 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 6, No. 1, March, 2005, pp. 39-42 Upper gastrointestinal endoscopic findings in adolescents at Lacor hospital, Uganda Tom Richard Okello
St. Mary’s Hospital, Lacor, P.O. Box 180, Gulu (Uganda), Gulu University, Faculty of Medicine Code Number: hs06008 Abstract Background and Objectives: Fiberoptic endoscopy is a highly efficient diagnostic tool, which is now being increasingly used, in the pediatric age group.This study has been carried out to demonstrate indications for and common findings of endoscopy in children. Key words: Upper gastrointestinal tract, Endoscopy, Dyspepsia, Epigastric pain, children Introduction
Gastrointestinal diseases are a common health problem in children worldwide1. Indeed peptic ulcer disease has been reported to occur in children worldwide2 whilst disorders such as irritable bowel syndrome, dyspepsia and abdominal pain have been found to represent specific disorders in pediatrics 3. Upper GI endoscopy is the most accurate and cost effective tool available to physicians when confronted with patients with digestive complains, yet this tool is only available in a few health units in Uganda. Information on digestive disease in children is lacking in our community. It is important therefore to report on the pattern of gastrointestinal lesion in children as seen in St. Mary’s hospital, Lacor, Northern Uganda. Definition of terms: Dyspepsia: Presence of troublesome pain or discomfort
expressed as one or more of the 11 pain modalities
located in the upper part of abdomen (epigastrium) and/
or nausea, early satiety, or uncomfortable feeling of
fullness after meals.4 Objectives The objectives of the study were to determine the demographic characteristics of children who had upper GI endoscopy from Jan 2000 to June 2005, at St. Mary’s Hospital, Lacor as well as determine the indications for upper GI endoscopy in the children and determine the prevalence of upper GI lesions in the children Methods and procedures Medical records of patients who underwent upper GI endoscopy in St. Marys’ Hospital Lacor, from January 2000 to June 2005 were retrospectively reviewed. St. Marys’ Hospital, Lacor is a 483 beds rural and University Teaching hospital, located in the war torn Northern Uganda. Routine diagnostic and therapeutic endoscopies are carried out twice a week in the Hospital. Approximately 400 patients undergo upper GI endocopy per year. Gastrointestinal endoscopy at the hospital is under the department of surgery, and is performed by general surgeons with training and experience in endoscopy. In 2004, Reed et al found that surgeons are competent in esophagogastroduodenoscopies20 Under topical lidocaine, a Pentax FG-29W fiber optic Upper GI scope is passed through the mouth of a patient in left lateral position through the upper esophageal sphincter into the esophagus stomach and duodenum (upper gut). Cases, which were studied consisted of children 0-18 years old. Cases with unclear medical records or those with missing values were excluded. The following data was collected from the patient: Age, Sex, Residences, Indication for the upper GI Endoscopy, Duration of Symptoms, and Endoscopy findings.Data collected was then analyzed using SPSS Version 10, result presented in tables and Charts. Results
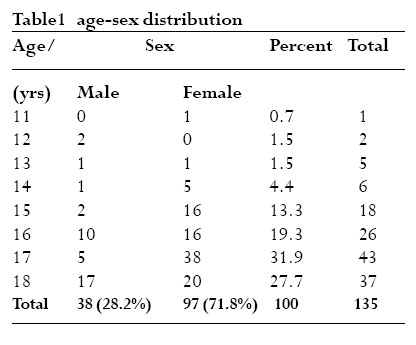
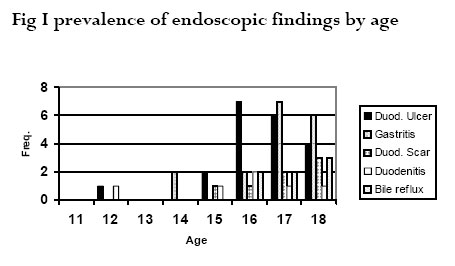
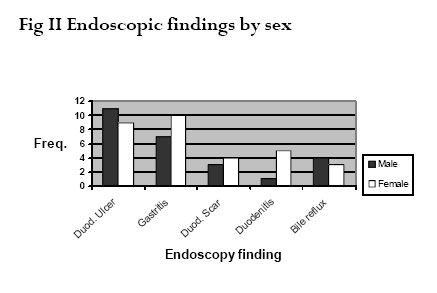
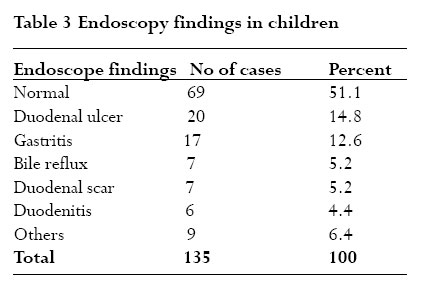
A total of 2084 patients underwent upper GI endoscopy during the period (January 2000 to June 2005), 140 (6.7%) of whom were children, of which 135(6.5%) were included in the study. The age of children who underwent upper GI endoscopy during the study period Jan 2000 to June 2005 ranged from 11 to 18 years, with a mean of 16 years (SD +/- 1.4293). The majority of the children scoped were adolescents 15 years and above (Table 1) Amongst the children scoped there were 97 females (71.8%)and 38 males (28.2%), the M:F ratio is1:2.5. However the sex difference for age was not significant (p=0.374) The three commonest indications for upper GI endoscopy in children were epigastric pain (67.7%), dyspepsia (11.9%), and hematemesis (8.9%). Miscellaneous causes (5.8%) included throat pain, chest pain, flatulence and alient body. Recurrent abdominal pain and vomiting were each responsible for 3% of the endoscopies for upper GI in children. Approximately 51% of the upper GI endoscopy done in children was negative. Of the 49% positive endoscopies, duodenal lesions were the most common 24.4%, (duodenal ulcer 14.8%, duodenal scaring 5.2% and duodenitis 4.4%) followed by gastritis (12.6%) and bile reflux (5.2%). Others (6.4%) include esophagitis, gastric polyps, fish bones, gastric ulcers, esophageal candidiasis and varicose esophagus. In Fig I, a large proportion of children with positive upper GI endoscopy findings were adolescents from the age of 15 years and above.The commonest site of GI lesions in children was duodenal followed by gastric. The mode age for children with duodenal lesions (duodenal ulcer, duodenitis, duodenal scars) was 16 years (mean 16.4 years, SD+/- 1.4149) while that for gastritis was 17 years (mean 16.8 years, SD+/-1.2690). However the difference between the mean ages for these GI lesions was not significant (P=0.552). Bile reflux was most prevalent amongst children 16-18 years of age. In Fig II, of the children scoped, a significant proportion of female children tended to have a positive endoscopy findings (P=0.000045). Generally duodenal ulcer and gastritis were the commonest positive findings in both sexes, though of the two, gastritis was more common in females and duodenal ulcer in males. Doudenitis and duodenal scarring tended to be more in the female, but bile reflux was more in male children. Discussion Gastrointestinal diseases affect children worldwide and in patients with digestive complaints, endoscopy is the gold standard and often the primary exploration 5. The indication for endoscopy in children is similar to adults 6,9. The age range was 11 to 18 years with a mean of 16 years (SD+- 1.4293) (Table 1). The majority of children endoscoped were 15 years and above and positive endoscopic findings were predominant in this same age group (Fig I). Similar age ranges were reported separately by Constantino et al in 20047 and Kawakami et al in 200416 There were 97 females (71.8%) and 38 males (28.2%) in the study, (Male: Female ratio 1:2.5) but the sex difference for age was not significant (P=0.374)*.A significant proportion of female children had positive GI endoscopic findings (P=0.000045). (Fig III). The finding of more female children attending endoscopy and more positive findings in the same sex can only be explained by the fact that female children either suffer more or have poor tolerance to GI diseases and hence tend to seek medical care at an earlier stage of their disease. Studies elsewhere have demonstrated similarly high prevalence of gastrointestinal symptoms and diseases in female children and adolescents8,17,18. The most common indications for endoscopy in children in this study were epigastric pain (67.4%), dyspepsia (11.9%), hematemesis (8.9%), abdominal pain (3.0%) and vomiting (3.0%) (Table 2).The above indications are similar to those of adults6. Many authors on childhood digestive diseases have found epigastric pain to be the most common indication for endoscopy in children16,18,19. In this study 12% of the children presented with dyspepsia, this is similar to the findings by Shah et al10 . Whilst we found hematemesis, recurrent abdominal pain and vomiting as the other indications for gastrointestinal endoscopy, other authors have reported the same in adults and children12,19. Of the 135 children studied, 51% had negative upper GI endoscopy findings (Table 3), and 49% were positive, similar to the findings of Lambert in 19995.This is important because a reliable negative finding relieves anxiety of patients and may prove cost effective by reducing drug prescription and number of consultations. Amongst the 49% positive GI endoscopy findings, the majority consisted of children aged between 15 and 18 (Fig I and II). However the most prevalent upper GI lesions in children was duodenal with a mean age of 16.4 years, (SD+/- 1.4149) and gastritis with mean age of 16.8 years, (SD+/-1.2690).The difference between these means was not significant (P=0.552). Of the Duodenal lesions, which accounted for 24.4%, duodenal ulcer was 14.8% while duodenal scarring and doudenitis were 5.2% and 4.4% respectively. (Table 3). Ogwang reported similar proportion of duodenal lesion21 in dyspeptic patients. Gastritis was found in 12.6% of the children (Table 3). The prevalence of duodenal ulcer and duodenitis in this study is similar to the 15.2% and 3% reported respectively in 2005 by Huang et al11. The findings of duodenal scar can be attributed to the sequelae of healed duodenal ulcer.Although many gastrointestinal studies in children have reported varying proportions of gastritis in 11,13,14, our finding of 12.6 % is close to the 9.3%, reported by Dhaliwal et al15. * Fisher’s exact test Conclusion In our experience, upper gastrointestinal endoscopy is a diagnostic procedure in children with gastrointestinal disorders. A large proportion of children 49% with gastrointestinal complaints have positive upper GI endoscopy. The most common indication for upper GI endoscopy in children is epigastic pain, and dyspepsia followed by hematemesis. Gastritis and duodenal ulcer are common gastrointestinal disease in children. These must be included in the differential diagnosis of upper GI pathology in symptomatic children References
Copyright © 2006 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs06008f1.jpg] [hs06008t3.jpg] [hs06008t2.jpg] [hs06008t1.jpg] [hs06008f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}