 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 6, No. 1, March, 2005, pp. 55-58 Neurologic infections in a Nigerian university teaching hospital Emmanuel N Chapp-Jumbo Department of Medicine, College of Health Sciences, University of Port
Harcourt & University of Port Harcourt Teaching Hospital (UPTH), Port
Harcourt, Rivers State, Nigeria Code Number: hs06012 Abstract Background: Neurologic infections are an important cause of morbidity and mortality especially worldwide but much more in the African continent.The frequency of the different types of neurologic infections and their mortality in this part of Nigeria is not known. Key words: neurologic infections, hospital admissions Introduction Infections involving the central nervous system (CNS) are important causes of mortality and morbidity in many African countries 1 and thus arouse tremendous anxiety in both physicians and patients. World-wide, the scenario of CNS infections is changing mainly due to the increase in immuno-compromised patients (due to AIDS, prolonged survival of patient with malignancies and organ transplantation), increase in international travels allowing rapid transmission of infectious agents and widespread use of antibiotics creating the emergence of resistant organisms. The pattern of these infections in Rivers State, Nigeria, is not known. This study was undertaken to determine the types, frequency and mortality associated with these infections. It involved a retrospective review of patients admitted into the medical wards of the University of Port Harcourt Teaching Hospital (UPTH), Port Harcourt, Rivers State, Nigeria2 over a ten-year period between April 1993 and March 2003 diagnosed with neurologic infections. The UPTH is a 484-bed tertiary hospital and the main referral center in Rivers State and other neighboring states in Nigeria, and has an annual admission rate of 10,000 . Methods The case notes of all admissions into the medical wards of UPTH, Port Harcourt between April 1993 and March 2003 were collected from the medical wards and the medical records department of the hospital. Admission into the medical wards is from age of 14 years, so patients below this were not included. Figures of hospital admissions and deaths during the same period were also collected from the medical records department. Cases admitted with CNS infections were extracted for the study. The following data were extracted from case notes – age, sex, date of admission, diagnosis, date of discharge and outcome (whether discharged, died, discharged against medical advice (DAMA) or absconded, or transferred to other tertiary centers or departments). Sixty seven case notes with defective data were excluded. All diagnoses were made by a consultant physician. These data were then analyzed. CNS infections identified included: bacterial meningitis and tuberculous meningitis (TBM) whose diagnoses were based on a typical history and physical findings of various combinations of headache, fever, meningism, clouded consciousness and signs of raised intracranial pressure and CSF findings. Pott’s disease with cord compression diagnosed from the history and physical findings of combinations of past tuberculosis, signs of cord compression and typical chest and spine x-ray findings, elevated ESR and response to treatment.Viral meningoencephalitis including rabies was diagnosed from the history, physical finding and CSF studies. Tetanus and cavernous sinus thrombosis (CST) were diagnosed mainly from clinical findings. Cerebral malaria was diagnosed from the history, physical examination, CSF findings and blood smear. Lumbar puncture (LP) was done in 11 (81.2%) of 136 cases of meningitis, 10 (52.6%) of 19 cases of tuberculous meningitis, 24 (88.9%) of 27 cases of viral encephalitis and the 2 cases of cerebral malaria. The laboratory tests employed depended on the suspected CNS infection; availability and affordability so varied among patients and period. These included complete blood count, peripheral blood smear, ESR, serum biochemistry, x-rays, serological tests and microbiology. None of the patients had a CT scan as this became only recently available, and even then the cost was prohibitive for most patients..Viral studies were not done due to lack of facilities. HIV screening using the ELISA method was documented in only 12 cases (meningitis 6, viral encephalitis 2,TB meningitis 3, and tetanus 1).There was no autopsy report documented on the case notes of the deceased. Results
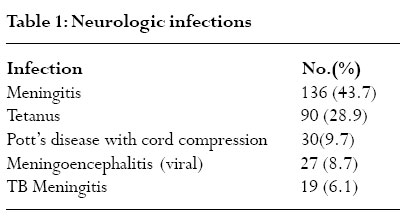
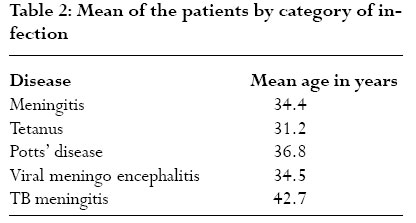
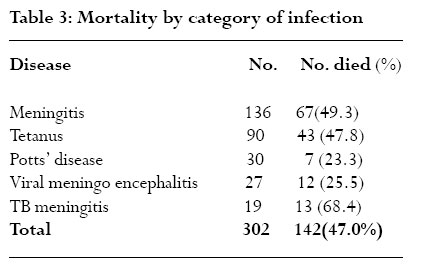
The number of cases admitted with neurologic diseases during the study period was 1395. Of these, 311 (22.3%) had neurologic infections. Hospital and medical admissions during the same period were 92,455 and 4,213 respectively. The male to female ratio and mean age of patients with neurologic infections were 1.7:1 and 34.1 years respectively. The frequency distribution of sex, types of infection, and outcome of patients are shown in Tables 1, 2 and 3 respectively.The mean duration of hospitalization of cases with neurologic infections was 14 days. During the period under review, the number of hospital deaths was 13933, medical deaths 1759 and neurologic deaths 509 (including 147 with infections). Viral infections affecting the CNS was documented in 27 cases representing 1.9%, 0.6% and 0.03% of neurologic, medical and hospital admissions respectively. Males were more affected and the mean age of affected individuals was 34.5 years.The case fatality rate was high (44.4%), representing 2.4%. 0.7% and 0.09% of neurologic, medical and hospital deaths respectively Discussion The diagnoses of most of the cases were largely clinical. The study showed that during the period under review, infections of the nervous system were a common cause of admission in the hospital.The commonest infections, were meningitis, tetanus, Pott’s disease with cord compression, viral meningoencephalitis, and tuberculous meningitis. Less common infections included rabies, cerebral malaria, cavernous sinus thrombosis and cerebral abscess.A similar study in Madagascar3 reported a lower CNS infection rate with neurocysticercosis topping the list of CNS infections. Bacterial meningitis was the commonest neurologic infection in the current study representing 43.7% of neurologic infections. Almost half (49.3%) the patients died.. This mortality rate was very high compared with that reported by other workers.4,5 The cause of this high mortality may be related to late presentation of the patients, level of consciousness, cormobidity such as pneumonia, diabetes, HIV infection and resistance to penicillin and chloramphenicol, the most commonly used antibiotics on the patients. Third generation cephalosporin such as cefotaxime or ceftriaxone the recommended6 first line of treatment in most patients, are usually unaffordable by the majority of patients with meningitis in this hospital. Most of the adults with bacterial meningitis present to clinicians with little experience with the management of meningitis thus resulting in delay with referrals to centers with specialists or experienced physicians. Early recognition, stabilization and institution of specific therapeutic measures are crucial to patient outcome with bacterial meningitis. Tetanus: This was the second most common neurologic infection requiring admission in this study. It was responsible for 28.9% of cases admitted with neurologic infections. Case fatality rate (47%) was high consistent with findings of other studies in developing countries. 7,8 The high mortality rate was due to respiratory failure occasioned by hypoxia and airway obstruction, aspiration hypoventilation, pneumonia and respiratory arrest. Intensive care was rarely utilized because of limited facilities. Other contributing factors were low immunization rates of the population and late presentation of cases. Pott’s disease with cord compression: All patients were treated with anti-tuberculous drugs only without any surgical intervention because of lack of neurosurgical facilities locally and the unaffordable cost of referral. This may account for the high mortality recorded. Decompressive surgery plus anti-TB chemotherapy remains the best mode of therapy for Pott’s disease.The major causes of death in the UPTH, PH cases were complicating septicemia from infected decubitus ulcers or urinary tract infections and pulmonary embolism from prolonged immobilization. A low mortality of 2% was reported in a Turkish study 9. In that study, it was concluded that the neurological involvement due to Pott’s disease is relatively benign if urgent decompression is performed at the onset of the disease. Viral meningoencephalitis: The mean duration of hospitalization was 9.7 days. Concomitant infection with the HIV virus, secondary bacterial infection and late presentation were factors contributing to the high mortality rate. Tuberculous meningitis: Nineteen cases (19) cases of TBM, representing 1.4%, 0.5% and 0.02% of neurologic, medical and hospital admissions respectively were identified. TBM had the highest case fatality rate of all neurologic infections with 13 (68.4%) deaths, comparable to that reported by Karstaedt et al 10 in South Africa.This mortality represented 2.6%, 0.7% and 0.1% of neurologic, medical and hospital deaths respectively. Mortality was related to the patient’s level of consciousness on admission, as over half of those admitted with altered level of consciousness, died. Concomitant HIV infection was also another factor producing a dismal prognosis in these patients. The less frequent neurologic infections encountered in this study included rabies (1.3%), cerebral malaria (0.6%), cavernous sinus thrombosis (0.6%) and cerebral abscess (0.3%). All the cases of rabies were from dog bites; three of who died and one was discharged against medical advice. Cerebral malaria is mostly observed in children because of their low immunity to the parasite, hence the low frequency in the study population. The cases of cavernous sinus thromboses and cerebral abscess were the result of complications arising from paranasal infections and chronic otitis media respectively. 50% of the cases with HIV infection died during the period of admission. The low rate of screening for HIV in suspected cases was mainly attributable to refusal to give consent and cost of screening. None of the positive cases received anti-retroviral treatment. Conclusion Neurologic infections are an important cause of morbidity and mortality in neurologic practice in this environment. The high mortality rates were largely due to late presentation to specialized care. Therefore, cases presenting with suspicious neurologic infections to lessexperienced health workers should be referred immediately to centers where specialized care can be instituted early.The use of penicillin and chloramphenicol for the treatment of bacterial meningitis needs review in light of increasing resistance of the organisms to these antibiotics. Acknowledgements
To the Almighty God for His mercies and Guidance; to the Matron and nurses of the Dept of Medicine and the staff of the Medical Records Dept of UPTH, Port Harcourt for tassistance in the collection of the data; to my family for ensuring a conducive study environment. References
Copyright © 2006 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs06012t1.jpg] [hs06012t2.jpg] [hs06012t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}