 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 6, No. 1, March, 2005, pp. 14-20 Burden of alcohol use in the Uganda Police in Kampala District Emilio Ovuga1, Charles Madrama2
Correspondence: Emilio Ovuga, Department of Psychiatry, Makerere University, P.O. Box 7072, Kampala, Uganda. Fax: 256 41 231289 E-mil: emilio.ovuga@gmail.com, emilio_ovuga@hotmail.com Code Number: hs06003
Abstract Background: Alcohol dependence is one of the leading causes of the global burden of disease.Among members of the Uganda Police Force, alcohol dependence has been a major contributor of poor mental health, poor work output and forced retirement. Background
Four of the top ten causes of the global burden of disease are mental disorders including Unipolar major depression, alcohol and substance abuse, schizophrenia and obsessive compulsive disorder 1-4. The basic tenet in the concept of disease burden is that a chronic illness imposes restrictions in how fully the individual can function and or make free choices in life. However it is not always easy to comprehensively measure the impact of chronic illnesses since it may not be possible to measure the hidden and undefined burden of such illnesses 5. In the case of alcohol dependence, possible ways to measure the burden of disease would be to determine the prevalence of alcohol use in the population, or the prevalence of liver cirrhosis or cancer, mortality associated with liver cirrhosis or cancer, or fatal accidents positively associated with alcohol use. It is also possible to infer alcohol related disease burden by estimating the prevalence or incidence of psychiatric disorders or suicide and attempted suicide associated with primary alcohol use in the population. Information from the Uganda Police Headquarters showed that one hundred seventy seven officers had been admitted to Butabika Hospital due to alcohol related problems from 1992 to 2002. On average, 12 police officers per 1000 were admitted to the mental hospital per annum from an estimated population of 14,000. During the early part of 2002, at least 350 police officers were implicated in alcohol related disciplinary problems. The present study was conducted to determine the magnitude and psychosocial problems associated with the use of alcohol by members of the Uganda Police Force (UPF) in Kampala district. The aim of the study was to highlight the public health importance of alcohol dependence in the UPF in relation to implications for the security of society when police officers who are entrusted with the task of guaranteeing the safety and security of society suffer from various forms of impairment associated with alcohol use. Methods of study Study design and sites A cross-sectional survey of a sample of police officers resident in two police barracks in Kampala district designated as Barracks I and Barracks II was conducted in the months of March to May 2002 using systematic sampling strategy. (The two barracks are represented with codes out of ethical need to protect the anonymity of the stations and the officers therein).The total population at Barracks I was 3505 with 701 (20%) of this being police officers. Police Officers at this barracks are responsible for security on highways and situations of unrest. At Barracks II, the total population at the time of the survey was 11,226 residents with 1618 (14.4%) of this being police officers. Sampling procedure Sampling was achieved by systematic sampling procedure using police register provided by Police Headquarters. The procedure involved drawing up a list of police officers from the rank of Constable to Senior Superintendent of Police (SSP). A sampling interval of 20 was calculated for a convenient sample size of at least 100 respondents from both barracks. The first respondent was randomly selected by drawing a lottery of the first 20 members on the list from each barracks. Thereafter, every 20th police officer was selected from the list by adding the sampling interval to the number of the last respondent. A selected officer who refused to participate was skipped and the next person on the list was selected.The procedure was continued until the list of police officers at each barracks was exhausted. The respective numbers of interviewees from the two barracks reflected the proportional size of each barracks. Thus 40 interviewees came from Barracks I and 64, from Barracks II giving a total sample size of 104 respondents. Data collection Data was collected using a semi-structure questionnaire designed for the study.The instrument included data on socio-demographic characteristics of respondents, criteria for alcohol dependence based on ICD-10 [1], and a range of medical and psychosocial problems associated with alcohol dependence in Uganda. Each respondent was interviewed at his or her residence in the barracks. One of us (CM) conducted all interviews after he was trained for the purpose. The interviewer read out each question to the respondent and recorded all answers in the appropriate sections of the questionnaire. Details of medical and psychosocial data collected Health service use: Respondents were asked if they had used hospital facilities, private clinics, or police clinic during the three months prior to the survey. The respondents also provided information on admissions to hospital on account of their own poor health. Job satisfaction: Respondents rated their level of job satisfaction along a 10-point scale. A position at or near 10 indicated a high level of job satisfaction, and that near zero indicated dissatisfaction. During analysis, the respondents were grouped according to their individual positions along the scale, namely: 0-3 for extremely dissatisfied; 4-6 for satisfied; 7-9 for moderately satisfied; and 10 for extremely satisfied. See figure 1 for the distribution of respondents according to their levels of satisfaction with their occupation. Project development: Respondents were asked if they had started a developmental project to supplement their income, or built a house in their home village. Savings: Respondents were asked to provide information on their level of monthly savings based on their salary and or other sources of income. Extra income: Respondents provided information on whether they had extra sources of income than their monthly salary. Recreational activities: Respondents provided information on the form of recreational activities they engaged in during their free times. Absenteeism: Respondents were asked to estimate the number of days off work during the past three months. Disciplinary problems: Respondents were asked if they had ever been demoted or reprimanded at work as a result of alcohol use. Ethical considerations The interviewer explained to every respondent the nature and purpose of the study and informed him or her that the study aimed to determine probable health, social, economic, psychological and work-related problems in alcohol use. Respondents were assured of complete confidentiality and anonymity. Interviewees were assured that they could refuse to participate in the study, or decline to answer any question that they did not feel comfortable providing information about. Respondents who needed health care received appropriate advice and were referred. Interviewees gave consent in the form of their usual signature, witnessed by a colleague or adult member of their household.The Butabika School of Psychiatric Clinical Officers and Police Headquarters granted permission for the study. Analysis
Data was entered and analyzed using SPSS version 11.0. Odds ratios and 95% confidence intervals were calculated using Epi Info version 6.04. In the present paper we provide prevalence figures for alcohol use, prevalence of probable alcohol use disorder (AUD) and prevalence of alcohol use problems (AUP) commonly associated with alcohol dependence in Uganda. Alcohol use disorder (AUD) The criterion for alcohol use disorder was derived from the seven features of alcohol dependence [1]. Each feature was scored one if present, and zero if absent. A score of 4 or higher on AUD was considered significant indication of alcohol use disorder. Alcohol use problem (AUP) The criterion for alcohol use problem (AUP) was derived from a list of ten psychosocial problems commonly associated with alcohol dependence in Uganda some of which are defined in the methods section above. These included absenteeism from work, disciplinary problems at work place, poor health, debt, problem paying school fees, inability implementing personal plans, fighting when drunk, social disapproval of one’s drinking habits, inability to fulfill one’s social obligations and responsibilities, and being blamed for poor work output. Each of these problems was scored “one” if present, and “zero” if rated absent by the respondent. A total score of 4 or higher was considered a significant indication of alcohol use problem. Results
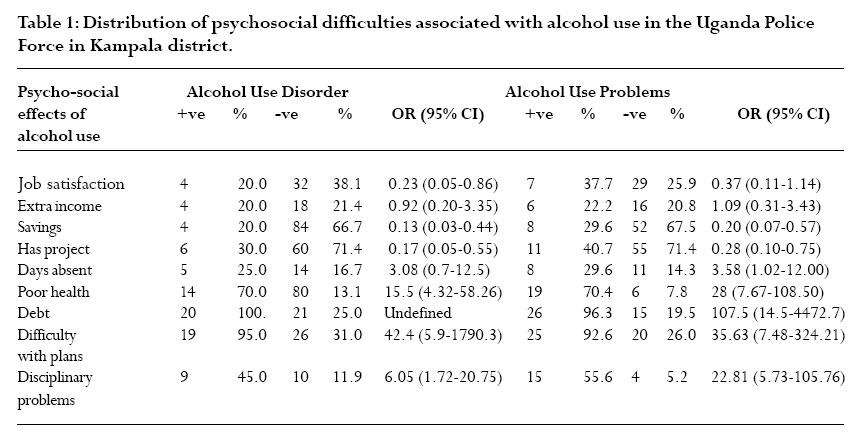
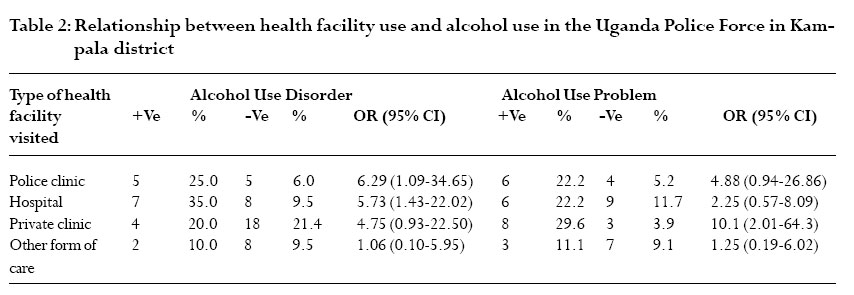
Socio-demographic characteristics One hundred and four police officers participated. Five of the interviewees (5.0%) were female and 97 (95.0%) were male; information on the sex of two respondents was missing.The mean age of female respondents was 39 years (SD=5.3), and that of males was 34 years (SD=5.9). The male predominance in the UPF reflects the recruitment profile of personnel for the police in Uganda. Ninety one respondents (89.0%) were married, five (5.0%) were single, 3 (3.0%) were separated, 2 (2.0%) were widowed, and 1 (1.0%) was cohabitant; 2 respondents had missing information on marital status. All respondents had attained the basic secondary educational level required by the UPF. Fifty six (53.8%) were at the rank of Constable and only 2 (2.0%) were at the level of SSP. See figure 2 for the distribution of respondents according to their ranks in the police force. Prevalence of alcohol use Seventy six respondents (73.1%) reported that they had ever used alcohol in their lifetime, and sixty six (63.5%) reported that they currently used alcohol.The majority of respondents started the use of alcohol in the age bracket 15-19 years, but 8 (7.7%) began alcohol use before the age of 10 years. Job satisfaction Eight respondents (7.7%) felt extremely dissatisfied with their work, and only 10 respondents (12.5%) of the respondents reported being satisfied with their occupation. Information for 4 respondents on job satisfaction was missing. Savings Sixty respondents with information on savings (57.7%) reported that they had saved from their monthly income. Extra income Twenty two respondents (21.2%) reported that they had other sources of income to supplement their monthly salary. Development project Sixty six respondents with information on project development (63.5%) reported that they had started income generating, or other developmental project since they joined the police force. Recreational activities Respondents reported that they engaged in a wide range of recreational activities and only 6 (5.8%) did not participate in any such activity. None of the respondents with alcohol use disorder or alcohol use problem participated in religious activities but they engaged in indoor games and sports where alcohol use formed part of such activities. Disciplinary problems Nineteen respondents (18.3%) reported that they had been disciplined for various reasons. Prevalence of alcohol use disorder (AUD) and alcohol use problems (AUP) Twenty respondents (19.2%) met criteria for AUD, 27 (26.0%) met criteria for alcohol use problems (AUP), and 10 respondents (9.6%) reported that their health was poor. Alcohol use disorder (AUD) Respondents who met criteria for alcohol use disorder were more than 15 times as likely as those without AUD to report poor health (X2 = 5.61, df = 1, P = 0.0000), more than 6 times as likely as those without AUD to have visited the police clinic during the past three months (X2 = 6.96, df = 1, P = 0.03), and more than five times as likely as those without AUD to have visited the hospital during the past three months (X2 = 7.36, df = 1, P = 0.007). In addition respondents who met criteria for AUD were more than 40 times as likely as those without AUD to report the experience of difficulties in implementing personal economic plans (X2 = 24.45, df = 1, P = 0.0000), were less likely to have saved from their monthly incomes than those without AUD (X2 = 12.56, df = 1, P = 0.0003) and were less likely than their colleagues without AUD to have a development project (X2 = 10.24, df = 1, P = 0.001). Respondents with AUD were less likely than their colleagues with AUD to be satisfied with their work (X2 = 4.83, df = 1, P = 0.03), and were 6 times as likely as those without AUD to report disciplinary problems (X2 = 9.74, df = 1, P = 0.002). There were no statistically significant differences between Barracks I and II in the distribution of respondents in relation to AUD. See Tables 1 and 2. Alcohol use problems (AUP) Respondents who met criteria for alcohol use problems (AUP) were more than 3 times as likely as those without AUP to report more days off work in the past three months (X2 =4.29, df = 1, P = 0.04), more than 28 times as likely as those without AUP to report poor health (X2 = 39.51, df = 1, P = 0.0000), more than 10 times as likely as those without alcohol use problems to have visited a private clinic at least twice in the three months preceding the survey, more than 100 times as likely as those without AUP to be in debt (X2 = 46.23, df = 1, P = 0.0000), more than 35 times as likely as those without AUP to report problems in implementing personal economic plans (X2 = 33.48, df = 1, P = 0.0000), more than 22 times as likely as those without AUP to report disciplinary problems (X2 = 30.67, df = 1, P = 0.0000), were less likely to have started a developmental project (X2 =6.85, df = 1, P = 0.009), were less likely to have saved from their income compared to respondents without AUP (X2 = 10.26, df = 1, P = 0.001), and were less satisfied with their work compared to those without AUP (X2 = 11.43, df = 4, P = 0.02). There were no statistically significant differences between Barracks I and II in relation to AUP. See Tables 1 and 2. Discussion
General considerations This paper describes the results of a study, which was carried out to assess the prevalence of alcohol use and the associated psychosocial problems in alcohol use in the Uganda Police Force (UPF). Respondents in faceto-face interview with their fellow employee (CM) in the UPF provided data on the probable negative effects of alcohol use by members of the police force. In addition to estimating the prevalence rate of harmful alcohol use to assess the public health importance of alcohol use in the target population, the study tapped the social, economic and perceived health effects of alcohol use by the respondents. Magnitude of alcohol use in the UPF The results showed that 19.2% of the respondents reported the experience of symptoms of alcohol dependence referred to in the present paper as alcohol use disorder (AUD). Twenty six percent of the respondents reported that they experienced psychosocial problems related to alcohol use, and 9.6% reported that their health was poor. The use of alcohol by the respondents concerned was associated with poor health, absenteeism and more days off work, inability to implement personal plans and projects, lack of sources of extra income, less satisfaction with work, inability to save from monthly income, and disciplinary problems. Limitation The sample size used in the present study was small due to time and financial constraints that CM faced as a student; the study was carried out as part of his training as a Psychiatric Clinical Officer. Owing to the small sample size and the nature of the study population, the results of this study may not generalize to the rest of the Uganda Police in the whole country or the general adult population in Uganda. The results of this study are limited by the failure of the study to have assessed the physical and mental health of respondents. Alcohol is frequently associated with a host of physical ailments, and it commonly coexists with psychiatric disorder. In addition alcohol dependence is an important risk factor in suicide behavior6, and this important relationship has been reported by Tusiime in the Uganda armed forces7. Modeling to define the burden of alcohol use in terms of DALYs was beyond the scope of this paper, but is recommended in future studies to highlight the economic impact of alcohol use not only in the Uganda Police Force, but in other population groups as well. It is possible that some respondents did not provide the required information on account of recall failure or for fear of victimization despite the assurances provided by the interviewer. Thus less than half of the sample size provided information on their income and savings and others were reluctant to provide data on their ethnic background. Furthermore, individuals with alcohol use problems were more inclined to use private clinics rather than the police clinic, possibly out of fear of attracting disciplinary problems related to alcohol use. Notwithstanding these shortcomings, the majority of respondents willingly provided information in the safety of their homes. The study has provided information on the prevalence of alcohol use by respondents in a nonclinical setting.Thus the study provides useful information on the role of alcohol use in the experience of social, economic, probable psychological and occupational difficulties by members of the Uganda Police Force.The results form the basis for the promotion of health and the prevention of ill health in the police force in Uganda. Comparison to other studies A Medline search of the literature identified no single study on the use of alcohol in members of the police force in Africa. Studies of communities, health care facilities and student populations indicated prevalence rates in the range of 40.3% to 91.8% (8-18) with alcohol use being the most common finding at trauma units. Sebit, Tembe Siziya et al (19) reported in 2003 the prevalence of HIV among alcohol users and non-users as 24.3% and 16.5% respectively. Several health and social problems related to alcohol use have been reported including erectile dysfunction (20), suicide attempts and crime (21, 22), multiple causes of mortality (23, 24) domestic violence (25, 26), social censure on women who use alcohol (27, 28) and psychiatric ill-health (19). In his study of secondary school students in Kampala, Basangwa in 1994 reported that alcohol was the commonest substance that 63% of the respondents used followed by cigarettes and hard drugs (29). Studies from elsewhere in Africa confirm the widespread use of alcohol by students with prevalence rates varying from 40% to 77% (14-16). Implications This study has revealed that members of the UPF experienced a variety of psychosocial and health problems related to alcohol use that ranged from 9.6% for poor health through nearly 20% for alcohol dependence to 26% impairment in psychosocial functioning. Excluding impaired psychosocial functioning, the results showed that between 1 in every 10 police officers and one in five officers were perhaps not functioning well in their jobs on account of harmful alcohol use. The results suggest serious implications for the quality of services provided by the Uganda Police. When police officers who suffer from various forms of psychosocial impairment related to alcohol use are entrusted with security issues and they are not able to perform optimally, the security of the public will be seriously undermined and the trust of the public in the force will be seriously eroded. There is therefore a need to establish measures to provide services for those affected, and a further need to establish preventative measures against alcohol dependence in the police force. However the success of such measures will require further studies to derive the needed evidence to support alcohol prevention and demand reduction policies to prevent the probable failure of policy (30). For example there will be need to study the etiological factors behind alcohol use in the UPF including personal characteristics, work environment, and rules and regulations governing the production promotion sale and timing of alcohol use. Studies in South Africa (31, 32) have suggested that the high prevalence of alcohol abuse among farm workers may be related to the policy of paying farm workers in part with alcohol rather than cash on daily basis. In the case of Uganda alcohol control measures may not work unless decisive measures are put in place to control the promotion and sale of alcohol through the print and electronic media, and introduce alternative sources of income at household level supported by measures to improve the nutritional status of household members. Declaration of interest
This paper was based on data for a dissertation written by Charles Madrama, supervised by Emilio Ovuga, for the diploma in mental health, Butabika School of Psychiatric Clinical Officers. Acknowledgements We are grateful to the Director of Medical Services in the Uganda Police Force, and the Commandant of the Police Training School for permission to carry out the study.The Uganda Police Force and the Mental Healthcare Organization of Uganda provided financial support. References:
Copyright © 2006 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs06003t2.jpg] [hs06003f2.jpg] [hs06003f1.jpg] [hs06003t1.jpg] |
| |||||||||

{kind=link}
{kind=link}