 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
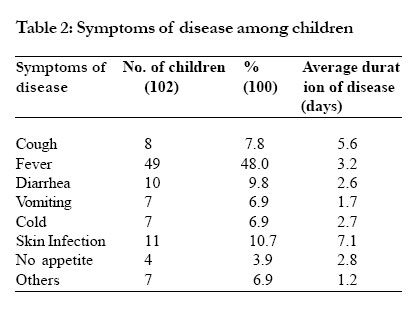
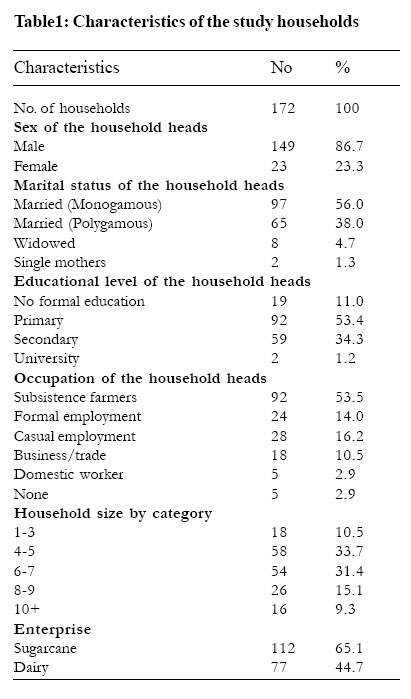
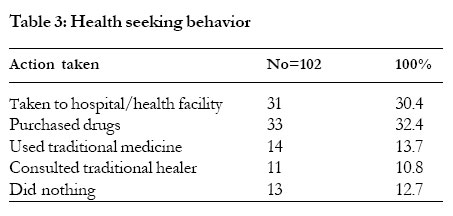
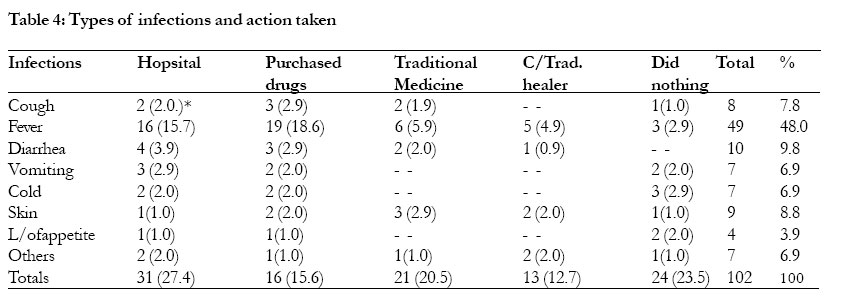
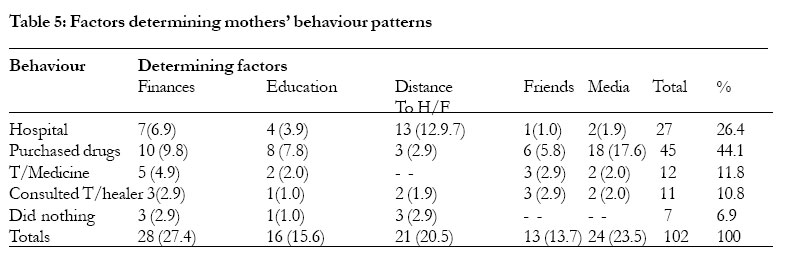
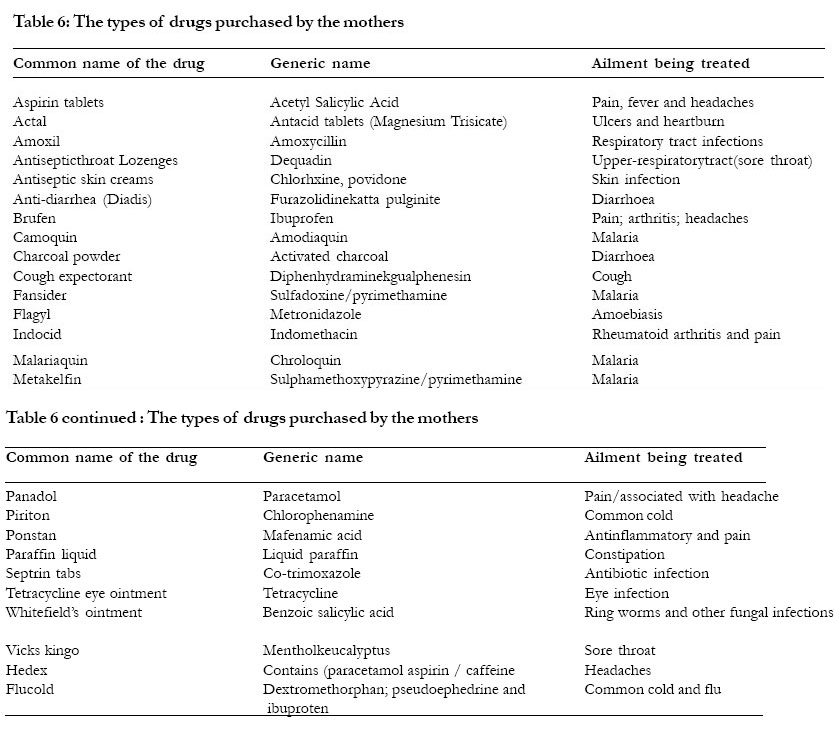
African Health Sciences, Vol. 5, No. 4, December 2005, pp. 322-327 Mother’s health seeking behaviour during child illness in a rural western Kenya community Grace M. Mbagaya,1* Mark O. Odhiambo,2 Ruth K. Oniang’o3 1 Moi University, Department of Home Science and Technology, P.O.Box, 1125 (30100), Eldoret, Kenya. Code Number: hs05057 Abstract Background: In most developing countries, the health of the children is strongly dependant on maternal healthcare behaviour. The study describes the prevalence of illness among preschool children in a rural sugarcane growing community and the mother’s health seeking behavior. Introduction Diseases among young children are the major causes of morbidity and mortality particularly in the developing countries of the world1. Each year about 13 million infants and children die in developing countries2 3. The majority of these deaths are due to infections, parasitic diseases, and many if not most of the children die malnourished. Malnourished individuals become debilitated and are susceptible to illnesses, which may become serious and extensive. The situation is more pronounced in children. The mechanism through which illnesses can be harmful to the nutritional status of children include: reduced food and water intake due to anorexia; diminished absorption and utilization of ingested food; increased nutrient and water losses; increased metabolic demands and therefore higher nutritional requirements; alteration of metabolic pathways and the intentional reduction or complete withholding of food4. The impact of illnesses on growth may vary according to previous nutritional status of the child, the availability of food and access to health facilities1. In Kenya studies show that higher prevalence of malnutrition is associated with higher morbidity rates 5 6 7 8 9. In recent years, epidemiologists and social scientists have focused attention to studying the relationship between illness and health seeking behavior 4 9 10 11 12. Evidence on health seeking behavior has been documented in a few local studies 6 9. Kenya’s national nutrition survey results in 1994 indicate that the proportion of the population that visited health centers/ dispensaries and other medical institutions consisted of a mere 21% whereas 73.9% bought drugs from the pharmacy and retail shops that stocked the drugs and 5% took no action or visited the traditional healer 6 7 13. Diseases and nutritional disorders causing high rates of morbidity and mortality among children characterize Mumias division like many other rural areas in the country. The present study investigated the prevalence of illnesses among preschool children in a rural sugarcane growing community in Western Kenya and also determined the mother’s health seeking behavior during the course of these illnesses. Methods This was a cross-sectional study carried out between November 1997 and December 1998 in 12 villages of Isongo sub-location, East Wanga (Shibinga) location, Mumias division of Kakamega district, Western Province of Kenya. The twelve villages are geographically, socio-economically and culturally similar. To capture food security patterns whose findings are reported elsewhere, the study took almost a year to complete. There are a number of drilled boreholes to supply water in the division. However, the boreholes only serve a few areas while most of the households have no access to clean water. The division is well served by schools and market places. The study area (Isongo sub-location) has seven primary schools, two secondary schools and one health center (Makunga), which serves Mumias and Lurambi divisions. There is one mission hospital and a few private hospitals and clinics. Most of the residents in Isongo-sublocation are within four to five kilometers away from Makunga health center. Electricity remains a dream for most of the residents in the area. Apart from the supply of electricity in Isongo and Makunga shopping centers, the only other supply is in Mumias town and the sugar factory. The majority of the population belongs to three main religious groups, Catholic, Protestant and Muslim. There are a number of churches and mosques in the division serving the different religious groupings. A random sample of 172 preschool was selected from 566 preschool children in the area using a formula suggested by Fisher14 . The formula was found to be appropriate for this kind of household survey intended to cover an area such as this. The method ensured that all eligible children from the sampled sub-location had an equal chance of being included in the survey. All the eleven villages of Isongo sub-location were covered. Each household was visited once and the household-heads and the mother of the child interviewed. Information on demographic, socioeconomic and child characteristics, which included the children’s health status, in the past week prior to the survey, severity of the illness and the mothers’ health seeking behavior, was collected. The health status as well the severity of the illness of the children was ascertained by recall information from the mothers. Anthropometric measurements of the children, which are reported elsewhere, were also taken to determine their nutritional status. The questionnaires, which were in English, were translated into Kiswahili (the national language) and later back to English. The interviews were conducted in Kiswahili. Pre-testing and practical interviewing exercises were conducted repeatedly among the research assistants and mothers from the neighboring location before carrying out the actual survey. Semi structured interviews were conducted with key informants including three nurses/midwives, clinical officer, nutrition field worker and two community health workers who were randomly selected from the staff at the health center. In addition to the interviews, focus group discussions were held at Makunga Health Center with various members of the community who were purposively chosen. The discussion group of twenty people comprised of community leaders, sugarcane farmers and other key leaders from the community who were invited to the meeting by the village elders. Each village had one representative. The objective of the focus group discussions was to collect more information on the prevalence of illnesses among the children, healthseeking behavior, health services and improvement of the health of the children. The principal investigator guided the discussions, which were recorded, on a tape and later on transcribed. The results of the focus group discussions have been integrated in all the relevant sections of the research. At the end of each day, the principal investigator went through the completed questionnaires to check for completeness and accuracy. The data was entered into the computer using Dbase IV program for windows 95.The Dbase IV files were imported and converted into SPSS Version 7 for windows 95 program for cleaning and statistical analysis. Descriptive statistics were used in data analysis. Responses from some of the qualitative data were coded and frequencies determined. Cross-tabulations were used in establishing relationships between variables at a significant level of (P=0.05). ApprovalThe Ministry of Research Science and Technology approved the research by granting a research permit. Contacts were established with the District Commissioner’s office, the chiefs, assistant chiefs and the village headmen. The District Health Management Team approved the use of the government health facility for information and discussions during the study. All the study procedures were explained to the mothers and their verbal consent sought before their involvement in the study. Use of numbers on the questionnaires instead of names ensured confidentiality. Results There were eight categories of symptoms of disease reported among children in this study. These included: cough and colds, fever, diarrhea, vomiting, skin infections, lack of appetite and others. One hundred and two (59.3%) of the study children had had at least one illness in the week prior to the survey. Fever was the most commonly reported symptom with 49 (48%) cases. Table 2 shows the numbers and percentages of children with selected symptoms of illness. Information from the health facility indicates that malaria is endemic in the area. In addition, the illnesses treated at the health facility seemed to be similar with symptoms of diseases reported among children in this community. (Table 1) Severity of infections and mother’s health seeking behaviorRelationships were drawn between maternal age, number of years of schooling, severity of illnesses and the mother’s health seeking bahaviour patterns. Findings indicate that the mother’s responses and action were influenced by their perception of severity of the illness, which was classified as mild, moderate, severe and length of the illness. Only 40% of the respondents classified the illness of their children as severe. Over half (28%) of the mothers whose children had had fever considered it to be severe followed by diarrhea (7%) and vomiting (5%) compared to skin infections, colds and coughs which were considered to be mild. Little or no action was taken for these symptoms. It was assumed they would heal in their own time. In a few cases, having had a previous episode of an illness influenced the mother’s action. Previous episodes of an illness were determined from the mother’s recall information. Study findings indicate that there was substantial variability in estimating the length of the different symptoms ranging from about three days of fever to seven days of constant cough. The mother’s health seeking behavior varied from purchasing over the counter drugs, taking the child to hospital to doing nothing. Cross-tabulations were used to establish the relationship between the length of the illness and mother’s health seeking behaviour. This was found to be significant (P<0.05). The longer the illness the more likely a mother would seek help or take action. Table 3 illustrates the mother’s health seeking behavior whereas Table 4 shows the types of illnesses and action taken by the mothers. Associations were drawn between the mother’s years of schooling and her health seeking behavior. Mothers with more years of schooling tended to take action by either buying drugs or taking their children to hospital as compared to mothers with less years of schooling. Although educational level, which was determined by the number of years of schooling, had no statistical significance in comparison with severity, women who were less educated were likely to perceive greater severity than people with higher educational levels (29% vs.19%) respectively. Table 5 shows the factors that determined the mothers’ behaviour patterns.The mothers of the children were grouped into various age categories and associations made. There were marked differences in the behavior patterns when mothers were grouped under forty and above forty. Of the mothers who took action, majority (35.8%) were young (under 40) compared to the older (27%) mothers (above 40) who more often did nothing. The general bahaviour pattern was to do nothing, then attempt to self-treat with over the counter drugs based on knowledge on symptoms and then seeking help from the health provider or traditional healer or attendant. Types of drugs purchasedBased on self-report, mothers who purchased drugs were asked the types of drugs they purchased when their children had specific ailments. The drugs purchased by the mothers from the local shops and pharmacies varied with some of them being quite common. Table 6 shows the different types drugs bought by the mothers and the symptoms being treated (based on recall information on illnesses and the drugs purchased). Sources of information on the drugs purchased ranged from the mass media particularly the radio, friends or neighbors, availability of drugs, their price and drugs having been previously prescribed by medical personnel. Proximity to the health facility and availability of fundsApart from severity and length of the illness, a mothers’ health seeking behavior was influenced by other factors. Mothers whose behaviour patterns included: purchasing over the counter drugs, consulting the traditional healer, using traditional medicine and doing nothing were asked why they took the various decisions regarding their children’s illnesses. Reasons given ranged from proximity to the health facility, lack of funds, convenience and lack of adequate services at the health facility. Of the mothers whose children had symptoms of disease, almost a third (29.2%) indicated that they would have sought professional medical services if the health facility were near. For most of these households, the nearest government health facility was about 4 kilometers away. This may suggest that participants who were located near a health care facility were more likely to visit the health facility at the time of illness than those who lived far. In a number (33%) of cases, the respondents indicated that they would have preferred to take their children to a health facility or qualified personnel but they lacked funds. This was as reported by the mothers of the children. Alternatively, even if they took their children and the medical personnel prescribed drugs they may not afford the medications. Discussion The results of our study show that on the whole children suffer from a number of ailments particularly fever, which may be a symptom of malaria. The morbidity pattern in this study is similar to what has been reported in other local studies in the country 6 7. Human health seeking behavior, which is the action people take when dealing with an illness, is influenced by a multiple of factors. Some of these factors are predisposing characteristics such as age, gender, occupation, education and other enabling factors such as proximity to the health facility, health insurance, income and existence of social networks 15. It is possible that some of these outcomes could not be clearly depicted in this study due to the small sample size and one weeks recall period. In this study, most mothers did nothing as their first response to the symptom of illness experienced by their children regardless of perceived severity. Only when the illness progressed and children were unable to eat or play then mothers were likely to take action. It is important to note that the decision to seek help was most often precipitated by the impairment of the child’s daily activities or fear of severity. Mothers in this study, purchased over the counter drugs for their sick children. This finding is consistent with what has been reported elsewhere 15 16 17. The findings of this study are an indication that, households seem to have shifted from making use of professional medical services a situation which is dangerous for the general health of the population and therefore worth giving proper attention. This is because some types of illnesses diagnosed by households may turn out to be different from what is diagnosed by a qualified medical practitioner. In general, families are more likely to seek treatment when a child experiences fever, diarrhea and vomiting as compared to colds, coughs and skin infections. This may due to these illnesses being considered severe, as the effects of dehydration are immediate and detectable. Additionally, the illnesses are major causes of mortality and morbidity among children in developing countries 16. Tassema and others made similar observations in an Ethiopian study 17. The findings of this study indicate that other enabling factors such as proximity to the health facility and availability of funds were also important in determining health-seeking behavior. Whereas a few mothers cited availability of funds and proximity to the health center as reasons for alternative health seeking behaviour, these issues require further exploration before definite conclusions can be drawn. In this community, sugarcane, which is the main source of income, requires along time between initial planting and harvesting. Majority of the households do not have regular sources of income as they depend on the sugarcane payments that are made in lumpsum almost after three years of planting the crop and delivering to the factory. The mode of payment determines the expenditure patterns. Income received in lumpsum is spent differently from small regular streams of income. There is therefore need to split payments into portions and spread them over longer periods so that households have more regular payments. Alternative sources of income by households may ensure basic household needs such as medical care are taken care of. Tassema and others in a study in Ethiopia showed that the health care expenditure increased linearly with income 17. Although these findings are based on one government facility, they seem to suggest that services in government rural health facilities are poor. That is why in a few cases mothers may not take their children to these health facilities. This has been previously documented in studies in India 18 19 20. The parent’s schooling particularly that of the mothers is likely to influence their behavior in seeking health care services for their children. Our results show that the mother’s health seeking behavior was influenced by the number of years of schooling. In number studies, the education of the mother is associated with a greater commitment to the care of the child. Educated women tend to provide better healthcare, hygiene and are more likely to seek help when a child is ill 15. In India, a persons work status and monthly household income were significant explanatory variables for seeking care 18 21. Primary health care services in this study area and many other rural communities in the country need consideration by planners and healthcare providers. Community based primary health care services such as mobile clinics and improved socioeconomic status of the families is likely to benefit the community. It is noted that illnesses in this study could not be properly described or classified without a complete report of symptoms and verification by the medical personnel. The authors therefore depended on information on the diagnosis as described or perceived by the mothers of the children. Conclusion Our study has exposed the burden of illnesses among preschool children at household level in this community. Primary health care services in this study area and many other rural communities in the country need consideration by planners and healthcare providers. Community based primary health care services such as mobile clinics and improved socioeconomic status of the families is likely to benefit the community. These conclusions are made in view of two main limitations experienced by study. The survey involved a single cross-sectional interview in which mothers recalled the illnesses experienced by their children and their behaviour within a week’s period. Due to this, the data was not detailed enough to permit meaningful statistical analysis of the relationship between illness and treatment behaviour. Secondly, whereas the sample was drawn from a rural community it may be small for any general conclusions regarding illnesses and behaviour patterns. Acknowledgements The first author is grateful to the German Academic Exchange Service (DAAD) for funding the research, the mothers of the study children for their patience and the staff of Makunga Health Center for their cooperation and assistance. This paper is part of PhD work for the first author. References
Copyright 2005 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs05057t2.jpg] [hs05057t5.jpg] [hs05057t6.jpg] [hs05057t3.jpg] [hs05057t4.jpg] [hs05057t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}