 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
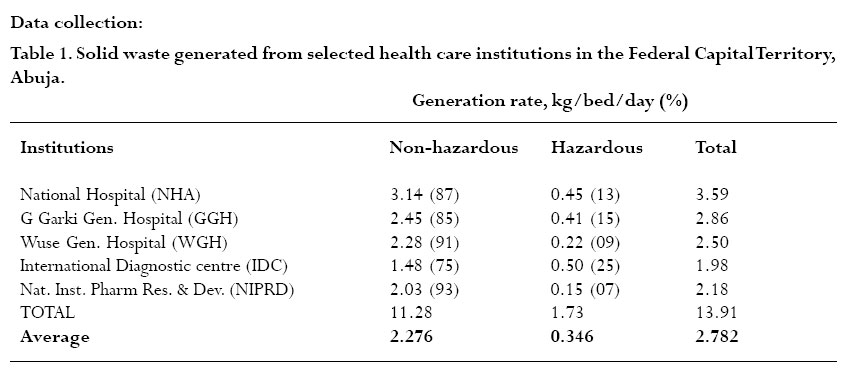
African Health Sciences, Vol. 6, No. 1, March, 2005, pp. 58-63 Characterization and management of solid medical wastes in the Federal Capital Territory,Abuja Nigeria B. E. Bassey1, M.O. Benka-Coker2, H.S.A Aluyi2 Department of Medical Laboratory Services General Hospital, Wuse, Garki-Abuja, Nigeria. Department of Microbiology, Faculty of science,University of Benin, Edo State, Nigeria. Code Number: hs06013 Abstract Background: Medical establishment such as hospitals and research institutes generate sizable amount of hazardous waste. Health care workers, patients are at risk of acquiring infection from sharps and contamination of environment with multiple drug resistant microorganisms if wastes are not properly managed. Key words: characterization, medical waste, management, hazardous, Nigeria. Introduction Healthcare institutions are service-oriented establishments that provide medical care facilities comprising of observational, diagnostic, research and therapeutic and rehabilitative services. These facilities are among the largest generators of solid waste on a per capita basis 1 In Nigeria, healthcare waste falls under the category of infectious waste 2. Within this category are culture and stock of infectious agents, pathological waste, waste from surgery or autopsy that were in contact with infectious agents, sharps (hypodermic needles, syringes, scalpel blades), waste from human blood and products of blood and laboratory waste. Other hazardous materials used by healthcare institutions that become part of their waste streams include chemotherapeutic agents, antineoplastic chemicals, solvent, formaldehydes, photographic chemicals, radio nuclides, mercury, anesthetic gases and other toxic, corrosive and miscellaneous chemicals. Additional wastes such as incinerator exhaust, laundry– related and kitchen wastes are also generated 3 Healthcare sewage usually contains a variety of pollution indicators and pathogenic bacterial species that come from patients. Variation and concentration of these bacteria depend mostly on two factors: the amount of antibiotics, detergents and radioactive substances that may be disposed in sewage and the environmental conditions such as temperature, humidity and nutritional state 4. The connection of healthcare waste effluent with municipal sewage network creates public health risk and imbalance in the microbial communities in the sewage system, which in turn affects biological treatment process 5. High numbers of total coliforms, faecal coliforms and streptococci, staphylococci, Klebsiella species and fluorescent Pseudomonas species were reported in sewage for Baghdad City hospitals 4. Waste management, as an important part of environmental hygiene needs to be integrated with environmental planning and policies. Improper collection, storage, treatment and disposal can lead to serious environmental damages of various kinds. Some of the health problems associated with improper collection; treatment and disposal of health care wastes include typhoid fever, cholera, skin disease malaria, intestinal parasitosis, and hepatitis6,7. Burning and incineration of medical and municipal waste have been linked to severe public health threat and pollution resulting in the release of toxic dioxin as well as mercury and other toxic substances. These substances produce a remarkable variety of adverse affects in humans at extremely low doses 8. Putrefaction occurs in portions of refuse, which have not been fully burnt and add to air pollution through foul smells. Sanitary landfill can lead to pollution of ground water if not properly managed. The microbiology of medical waste and their biodegradation potentials would assist in the biological treatment of these wastes. The objective of this study was to characterize types and evaluate waste disposal techniques employed in the management of solid medical wastes generated in the five selected hospitals in the Federal Capital Territory,Abuja, Materials and methods Study area: This study was conducted in five health care institutions, selected based on size, location and service utilization in the Federal Capital Territory, Abuja, the administrative capital of Nigeria, which predominantly is made up of civil servants, with an estimated population of 1.3 million inhabitants 9 Sources of sample: Medical wastes were collected from the following sites within the Federal Capital Territory,Abuja. National Hospital, the largest and a five star hospital in Nigeria, Garki General Hospital and Wuse General Hospitals, which serve over 80% of the population, Abuja International Diagnostic Center, a first line privately owned hospital and National Institute for Pharmaceutical Research and Development. Data collection:
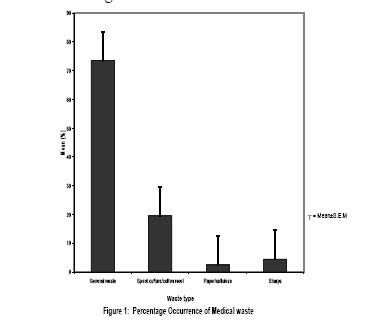
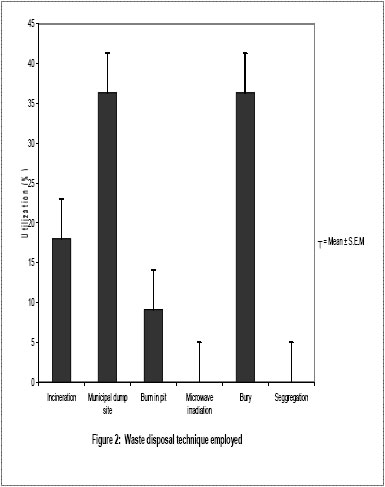
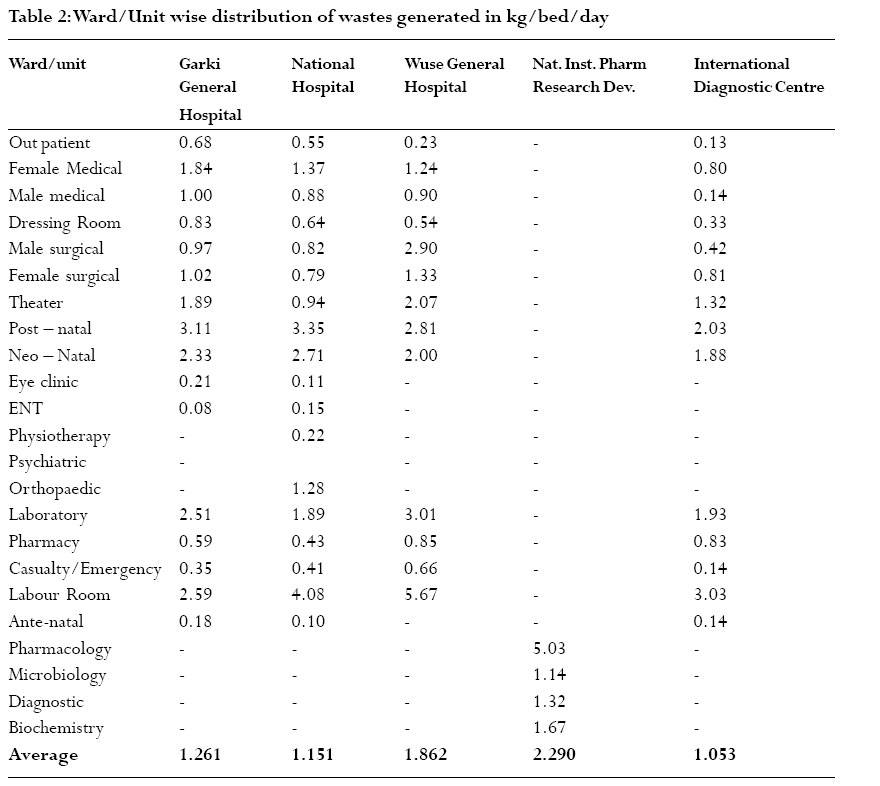
Three instruments, questionnaire administration, indepth interview and participant observation strategy / discussion were adopted in this study. The questionnaires were administered to the hospital administrators.The existing waste management policy with respect to collection, storage, transportation and final disposal were evaluated. Information regarding staff strength, services available, wards, units, number of beds, average bed occupancy rate, and profile of waste handlers were collected through administered questionnaires; others are quantities and waste type produced. The discussion was organized to obtain additional information from respondents and heads of units and wards as well as use the responses to validate some of the results from the questionnaire and in-depth interview. In total, 5 administrators, 40 unit/ward heads and 10 cleaners were interviewed. The Incinerator Institute of America method was used in the analysis of waste samples 10. The solid medical waste generated in each ward or unit of the hospitals selected for this study were collected in labeled polythene leak-proof bags as appropriate. Twenty four (24) hours solid waste was collected in labeled polythene bags till the end of the 21-day monitoring exercise. The composition of dhe wastes from each hospital was estimated by sorting into four main categories namely: paper/cellulose/swabs/gauze/pads, sharps, general and infectious wastes. The sorted wastes were then weighed using top loading balance MB640 and characterized into cellulose, general, infectious wastes or sharp instruments and were treated and disposed of appropriately. Results Figures showing variation in the volume of waste generated from each health care institution and solid wastes generation rate per kg/bed/day from the five selected institutions in the Federal Capital Territory,Abuja are presented on Table I. It is apparent that average waste generation rate per bed per day is 2.782 kg/bed/day. Generation rate (Total weight) per health institution is as follows: National Hospital, 3.59kg; Garki General Hospital, 2.86kg;Wuse General Hospital, 2.50kg; International Diagnostic Center, 1.98kg and National Institute for Pharmaceutical Research and Development, 2.18kg. Non–hazardous waste ranged from 1.48kg/bed/day at International Diagnostic Center (IDC) to 3.14kg/bed/day at National Hospital, while hazardous waste ranged from 0.15kg at National institute for pharmaceutical research and development to 0.50kg/bed/day at IDC. The average of hazardous and non hazardous waste generated from the five health care institutions amounted to 0.346kg and 2.276kg respectively. There was a significant variation in the volume of hazardous and nonhazardous wastes generated at P=0.05. General waste had a mean percentage of 73.5%; infectious waste (spent cultures/ swabs/cotton wool), 19.5% and paper/cellulose 2.5%, Sharps (needles, blades, syringes, scalpel, broken glass, and nails), 4.5% as indicated in Figure 1. Results obtained indicated that waste disposal techniques employed by the selected health institutions in the management of solid waste were incineration, burial in the hospital premises, burning in open pits, and disposal of their waste into the municipal dumpsite, microwave irradiation and segregation. From the results 18% of health care institutions surveyed incinerated their solid wastes in locally built bricks incinerators without adequate protection to the environment. 36.3% of the institutions simply disposed off their wastes into the Abuja municipal dumpsite, these wastes were found not to be treated before dumping into the dustbin at the dumpsite. 9.1% buried their solid wastes while another 36.3% had their waste burnt off in open pits. Waste segregation and microwave irradiation techniques were never employed by any of the selected health care institutions surveyed (Figure 2). Results obtained from investigation on generation rate per/bed/day are presented on Table II. In Garki General Hospital generation rate ranges from 0.08kg/bed/day in Ear Nose and throat (ENT) unit to 3.11kg/bed/day in post natal unit. In the National Institute for Pharmaceutical Research and Development, Idu, waste generation rate ranges from 1.14kg in microbiology unit to 5.03kg in the Pharmacology unit. Generation rate in National Hospital ranges from 0.10kg/ bed/day in antenatal unit to 4.08kg/bed/day in the labor ward. In Wuse General Hospital generation rate ranges from 0.23kg/bed/day in the outpatient unit to 5.67kg/ bed/day in the labor unit.At the International diagnostic center generation rate ranges from 0.13kg/bed/day in outpatient unit to 3.03kg/bed/day in the labor ward. Discussion Medical waste management has received very little attention in waste management process in Nigeria. Neither the government nor hospital authorities pay proper attention to its management. Unwholesome waste disposal by many hospitals, clinics and health centers in Abuja pose serious health hazard to the city dwellers in general and people living within the vicinity of the health care institutions in particular. Almost all the health care institutions surveyed dispose every kind of waste generated into municipal dumpsites without pre-treatment, leading to an unhealthy and hazardous environment around the health institutions, affecting patients and staff. Scavengers who collect waste from dustbins are at risk of injury from sharp instruments and direct contact with infectious materials. Liquid medical wastes are disposed directly into the municipal sewer system by all the institutions surveyed. Direct disposal of faces and urine of infectious patients in municipal sewer system may cause outbreak of epidemic diseases 11,15. The scavengers that engage in recycling operations are unaware of the harmful consequences of exposure to contaminate and hazardous waste 12. Adjacent to the main gate at the Wuse General Hospital is an open dump, creating an eye sore to the inhabitants of the fairly-densely populated commercial area and are exposed to adverse effect of this action. The situation at the Garki General Hospital is hardly better. The cleaners collect wastes produced in each ward in plastic buckets and dump them behind the hospital.The wastes are burnt here without regards to the effect of the action on the environment. Waste management options employed by the surveyed health care institutions included disposing their waste into municipal dumpsites, burial and burning. 18% of the health institutions surveyed incinerate their wastes in locally built brick incinerators without safety devices. This may enhance the deposition of heavier particles of the flue gases in the conical portion, the exhaust gas being later discharged into the atmosphere with very serious health implications, while multidrug resistant microbes are plough back into the environment15. 36.3% of wastes generated are disposed into the municipal dumpsites. This over-flow the bins and litter the environment as waste collectors stay away for weeks without attending to the wastes produced. 9.1% of the institutions bury their waste in the hospital premises. This has the potential to pollute ground water, which may therefore expose the population to health hazards. While another 36.3% burnt waste produced in open pits leading to the production and release of smoke and dangerous gases into the atmosphere. These practices expose the people to serious health risk.This study also revealed that none of the health institutions surveyed treated its wastes before disposing of it into the municipal dumpsites. Microwave irradiation and waste segregation were not practiced. Waste segregation is an important treatment option in the management of hazardous wastes. This procedure not being practiced by any of the selected institutions may be due to lack of trained waste managers in the healthcare institutions studied. Generally, treatment options employed by the surveyed healthcare institutions fall short of the World Health Organization standards 13. The average healthcare waste generation rates were in the range of 1.053kg/bed/day to 2.290kg/bed/day in Abuja. Similar ranges have been reported for Dhaka City (0.8kg/bed/day to 1.67 kg/bed/day),Amsterdam (2.7kg/ bed/day) and Paris [2.5kg/bed/day10. However higher ranges 1.0kg/bed/day to 4.5kg/bed/day were documented for New York City,Chile,Brazil,Argentina,and Venezuela 5 and in Ibadan here in Nigeria (1.0kg/bed/day to 1.50kg/bed/ day)1. The average generation rates per bed per day are lowest at the ENT unit of the Garki General Hospital (0.08kg/ bed/day) and highest at the labour ward of Wuse General Hospital (57.7kg/bed/day). The considerable smaller quantities of solid wastes generated at the ENT clinic is not surprising given the fact that the kind of therapy usually prescribed here does not lead to generation of much wastes. The variation in the waste generation rate from one ward or unit to another within each health institution obtained is as expected, since this depended on the nature of activities in a specific ward or unit 5. Majority of the patients attended to at the injection rooms were out patients, generating typically light weight wastes such as needles, syringes; whereas relatively heavy and moisturized wastes such as soaked swabs, gauze, pads, disposable napkins were generated by the largely in-patients at the labor ward. Similar reason accounts for the high value of waste generation rate at the Neonatal and Postnatal wards of the institutions surveyed. Similarly, Coker et al reported the generation of heavy and moisturized wastes in Ibadan, Nigeria 1. This study revealed that 26.5 per cent of the total wastes generated from the five selected health institutions were hazardous, and therefore required special attention for their disposal. Rahman 12,14 reported comparable values, for Denmark (25 %) and for NewYork City (28 %). However in Netherlands, Sweden, Dhaka City and Germany much lower values (5.0%, 9.0%, 15.5%, and 14.0% respectively were reported 12. This variation may be due to differing living habits and standards, availability of different treatment facilities, geographical location and perhaps the ways in which solid wastes are segregated and categorized in the different countries 12. Conclusion This pilot study in the Federal Capital Territory, Abuja has shown that very little has been done on medical waste management in Nigeria. It is therefore recommended that the ministries of Environment and Health must put place a legislation that will regulate medical waste generation and management and also adopt a multidisciplinary approach to medical waste management in Nigeria. Acknowledgements We gratefully acknowledge the skilled technical assistance of Prof. N. O. Eghafona, Dr. Ibrahim Kolo, Mrs. Gloria Fojule, and the use of National, Gwagwalada Specialist,Wuse and Garki Hospitals, also International Diagnostic Center and National Institute for Pharmaceutical Research and Development facilities for data and study, which resulted in this paper. References
Copyright © 2006 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs06013f1.jpg] [hs06013f2.jpg] [hs06013t1.jpg] [hs06013t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}