 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 5, No. 4, December 2005, pp. 319-321 Competence of maternal and child health clinic workers in detecting malnutrition in Somalia Mohamed Gedi Qayad Faculty of Medicine, Somali National University, Community Medicine Department Code Number: hs05056 Abstract Background: The MCH clinic workers in Somalia receive formal and in-service
training to perform their professional duties. Their competence in the field
was never examined. This study assessed their competencies in detecting malnourished
children 5 years and
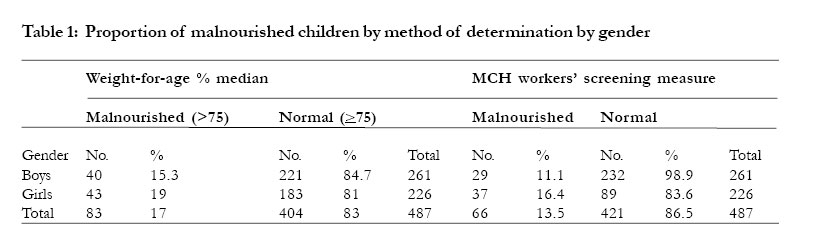
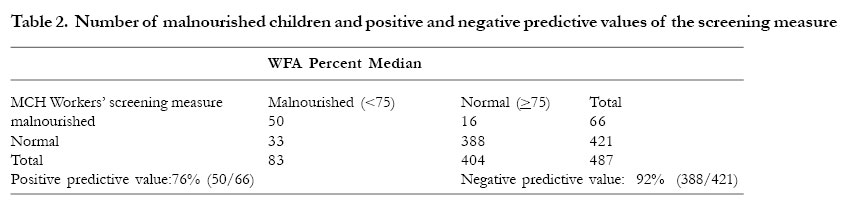
below in Beledweyne. Key words: Health workers, competence, training Introduction The Ministry of health (MOH) in Somalia, which is the primary health care service delivery institution in the nation, trains mid-level health care workers, nurses and other paramedics to provide primary and auxiliary health care services to the Somali population. In Somalia, as in many developing countries, these health workers are the sole health care providers for the majority of the population 1. Persons who have completed eight years of education are recruited for two-year training in basic nursing. In 1989, the level of prior education required for such training was raised to 12 years. The trainees are exposed to standard learning experiences, theory and practice, that provide the knowledge and skills needed to address major health problems facing the population. The training takes place in nursing schools and various health care facilities where people seek medical care. Experienced health care providers in these setting, physicians, nurses and auxiliary health workers, provide needed guidance and supervision to these trainees. After completion of their training, the MOH sends them to Maternal and Child Health (MCH) clinics and other health care facilities around the country. Some graduates, after one or more years in the field, receive further training in post-basic nursing and assume managerial positions in the MOH. The Primary health care (PHC) programs in various regions of the nation provide additional need-based training to the PHC workers, including nurses placed at MCH clinics, regularly. In Beledweyne, the capital of Hiran region, the MCH clinic provides health care services to the MCH population in the city and its’ surrounding villages. The PHC program in the region, which oversees the MCH clinic operations, provides in-service training to the MCH clinic workers on how to use the growth chart for monitoring growth and detecting malnourished children, a problem often encountered by these workers 2. Some studies showed competency deficiencies of health workers and mothers in using the growth chart 3, 4. However, the competency of MCH workers in Somalia, in this respect, was not examined. By virtue of their responsibilities as frontline health care providers and as the sole providers for the majority of the population in the country, it is essential to assess their competencies in the critical domains covered by the training. This paper examines the competence of these health workers in detecting malnourished children at the MCH clinic in Beledweyne. Methods The study was conducted in 1989 in Hiran region, Somalia. We obtained the data from the MCH clinic register in Beledweyne, which collects information on children five years and below attending the clinic. We used two months data, January and February 1989, for this study. These two months had complete data at the initiation of the study. The MCH workers recorded age, gender, weight and height measurements, illness and treatment, and nutritional status, based on the growth chart readings, of each child. They determined the nutritional status by plotting the child’s current weight, taken at the time of the visit, on the growth chart, designed by Gomez 5. Based on the weight plotted on the chart, this was recorded as normal, first, second, or third degree malnutrition in the MCH clinic Register. There were no prior weights in the chart for the child. The Centers for Disease Control and prevention (CDC) anthropometric software package (CASP) was used to calculate the weight-for-age (WFA) anthropometric index 6. In this paper, we compared the WFA percent median index to the nutritional status determined and recorded by the health workers to evaluate the competencies of the MCH clinic workers in detecting malnourished children. There were 487 children, 261 boys and 226 girls, in the study. We grouped the nutritional categories determined by MCH clinic workers into two categories. Children with first degree malnutrition and normal were categorized as normal and those with second and third degree malnutrition as malnourished. The former corresponds to >75 percent median WFA of the National Center for Health Statistics (NCHS) reference population, and the later corresponds to <75 percent median WFA 7. Similarly, we categorized the WFA percent median index into two categories. Children >75 percent median WFA were categorized as normal and those < 75 percent median WFA as malnourished. We refer the WFA index as the gold standard and the nutritional status determined by the health workers as the screening measure in the rest of the paper. We calculated the positive and negative predictive values of the screening measure to assess the competencies of the health workers in the MCH clinic. Positive predictive value was defined as the proportion of children who were truly malnourished among those classified as malnourished by the screening measure. This measure reflects the proportion of children falsely classified as malnourished, when they were truly normal. Negative predictive value was defined as the proportion of children who were truly normal among those classified as normal by the screening measure. This measure reflects the proportion of children falsely classified as normal, when they were truly malnourished. We used Statistical Packages for Social Sciences (SPSS) Software to construct 2 by 2 tables 8. We cross-tabulated the WFA index, the gold standard, with the screening measure to calculate the positive and negative predictive values of the screening measure. Results Table 1 shows the number and percent of malnourished children by gender and method of determination of the nutritional status. Seventeen percent of the children were malnourished based on the gold standard, whereas 13.5% were malnourished in the screening measure. Girls had higher prevalence of malnutrition than boys for both measures. The health workers underestimated the prevalence of malnutrition by 21%. Table 2 shows the number of malnourished children detected by the screening measure and its predictive values. The positive and negative predictive values were 76% and 92% respectively. Around 24% of the children classified by the MCH workers as malnourished were truly normal, and 8% of the children classified as normal were truly malnourished. The number of malnourished children misclassified as normal were higher than the number of normal children misclassified as malnourished, 33 and 16 respectively. DiscussionThe MCH clinic workers evaluated in the study showed some deficiencies in their competences to detect malnutrition. They wrongly classified around ten percent (10%) of the children studied. The misclassification was worse among malnourished children classified as malnourished compared to those classified as normal. Twenty four percent (24%) of the children classified as malnourished were normal and eight percent (8%) of the children classified as normal were truly malnourished. The former misclassification, often termed as false positives, may result in misuse of resources whereas the latter may expose undetected malnourished children to the adverse health consequences of malnutrition. Although the proportion of undetected malnourished children may not be alarming to health authorities in the developing world, countries like Somalia where the prevalence of malnutrition is high, children falling into this category could be substantial 9. The prevalence of malnutrition among the children, 5 years and below, attending the clinic would be underestimated by 21% (13.5/17), if one uses the MCH clinic register data for estimation purpose. This also portrays a wrong impression about the performance of nutritional intervention activities of the PHC program in Beledweyne, and may mislead planning decisions about future nutritional programs and allocation of resources. The competency deficiency observed in the study may herald other problems in their skills that are critical to the MCH population services, and may also reflect the competencies of similar cadre of health workers in other parts of the nation. The regional PHC programs assess the skills of these health workers before retraining them. However, post-training evaluations in the field are conducted rarely (verbal communication). Continuous monitoring and evaluation, which is included in the PHC framework, could remedy this problem timely. However, other priorities that often take precedence in the developing countries impede such proper actions. The problem observed in the study was caused by incorrect plotting of the weights on the growth chart, because other factors used in determining the nutritional status, i.e., age and weight, are constant and affect both measures, the gold standard and the screening measure, equally. A study in Lesotho showed that health workers had poor knowledge and skills in using the growth chart 3. Another study in Somalia, which examined mothers’ understanding of the growth chart, showed some deficiency 4. A study in south India showed the lack of benefits of the growth chart over other education methods 10. This indicates the complexity of using a simple health care technology for educational and screening purposes by trained health workers and mothers, and may require proper training programs to ensure the acquisition of critical knowledge and skills in using the growth chart and other health care technologies in the developing countries. There are several limitations in the study. The nutritional status categories determined by the MCH clinic workers were collapsed into two categories, normal and malnourished, to approximate the NCHS WFA index, which may misclassify some children. The positive and negative predictive values used to measure the competences of the MCH clinic workers are chosen arbitrarily, and other measures may be more appropriate to gauge their knowledge and skills in this domain. The MCH clinic workers may have used other additional information, e.g. signs of malnutrition, to determine the nutritional status. Despite these limitations and the lack of applicability of the findings to Somalia, currently, studies of this kind are appropriate, efficient and convenient for Somalia and other developing countries, where resource constraints hinder the execution of more expensive evaluation activities. Further investigation on the contents and methods of delivering the learning experiences may illuminate areas contributing to the competence weakness of the health workers evaluated in the study and others with similar training. Acknowledgment I am grateful to the Regional Medical Officer and Primary Health Care Coordinator in Hiran region for their assistance in facilitating the collection of the data. I also grateful to Dr. Jim Buehler, Professor at Emory University, Atlanta, Georgia, for reviewing and editing the article References
Copyright 2005 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs05056t2.jpg] [hs05056t1.jpg] |
| |||||||||

{kind=link}
{kind=link}