 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 6, No. 2, June, 2006, pp. 76-80 Non-neoplastic diseases of the cervix in Nigerians : A histopathological study Olutoyin. G. Omoniyi-Esan,* Steven.A. Osasan, Olusegun. S. Ojo Department of Morbid Anatomy and Forensic Medicine, Faculty of Basic Medical
Sciences, College of Health Sciences, Obafemi
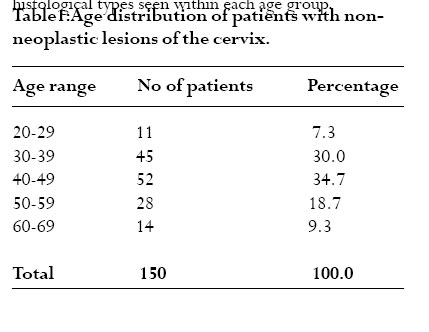
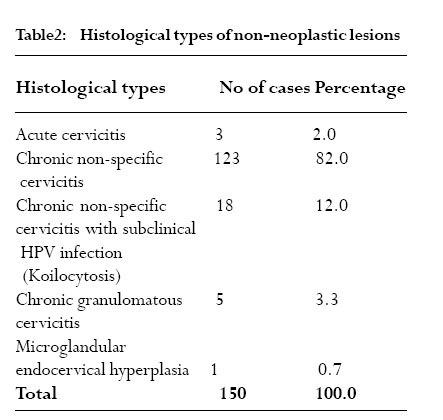
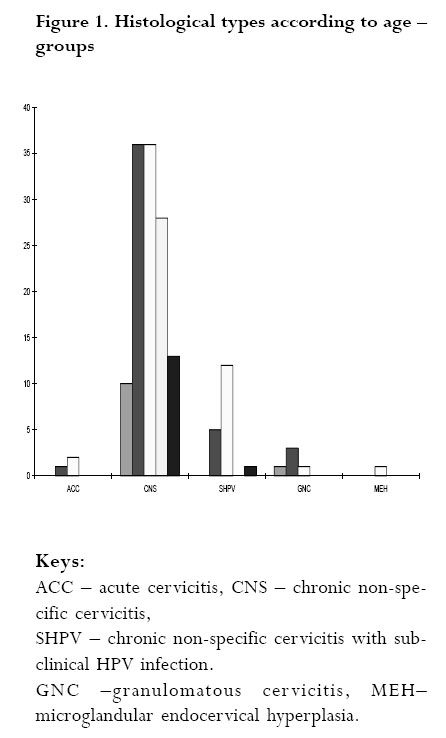
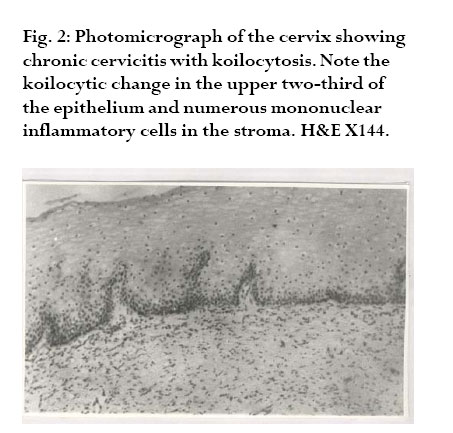
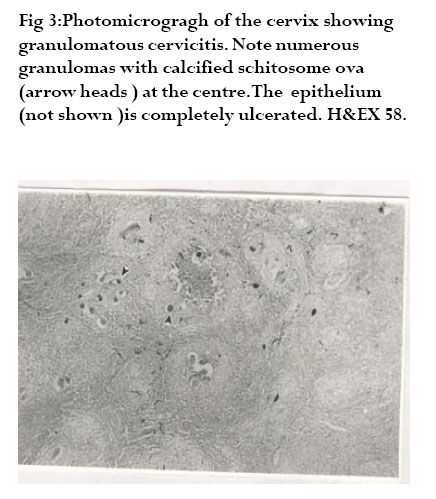
Awolowo University Ile-Ife, Nigeria Code Number: hs06018 Abstract Background: Diseases of the cervix are common in young sexually active women. Non-neoplastic diseases are predominantly inflammatory and are common but there are a few publications on the subject compared to neoplastic diseases of the cervix. Key words: Non-neoplastic, Cervix, Disease. Introduction Diseases of the cervix are common in young sexually active women.1 Non-neoplastic diseases of the cervix are predominantly inflammatory in nature. Infections and inflammatory lesions of the cervix are common but there is a dearth of literature on the histological characteristics of these lesions. Cervical inflammation may be acute, chronic or active (acute-on-chronic). Each of these may be from non-infective and infective causes. Non infective cervicitis is most often chemical in nature. Common causes include chemical irritations secondary to douching or local trauma produced by foreign bodies including tampons, diaphragms, pessaries and intrauterine contraceptive devices.1 The aetiology of infective cervicitis is variable and consists commonly of sexually-transmitted diseases, Staphylococcus aureus, endogenous vaginal aerobes and anaerobes among others. Although frequently encountered clinically, there are few reports on the histopathology of these lesions. This is not unconnected to the fact that most of these infections are amenable to antimicrobial agents and do not require cervical surgical biopsy for diagnosis. Chronic Granulomatous inflammation also affects the cervix. Worldwide, the commonest cause is tuberculosis2 ,3 Other less frequent causes include schistosomiasis, amoebiasis4 , enterobiasis, actinomycosis, lymphogranuloma venerum (LGV) and syphilis. Tuberculous cervicitis usually arises secondary to disseminated tuberculosis and usually produces ulcerative lesion and sometimes hypertrophic lesions which may grossly simulate carcinoma of the cervix5 . In a study by Chakraborty et al, hypertrophic lesions were found to be predominant and contain abundant acid fast bacilli than the ulcerative lesions6 .The occurrence of concomitant tuberculous cervicitis and carcinoma has also been reported.7 Schistosomiasis is endemic in the tropics. In severe infections, calcified ova of Schistosoma may be seen in the genital tract. Cervical involvement may be present as polypoid or nodular masses8 . Viruses especially Human papilloma virus and Herpes simplex virus commonly infect the cervix and are strongly associated with carcinoma of the cervix9 10 Other lesions seen in the cervix include tunnel cluster, mesonephric hyperplasia, endometriosis and microglandular endocervical hyperplasia.11 , 12 . These lesions may be misinterpreted as malignant. Familiarity with their histopathological features is essential in their recognition and appropriate management. The aim of this study is make information available on non-neoplastic diseases of the cervix from our routine histopathological practice. METHODS The register of the histopathology department of the Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife from the year 1990-1999 (10 years) were studied for all cervical biopsies. The original requests cards were retrieved and information such as age and histopathological diagnosis were extracted. All non-neoplastic cervical biopsies specimens were assessed for the study. In our histopathology laboratory at Ile-Ife, cervical surgical specimens as other specimens are routinely formalin fixed, paraffin-embedded, and cut at 2-3mm. All such sections are routinely stained with haematoxylin and eosin stains. Vital statistical data like age and histopathological diagnosis were noted. All the slides of the patients with non-neoplastic cervical pathology were retrieved and examined. Where not available, fresh sections were cut and stained with routine haematoxylin and eosin stains. The biopsies were classified into acute cervicitis, chronic non-specific cervicitis ,chronic cervicitis with koilocytic change, granulomatous cervicitis, and miscellaneous lesions (e.g microglandular hyperplasia, endometriosis, turnell clusters .1 Data were processed using SPSS version 10.0. Descriptive methods such as tables and figures were used for presentation of the results. RESULTS Between the period January 1990 and December 1999, a total of four hundred and twentytwo (422) cervical surgical biopsies were received in the Department of Morbid Anatomy and Forensic Medicine, Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife. Four hundred cases met the criteria for the study.This constituted 4.4% of surgical pathology cases from females and 3% of total surgical pathology specimens during the study period. Out of these , one hundred and fifty ( 150 cases ) 37.5% were non-neoplastic lesions. The age distribution of the patients is depicted in tables 1. The age range was 20-69 years while the peak age incidence was 40-49 years with 52 cases (34.7%). This is also the peak age for all the histological types.This is followed by age group 30-39 years with 45 cases (30.0%), 50-59 years with 28cases (18.7%). The least number of patients is seen in age group 20-29 years with only 11 cases (7.3%). It is noteworthy to note that majority of non-neoplastic lesions (83.4%) occurred in age group 30-59 years. The histological types of non-neoplastic lesions are shown in tables 2 and Fig. 1 shows the histological types seen within each age group. Chronic non-specific cervicitis was the commonest non-neoplastic lesion and constituted 123 cases (82.0%). It was also seen in all age groups. Eighteen cases (12.0%) were chronic cervicitis with koilocytic change pathognomonic of HPV infection. Two third of these (12cases) occur within 40-49years. Five cases (3.3%) of chronic granulomatous cervicitis were seen, three of which were schistosomal cervicitis with numerous calcified ova. One of the cases was that of caseating granulomas suggestive of tuberculosis and the other has stellate abscess with numerous neutrophils suggestive of actinomycosis. There were only three cases with features of acute cervicitis. There was a case of microglandular endocervical hyperplasia.The complete spectrum of the non-neoplastic diseases occurs in the age group 40-49years. Majority of women within the age group 50-69years have chronic non-specific cervicitis. Chronic non-specific cervicitis was the commonest non-neoplastic lesion and constituted 123 cases (82.0%). It was also seen in all age groups. Eighteen cases (12.0%) were chronic cervicitis with koilocytic change pathognomonic of HPV infection. Two third of these (12cases) occur within 40-49 years. Five cases (3.3%) of chronic granulomatous cervicitis were seen, three of which were schistosomal cervicitis with numerous calcified ova. One of the cases was that of caseating granulomas suggestive of tuberculosis and the other has stellate abscess with numerous neutrophils suggestive of actinomycosis. There were only three cases with features of acute cervicitis. There was a case of microglandular endocervical hyperplasia.The complete spectrum of the non-neoplastic diseases occurs in the age group 40-49years. Majority of women within the age group 50-69years have chronic non-specific cervicitis. DISCUSSION Chronic non-specific cervicitis constituted 82.0% of all non-neoplastic lesions. This is not surprising because it is a frequently encountered condition both clinically and in histopathological specimens2. True chronic cervicitis is diagnosed histologically by the presence of a heavy mixed chronic inflammatory cell infiltrates – lymphocytes, plasma cells and histiocytes. This study showed that chronic non-specific cervicitis occurs in all age groups in our women between 2069years. Though, it is said to be rare before menarche or after menopause2, it is the main non-neoplastic lesion seen in the menopausal women in this study.This may be due to the fact that most of these women are still sexually active though menopausal. Infection of the female genital tract of which the cervix is the “gate-way” not only predisposes women to tubal infertility but also to the risk of ectopic pregnancy 13,14 . There are very few reports describing the histopathology of chronic cervicitis. Most of the studies available are on cytological and microbiological diagnosis1 ,2,3, ,4 ,5 Chlamydia trachomatis infection is the most prevalent sexually transmitted disease in developed countries and appears to be equally prevalent in developing countries. The prevalence in Gambia is 6.9%16, Ghana 7.7%17 and Kenya 10.0%18 in women attending antenatal clinics13,6 In Nigeria, a prevalence of 10.5% was reported among sexually active adolescent girls7 . Chlamydia cervicitis is significantly associated with cervical ectropion8,9 . The histopathological hallmarks of infection with C. trachomatis are subepithelial lymphoid follicles, fibrosis and scarring. Kiviat et al documented well-formed lymphoid follicles with germinal centres in 67% of culture-proven infection with C. trachomatis 10 None of the cases seen in this series has any of these features. Patients with chronic non-specific cervicitis usually have mixed infiltrates of plasma cells, histiocytes, lymphocytes and occasional neutrophils. These histological features are present in our patients. Chronic granulomatous infections are very common in the tropics. In severe infection there may be involvement of the cervix. Schistosomiasis and tuberculosis are frequently encountered. Schistosomiasis of the cervix caused by S. mansoni is very common in Egypt, South America, Puerto Rico and several Asian countries1. Many cases of cervical schistosomiasis are associated with urinary schistosomiasis. It may also be associated with extensive pseudo-epitheliomatous hyperplasia of cervical squamous epithelium. Association with carcinoma of the cervix has also been reported1 . The cases seen in this study had erosion of the ectocervix Genital tract tuberculosis in order of frequency affects more commonly the fallopian tubes, the corpus, ovary and occasionally the cervix. The incidence of cervical tuberculosis in the general population is 2-6%5. Viral cervicitis is very important clinically. Over the years there has been increasing detection of subclinical HPV infection cytologically and histologically. The hallmark of infection with HPV is koilocytic change in the epithelial cells, which correlates well with HPV nucleic acid by in-situ hybridisation9. In this series 18 cases (12.0%) of the chronic cervicitis showed koilocytic atypia ( sub-clinical HPV infection). A higher value of 37.0% of koilocytic atypia was reported in cytologically screened dysplastic smears in Ibadan15. Two-third of the cases occur within 4049years.This is also the peak age incidence for carcinoma of the cervix in our environment24. High grade HPV (serotype 16 and 18) is strongly associated with cervical cancer25,26. Infection with HPV is thought to be the initiating event; other factors like co-existing microbial infection and cigarette smoking also contribute to cervical carcinogenesis. Only 2.0% cases of acute cervicitis were seen. Patients with acute cervicitis usually present with acute discomfort, purulent cervical discharge and are treated medically. Most of the patients do not require cervical biopsy.Acute cervicitis may follow trauma due to parturition or abortion, inappropriate use of tampons or infection by pathogenic agents.2 T. vaginalis infection of the cervix produces acute cervicitis. The histological features of which include spongiosis, ulceration and necrosis of diffuse punctuated erythema. Cytologically T. vaginalis infection can easily be recognized by the presence of ovoid trichomonal organism and/or prominent perinuclear halo.15 In conclusion, the peak age incidence of 40-49 years shows that women in this age group are prone to cervical lesions. All the histological types were also found within this age range. Chronic non-specific cervicitis is the most common non-neoplastic cervical lesion and occurs in all age groups of women studied. This shows that the burden of non-neoplastic cervical lesions in the women of reproductive age is infective in origin with its attending sequelae. We recommend routine pap smear test in this group of patients especially, as a way of reducing the occurrence of carcinoma of the cervix. References
Copyright © 2006 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs06018t2.jpg] [hs06018t1.jpg] [hs06018f1.jpg] [hs06018f3.jpg] [hs06018f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}