 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 5, No. 4, December 2005, pp. 345-347 PRACTICE POINTS Ano-perianal tuberculosis - solving a clinical dilemma Gupta P J. Consulting Proctologist, Gupta Nursing Home, D/9, Laxminagar,
NAGPUR- 440022, INDIA. Code Number: hs05063 Abstract
Background: Tuberculosis is one of the causes of granulomatous disease
within the anorectal region. The clinical features, which include symptoms
and signs of anal pain or discharge, multiple or recurrent fistula in ano and
inguinal lymphadinopathy, are not characteristically
distinct from other anal lesions. It is also difficult to distinguish it
from other granulomatous diseases involving the same area. Keywords: Anal, perianal, tuberculosis, suppuration, recurrent. Introduction Extra pulmonary tuberculosis accounts for 5% of all case of tuberculosis. Perianal tuberculosis is a rare extra pulmonary form of the disease1. It can have varied presentation, frequently mimicking other common as well as rare diseases2. Ano-perianal tuberculosis may be associated with abdominal tuberculosis either as an extension of the original lesion or due to its spread via the lymphatics.3 Lesions of the abdominal organs are more common while the anal localization still is a rare occurrence (0.7%)4. Medline [1965-2005] was searched for all published reports using the key word ‘ anal’, ‘tuberculosis’ and ‘Koch’s’. This study sum up the clinical features of this entity, the main diagnostic and therapeutic advances, important points of distinction with other ano-perianal lesions and the best possible approach towards the treatment of the pathology. Pathogenesis The postulated mechanisms by which tubercle bacilli reach the perianal region are: 1) Hematogenous spread from the primary lung focus in childhood with later reactivation; 2) ingestion of bacilli in sputum from active pulmonary focus; 3) direct spread from the adjacent organs; and 4) through lymph channels from infected nodes.5 Most frequently encountered anorectal tuberculous lesions are suppurations and fistulae6. Other presenting features may be anal pain, fever and cough, anal or perianal ulcer with purulent exudates and a nonhealing wound around the anus7. Anal strictures, hemorrhoidal thrombosis with fever and purulent discharge are few others to mention8. A good digital examination is usually sufficient to diagnose an anal fistula. Nearly all fistulas are complex, and secondary tracks or additional complicating features are commonly found even at first presentation9. Tuberculosis can be a part of the complicating infection of HIV-positive patients.10 The incidence and severity of ano-perianal tuberculosis are increasing with increasing incidences of HIV infection.11 Various forms of ano-perianal tuberculosis Tuberculosis is known to manifest through many atypical and unexpected clinical presentations. These variables are often encountered in the proctology practice. They may present as pilonidal sinus12 or anal ulceration with inguinal adenopathy.13 Recurrent perianal growth, anal fissure,14 anal strictures,15 and rectal submucosal tumor16 are few other atypical presentations of the disease. Investigations
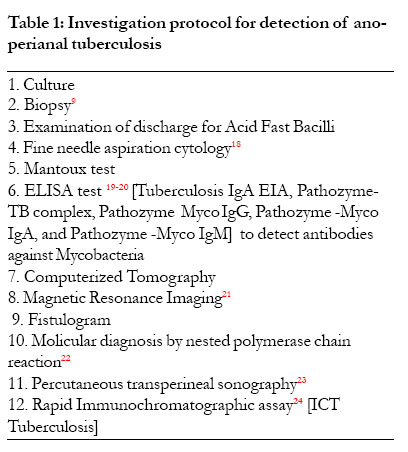
Despite availability of several tests, early diagnosis of anal and perianal tuberculosis remains a challenge. In countries like India, the search begins with the routine tests as total leucocytes count, Erythrocyte Sedimentation Rate, Mantoux test, detection of acidfast bacilli in the discharge or tissue section from the lesion.17 Clinical diagnosis is usually dependent on microscopic detection using Ziehl-Neelsen stain6 and mycobacterial culture7, but the sensitivity and specificity of these two methods are low. This necessitates tests that are more specific to come to a definite conclusion. A battery of investigative tools listed below are available to accurately diagnose the disease. The serodiagnosis of tuberculosis has long been the subject of controversy, as we sadly lack a test with widespread clinical utility. The overall sensitivity of these tests for extra pulmonary tuberculosis is as low as 16.7%.25-26. The simplest rapid method for diagnosis of the disease, perhaps, is the detectionof acid-fast bacilli by microscopy. However, 75% of patients with extra pulmonary tubercular disease are smear negative, and in the situation even contemporaryculture methods might take several weeks to become positive27. Histological examination of the excised fistula is mandatory for the diagnosis of anal tuberculosis. In other perianal pathologies, ridge biopsies of the growth or histopathological study of excised lesion helps in clinching the diagnosis.5, 7 Experience shows that triads of FNAC, AFB smear, and culture are cheaper, error free, and confirmatory when compared to costlier tests like TB IgG, IgM, or ICT tests28. Differential Diagnosis
Perianal cutaneous ulcerations in tropical countries have multiple causes: bacterial, viral, and parasitic. Infections, such as amoebiasis, foreign body reaction, sarcoidosis, syphilis, venereal lymphogranuloma and actinomycosis have to be explored in priority9. Crohn’s disease and tuberculosis pose major diagnostic problems for clinicians where these conditions coexist26. The necessity of careful study in differentiating the lesion from carcinoma could not be overemphasized. Few other clinical conditions mimicking tuberculosis are hidradinitis suppurativa, bartholinitis, radiation injuries, lymphomas and antibiomas. (Table 1) Discussion Infection by Koch’s bacillus is still a public health problem both in the underdeveloped and in developed countries where the human immunodeficiency virus is gaining epidemic form, the appearance of multi-resistant bacilli, large immigrant populations and poverty bringing along unknown organisms and lack of hygiene and education all play their part in the increased incidence of the disease. 2 Anal fistula is the most frequent symptom of anorectal TB (80–91 percent of cases). Unfortunately, there is no functional sign or preferred site that allows a tuberculous fistula to be distinguished from a cryptoglandular fistula. 4 The ulcerated form of anal TB typically presents as a superficial ulceration, not hardened, with a hemorrhagic necrotic base that is granular and covered with thick purulent secretions of mucous. The lesion may be very painful, or the patient may have few symptoms. 5 The tuberculin skin test remains a valuable guide because it is positive in 75 percent of cases, a negative tuberculin skin test in a patient who is not immunodepressed that is associated with a normal lung x-ray makes the diagnosis of anal TB improbable. 9 Positive diagnosis of anal TB depends on histologic or bacteriologic analysis.11, 12 The typical histologic lesion is the epithelioid and giant cell tubercle around a zone of caseous necrosis, but the pathognomonic presence of caseation is not constant, and presents diagnostic problems, especially in the case of Crohn’s disease with anoperineal localization. 26 Diagnosis can also be done by looking for Koch’s bacillus in the anal lesions by direct examination (Ziehl-Nielsen stain) and culture. To overcome the slowness of the culture (3 to 4 weeks), new diagnostic techniques for TB have been proposed, in particular genomic amplification by polymerase chain reaction, which can detect the presence of the bacterial DNA in 48 hours with high sensitivity. 22 Sometimes, a cluster of epidemiologic, clinical, histologic, radiologic, and evolutive arguments can contribute to the diagnosis of anal TB. These may include the origin and social class of the patient, previous history of TB, recurrent anal suppuration, weight loss, fever, night sweats, chronic dry cough, positive reaction to the tuberculin skin test, epithelioid granulomas without caseous necrosis on a sample from the lesion, associated evolutive pulmonary or digestive TB and favorable and rapid response to antituberculosis treatment.1 Anal TB necessitates specific antibiotic therapy under rigorous supervision. Although in certain cases the fistula may heal after antituberculosis treatment, surgical removal of tuberculous fistulas is necessarily recommended as standard procedure. There is a high prevalence of anal lesions as a result of acquired immunodeficiency syndrome that is estimated as being between 16 and 34 percent. Although the incidence of TB is increasing in these patients, especially in extra pulmonary forms, the anoperineal region is only exceptionally affected. There appears to be a reciprocal Koch’s bacillus/HIV potentiation; in fact, Koch’s bacillus stimulates the propagation of HIV through released growth factors. The immunosuppression caused by HIV brings about a deterioration in the functions of different types of cells (B and T lymphocytes, natural killer cells, and macrophages) that leads to reactivation of latent seats of mycobacteria, which are generally localized in pulmonary adenopathies. Sexual transmission of Koch’s bacillus during anal intercourse has already been postulated, but never been proved.10, 26, 28 To conclude, ano-perianal tuberculosis can be present with or without the lungs being affected and can be diffused. Management is with conventional anti tubercular therapy for at least 6 months. The recommended surgical procedures today are conservative and a period of preoperative drug therapy is controversial. References
Copyright 2005 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs05063t1.jpg] |
| |||||||||

{kind=link}