 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
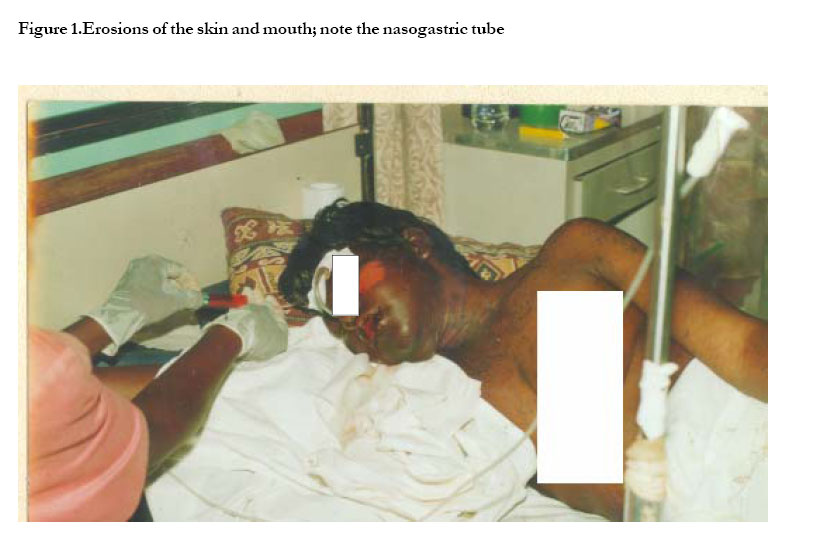
African Health Sciences, Vol. 5, No. 4, December 2005, pp. 338-340 CASE REPORTS Stevens –Johnson syndrome due to nevirapine G. K. Namayanja, J. M. Nankya, J. K. Byamugisha, F. N. Ssali, C. M. Kityo, S.D. Rwambuya, R. D. Mugerwa, F. A. Mmiro, C. S. Morrison, R.A.Salata Correspondence author: Byamugisha K Josaphat, Makerere University Medical School, Dep’t of Obstetrics & Gynaecology , P.O. Box 7072, Kampala-Uganda. Private Box 10442,Kampala Tel: 256 41 534361/533451;fax 531364/533451 Cell Phone 075691064/077580330 E-Mail:jbyamugisha@med.mak.ac.ug, byamugisha2001@yahoo.com Code Number: hs05060 Abstract A 25-year-old HIV-infected woman participating in a study of the effects of hormonal contraception on HIV disease progression was started on antiretroviral therapy-Combivir & Nevirapine (NVP) on May 27, 2004. NVP was 200mg daily initially for two weeks to be increased to 200mg bid thereafter. On day twelve, she presented with a mild skin rash on the trunk, purulent conjunctivitis, pharyngitis and fever. She was treated symptomatically and sent home. The following day she returned with a generalized erythematous eruption. She was admitted to JCRC (Joint Clinical and Research Centre) on June 14 and was diagnosed with Stevens - Johnson syndrome (SJS). Antiretroviral therapy was stopped. By July 05, 2004, she had improved and was discharged .After recovery she was restarted on Combivir and Efavirenz and is subsequently doing well on this regimen. Key words: Stevens - Johnson syndrome, antiretroviral therapy, generalized erythematous eruption, nevirapine Introduction First described in 1922 by Stevens and Johnson, Stevens -Johnson syndrome (SJS) is an immune complex hypersensitivity reaction that can be caused by many factors such as infections, drugs and malignancies. Recent reports have linked SJS to the use of drugs rather than other etiologic factors. Antibiotics e.g. sulphonamides are the most common cause of SJS, followed by analgesics, cough and cold medication, nonsteroidal antiinflammatory drug (NSAID), psycho-epileptics, and antigout drugs¹. Nevirapine has also been implicated in the pathogenesis of SJS2, 3. There may be a genetic predisposition to developing SJS3. We hereby report a case of severe SJS. Case history and examination findings A 25 yr old female participant in the Genital Shedding study (GS) is presented. This study is under the Makerere University-Case Western Reserve University (MU-CWRU) research collaboration. She was initially in the Hormonal Contraception and risk of HIV acquisition (HC-HIV) study. This was a longitudinal multi-centre multi-site study which followed women who were HIV negative. The women were followed every three months for a period of 15 –24 months or until HIV sero conversion. Women who became HIV-infected were invited to join the GS Study; informed consent was sought and provided prior to enrollment in the study The client was enrolled in the HC-HIV study on February 2, 2000 and tested HIV-negative at that time. At her visit on March 27, 2001 she first tested HIV-positive. She enrolled in the GS study on June 6, 2001 with a CD4 count of 843cells/mm³. She had vaginal candidiasis and was treated with clotrimazole vaginal pessaries. In January 2003 she developed otitis media, which improved on treatment with Erythromycin 500mg q.i.d for one week. She developed genital herpes in March 2003 and her CD4 cell count dropped to 324 cells/mm³. In September 2003 she presented with a generalized pruritic papular rash. Her weight had dropped from 58 kg to 53 kg (8.6% weight loss). On December 1, 2003 she had vaginal candidiasis which was treated with Ketoconazole 200mg o.d. for seven days and she improved. In February 2004 she had a pruritic papular eruption (PPE) again, oral hairy leukoplakia, and vaginal candidiasis. In May 2004 she presented with vaginal candidiasis, PPE and 10% weight loss (WHO stage III disease). The candidiasis was now poorly responsive to anti-fungal therapy (Fluconazole, Ketoconazole). Her CD4 count had dropped to 220cells/mm³and her viral load was 68,073copies/ml. The study HIV consultant recommended that she starts Anti-Retroviral Therapy (ART) based on WHO stage III disease coupled with the client’s willingness and commitment to take ART. She started Nevirapine 200mg once daily and Combivir 450mg twice daily on May 27, 2004. Twelve days later she came in with a mild skin rash on the trunk, purulent conjunctivitis, pharyngitis and fever. She was treated as a mild grade 1 Nevirapine rash and went home to continue with ART and was advised to come back if symptoms worsened. She returned the following day with a diffuse erythematous rash on the face, trunk and upper limbs. The oral mucosal erythema and ulceration was progressive and caused difficulty in swallowing. Nevirapine was discontinued and Combivir continued for 3 days then withdrawn. The initial intention was to overlap the Nevirapine with Combivir for seven days but this was not possible because of esophageal pain on swallowing. A pus swab was taken from the eyes and throat. The eye swab cultured staphylococcus aureus and throat swab cultured a non-significant growth of streptococcus viridans. She was hospitalized at the JCRC and treated symptomatically with oral morphine, cloxacillin, tetracycline eye ointment, nursing care, nasogastric tube for feeding, and I.V fluids for rehydration. While on the ward she developed oral ulceration and generalized bullous lesions. Some of which ruptured leaving a denuded skin (figure I). Investigations during hospitalization Blood slide showed plasmodium falciparum + and she was treated with metakelfin. ALT and AST were normal at 33.7 iu/l and 36.0 iu/l, respectively. Serum creatinine was 1.01mg/dl and serum amylase was 75.8 iu/l. Complete blood count was wbc-4500/cubic mm. Red blood cells were 4.65 million/cubic mm and lymphocytes were 24.7%. Haemoglobin level was 12.5g%, haematocrit was 36.2% and platelets were 139,000/cubic mm. Wound hygiene was done regularly. Her vital signs were monitored and her skin, oral ulceration and wounds healed after 25 days of intensive care. The odynophagia slowly receded until she was able to feed orally and she was discharged. A week later she was reviewed and found to be in good general condition. However, she had developed mouth contractures and could only open her mouth partially. Three weeks after discharge she was counseled and given a modified regimen of Combivir (CBV) and Efavirenz (EFV). Her viral load was 94,955copies/ml and her CD4 was 290cells/mm3 at the start of treatment. During her first month on CBV + EFV she complained of insomnia which later subsided. The drug rash did not recur. The participant is doing well on Combivir and Efavirenz and is adherent as seen from her pill count and pill calendar, as well as self-report. As of July 2005 her CD4 count was 678cells/mm3. The contractures healed on physiotherapy. Discussion Stevens - Johnson syndrome is a severe cutaneous disorder characterized by acute skin blisters and mucous membrane erosions. Previous studies reported that most cases of SJS in HIV infected patients were related to antibacterial sulphonamides in Western Countries and to thiacetazone in Africa. Investigators from Uganda reported two cases of SJS that occurred in a mother and her eight year-old son who both took nevirapine in combination with d4T and 3TC³ .Individuals with antigens human leukocyte antigen Bw44, HLA-B12, and HLA-DQB1*0601 appear to be more susceptible to developing SJS. It affects all ages and both genders¹. The disease process usually begins with a non specific upper respiratory tract infection and is usually part of a 1 to 14 day prodrome during which fever sore throat, headache, and malaise may be present. In a multinational case-control study done in Europe (EuroSCAR study) between May 1997 and November 1999 on 246 patients with SJS, the reaction began 10-240 days (median 12 days)2. Vomiting and diarrhea may occur during the prodromal period. A history of fever or localized worsening has been reported to occur in up to 85% of cases4. Involvement of oral and/ or mucous membranes may be so severe that the patient is not able to eat or drink. This was the situation with this patient. The mucosal membrane involvement was so great that even drinking became very difficult and she had to be on intravenous fluids and N-G-tube (fig 1).The rash may develop as macules that develop into papules, vesicles, bullae or confluent erythema. The rash may be confined to any one area of the body. The findings on examination will depend on the stage at which the patient presents and include fever, conjunctivitis, epistaxis, corneal ulcerations, vulvovaginitis, tachycardia, altered level of consciousness and at times seizures and coma. Investigations include a complete blood count (CBC).This count may be normal. A markedly elevated count may indicate a superimposed infection. Renal function tests, electrolytes and other chemistries may be needed. Cultures of blood, urine, and wounds are indicated when an infection is coexistent. Skin biopsy is a definitive diagnostic study and indicates that the bullae are sub epidermal, epidermal cell necrosis may be noted and perivascular areas are infiltrated with lymphocytes4. It should be noted however that a biopsy is not an emergency. Treatment of SJS is primarily supportive and symptomatic. Consultations may help establish the diagnosis with or without biopsy and are usually necessary depending on organ or system involvement Prognosis: Individual lesions may heal within 1-2 weeks unless secondarily infected. Patients may recover without sequelae; however, this is usually not the case. The SCORTEN score uses variables to prognosticate risk factors for death from SJS4. The variables include age>40 years, malignancy, heart rate>120, initial percentage of epidermal detachment>10%, BUN>10mmol/l, serum glucose >14mmol/l, and bicarb 20mmol/l. Lessons learned One must have a high index of suspicion to be able to diagnose and treat patients with SJS in time. This is critical for the subsequent survival of these patients. Intensive treatment must also be done together with specialist physicians, where available. One must be careful and suspect SJS if a patient on an ART regimen containing NVP presents with symptoms arising from irritation of the skin and mucous membranes. References
Copyright 2005 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs05060f2.jpg] [hs05060f1.jpg] |
| |||||||||

{kind=link}
{kind=link}