 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
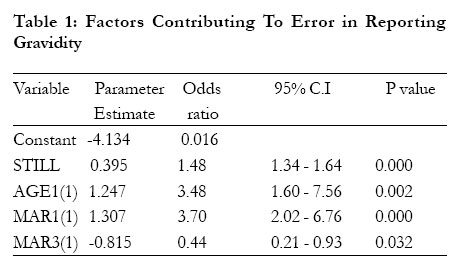
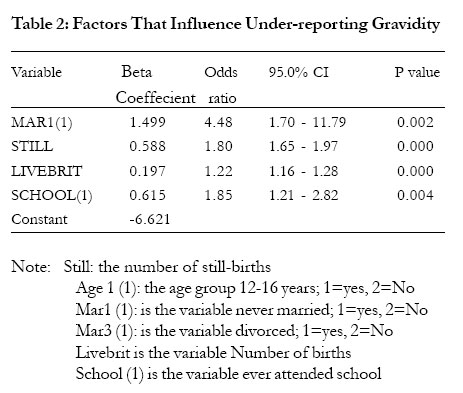
African Health Sciences, Vol. 5, No. 4, December 2005, pp. 335-337 Under-reporting of gravidity in a rural Malawian population Humphreys E. Misiri, Adamson S. Muula Department of Community Health, University of Malawi College of Medicine, Blantyre, Malawi Code Number: hs05059 Abstract Background: Mis-reporting of data by study participants in a questionnaire-based study is an important source of bias in studies. Introduction In most surveys, questionnaires are used as a data collection tool. Questions in these questionnaires may involve provoking the respondent to recall some episodes in their life. Recall questions introduce bias as not many people may be able to recall accurately personal life events. Recall errors could be under –reporting; when a respondent understates an event or over-reporting where a respondent gives an answer which is an overstatement of what actually happened. This under or over-reporting is sometimes deliberate more especially when the questions are asking for sensitive details which the respondent regards as embarrassing. Under-reporting and over-reporting occur in many surveys. Niccolai et al. 1 report the occurrence of underreporting sexually transmitted diseases as ranging from 21% to 47% and they suggest using multiple sources of information about the same issue the respondent is asked to give details about as a way of reducing errors in reporting that can be picked up during data analysis . In a study of use of hospital emergency department by Dendukuri et al,2 an incidence of lower sensitivity (or under-reporting) on the self-report appeared to be associated with higher age, low co-morbidity and shorter length of recall . Rennie et al 3 also report the incidence of under-reporting in reporting energy intake among young people. Diabetes is also under-reported in New Zealand as evidenced by Coppell et al 4. In this paper, we report on factors affecting low reporting of gravidity and parity in a rural Malawian population. We are unaware of any previous studies that reported these phenomena in a Malawian setting. Methods In a cross sectional study, socio-demographic data were obtained using a structured questionnaire in a census of Lungwena area, a rural area in Mangochi district in Malawi, on the eastern shore of Lake Malawi. A total of 5174 households were recruited, with a population of 27,103 people , only 7118 (26.3%) were women of child-bearing age. Two logistic regression models have been fitted using SPSS Release 11. One model has the logit of the probability of making an error in reporting as the response. The second model has the logit of the probability of under-reporting as the response 5. Descriptive statistics have also been computed by the same statistical software. For the purposes of this study, analysis was done only for the women in reproductive age group. The following variables were included in the census questionnaire: total pregnancies, total number of live births, total number of still births and the total number of children. The sum of the total number of still births and the total number of live births is what should be the actual gravidity of the respondent. The difference between the reported total pregnancies and this sum is the discrepancy or error in reporting gravidity by recall. If this is positive, then the respondent under-reported gravidity. If this difference is negative, the respondent must have over-reported gravidity. Lungwena area has been identified as a research community for the University of Malawi and various research especially regarding maternal and child health has been done in this area 6-8. The study was conducted in Lungwena area in order to obtain baseline information in the area after several years of maternal and child health interventions by the College of Medicine. The area is also a research site for other constituent colleges of the University of Malawi, this information was considered vital for the development of programs that may aim to improve the socio-economic status of the area. Up to 85% of the population of Malawi is rural-based and in this regard, this may represent the majority of the population. It is however important also to note that the area studied is a Yao dominated area, the majority are Moslems, and lineage in matrilineal. These characteristics may be represented in other areas of Malawi but not universally. As this was a census, data was collected in all households within Lungwena. Results Participants demographic Characteristics Misreporting of Gravidity From the data, 6553(92.1%) correctly reported gravidity, 159(2.2%) under-reported gravidity and 5.7% (406) overreported gravidity. Factors related to mis-reporting are presented in Tables 1 and 2 below. From the first model fitting results, it is seen that the number of still births (p <0.00001), being divorced or not (p =0.032), being never married or not (p<0.00001) significantly affect accuracy in reporting gravidity among women of child bearing age. The odds of inaccurately reporting gravidity is 3.48 times higher for women aged between 12 and 16 years than for women aged between 17 and 49 years. The odds of error in reporting gravidity is 3.70 times higher for women who never married than for women of other marital status. The odds of error in reporting is 2.27 times higher for women of other marital status than for divorced women of child-bearing age. The odds of error in reporting increases with a multiplicative factor of 1.48 for each unit increase in the number of stillbirths. From the model fitting information for the second model, it is seen that only marital status (married or not married), p=0.002 number of live births and stillbirths (p < .0001) and schooling (p=0.004) significantly contribute to underreporting. The odds of under-reporting is 4.48 times higher for those who never married than for child-bearing women of other marital status. The odd of low reporting gravidity is increases with a multiplicative factor of 1.8 and 1.22 for each unit increase in the number of stillbirths and live births respectively. The odds of under-reporting gravidity is 1.85 times higher for women who attended school than for women who never attended school. Discussion The present study found the prevalence of mis-reporting of pregnancy of 7.9% in a rural area on southern Malawi. Increasing number of still births, having never been married and ever having attended school increased the chance of underreporting gravidity among women of childbearing. There could be several reasons why this may be the case. As for women who may have had stillbirths, they may not have wished to report this as pregnancies as culturally in Malawi, the tendency is to report the live-births and neglect still-births. It may also have been painful to some women to be reminded of previous still-births and so reporting as if these never occurred may have been preferred. Woodward et al 9 reported that women who had low-birth weight babies were less likely to register their infants than those with adequate weight. Women who may not having been married may have under-reported gravidity for quite different reasons. In a community where not being married is looked down upon, having a pregnancy outside marriage is cause for stigma and individual low self-esteem. Perhaps fearing censorship from the interviewer respondents decided not to report pregnancy for fear of being categorized as ‘loose’ and ‘irresponsible’ for having a pregnancy outside marriage. Women with some education also underreported gravidity. This could be due to the fact that these are more likely to be knowledgeable on contraception and the ‘expectation’ by health workers for smaller family size. Reporting that they had been pregnant a few times may be chosen in order to appear as if they had heeded family planning messages. Uptake of contraception, though increasing continues to be low in sub-Saharan Africa 10. That young women aged 12-16 years were 3.5 times more likely to misreport gravidity than child women aged between 17 and 49 years is also of interest. This could be due to the same reason that young women could have censured themselves by thinking that they ought to have been in school, ought to have postponed child bearing and not to have married (for those married) as early as they did. They would therefore have reported lower gravidity. The fact the questionnaire was interviewer-administered may have introduced some biases in the ability of women to report the actual number of pregnancies they may have had. It must be appreciated that the validity of responses in a study like ours depends on the accuracy or recall, the truthfulness of reporting events and understanding the questions 11. We have determined that being young, unmarried, having experienced a still-birth is associated with under-reporting of number of pregnancies amongst women in a rural area of Malawi. We suggest that researchers seeking information on gravidity need to be aware of this problem as this may bias the data and the interpretation. Having multiple questions scattered within the questionnaire asking more or less the same thing, may facilitate detection of mis-reporting as they may serve as consistency checks. Acknowledgements We are grateful for Dr. Ken Maleta for permission to use the data from this census. Funding for the data collection was obtained from the Government of Norway, through the Norwegian Council of Universities’Committee for Development Research and Education (NUFU). References
Copyright 2005 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs05059t1.jpg] [hs05059t2.jpg] |
| |||||||||

{kind=link}
{kind=link}