are unconcerned, fear to get involved, don’t have the time, don’t have the optimum environment (privacy, confidentiality or management protocols) or think survivors are to blame. Recommendations
Acknowledgment The author is grateful to SIDA/SAREC, who provided the grant to the Department of Women and Gender Studies of Makerere University, from which this research was funded under the First University-wide Gender Mainstreaming Research. Special thanks to Prof. Florence Mirembe and Prof Grace Bantebya (Department of Women and Gender Studies) for supervising this research, and to all staff of the Obstetrics and Gynaecology Department, Makerere University who participated in the research. References
Copyright 2005 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs05055t1.jpg] [hs05055t2.jpg] |
| |||||||||

{kind=link}
{kind=link}