 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 6, No. 2, June, 2006, pp. 93-97 Cholera in endemic districts in Uganda during El Niño rains: 2002 –2003 Scholastica O. Alajo 2, Jessica Nakavuma 1, Joseph Erume 1 1 Faculty of Veterinary Medicine, Makerere University, P. O. Box 7062, Kampala, Uganda. 2 Central Public Health Laboratories, Ministry of Health, P. O. Box 16341,Wandegeya - Kampala, Uganda. Code Number: hs06022 Abstract Background: El Niño phenomenon causing increased rainfall and
flooding has been linked to flare ups and emergence of several disease outbreaks
including cholera.The latter has been reported in many districts in Uganda
in recent years.Therefore an understanding of factors influencing its pattern
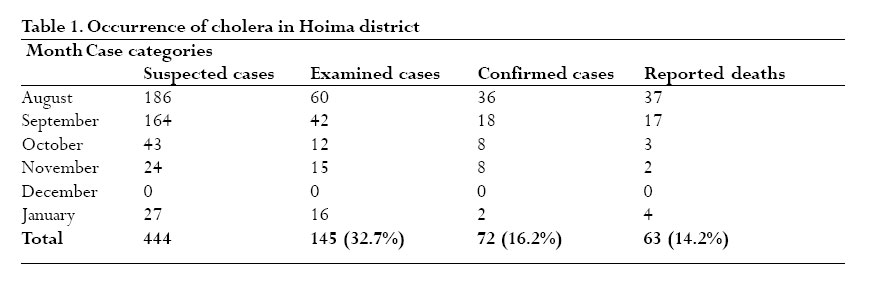
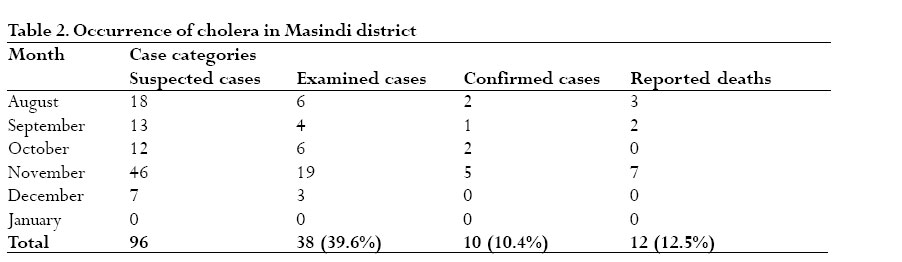
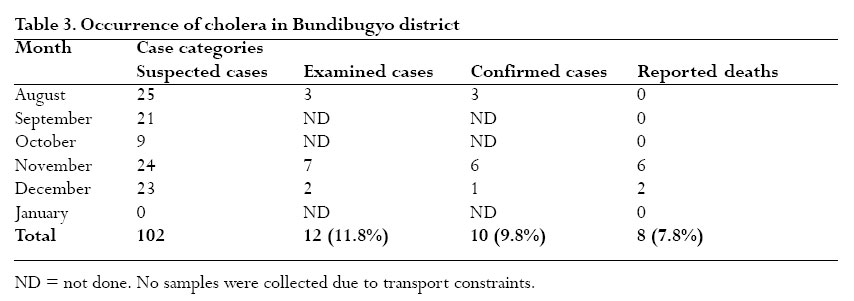
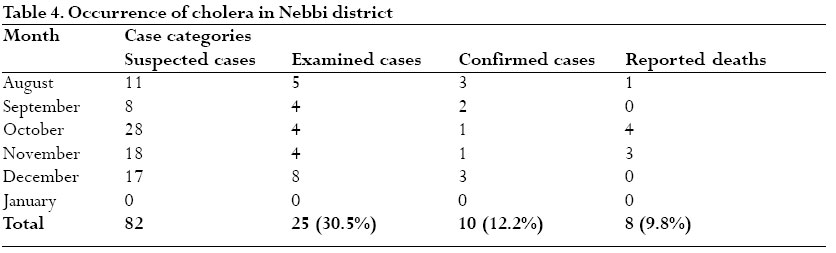
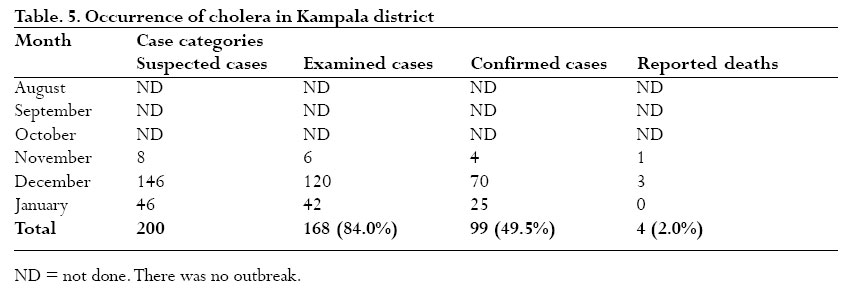
of occurrence is needed for effective control. Introduction Cholera is a severe diarrheal disease of humans caused by the bacterium, Vibrio cholerae. This organism is the most deadly of all pathogens frequently causing diarrheal illnesses, and accounts for an annual mortality rate of five million persons worldwide 1 . So far the world has witnessed seven pandemics of cholera 2 , and in most of the outbreaks of this disease, climatic influence, such as El Niño, has continued to be debated 3 . El Niño refers to the exceptionally severe and prolonged warm periods above normal that occur in the Central Pacific Ocean around the equator 2, 4. This climatic event occurs every 2 - 7 years, and usually lasts approximately a year 2, 5, 6 . This unusual warming creates storms and disrupts wind patterns 2 , and often begins when the prevailing easterly winds weaken over the Pacific Ocean. Although little is known about El Niño, it is now understood that the main rain zone is shifted eastwards towards the Central Pacific, causing a prolonged dry period in Northern Australia, Indonesia, and the Philippines and this is often associated with fires 4 . On the other hand the horn of Africa becomes wet, and northeast Brazil dries out. In general, El Niño leads to global consequences “natural disasters” in several places, with areas that are usually dry becoming wet and vice versa 5. However, with the exception of North America and Australia, the greatest climatic effects of El Niño are experienced in developing countries, mainly because these countries are poorly equipped to deal with weather extremes 4 . This weather pattern and cholera have been thought to have a link since the 1970s 7 . In particular, attention has been focused on this association because in the 1997 El Niño, several major cholera outbreaks affected most countries in East Africa, with spread toward central and southern parts of the continent 4. In Uganda, this epidemic started in November 1997 and rapidly encompassed 41 districts in all regions of the country. By December 2001, the occurrence had been restricted to some few “endemic districts” along Lake Albert region 8 . The purpose of this study was to determine the status of occurrence of cholera in these five endemic districts in Uganda during the 2002 – 2003 El Niño rains, a step that would help further assess the link between cholera and this phenomenon. The other objective was to determine the serotypes and antibiotic sensitivities of V. cholerae isolates from these outbreaks. Methods Purposive sampling was carried out from August 2002 to January 2003. Stool samples or rectal swabs were collected from cholera suspect cases admitted to health units in the districts of Bundibugyo, Hoima, Masindi, Nebbi and Kampala (Uganda). A cholera suspect case was defined by the presence of cholera-like symptoms, that is, profuse watery diarrhea with vomiting and stools with the appearance of rice water. When a cholera epidemic was reported, district laboratory and surveillance focal persons visited and established whether there was an outbreak. Samples were collected, preferably before antibiotic therapy was administered, although most patients had been on antibiotics before the sample collection team reached the site. Personal data such as name, age, sex, and location, date of onset of disease, suspected disease and type of treatment received, if any, were collected. All the samples were collected into Cary-Blair transport medium (Oxoid) and delivered to the Central Public Health Laboratory, Kampala. Standard microbiological methods were used for the culture and identification of V. cholerae isolates, as described previously 9. The isolates were subsequently serotyped by agglutination with Polyvalent 01 and monospecific Ogawa and Inaba antisera (GlaxoWellcome, England) 10. Additionally, isolates were assessed for susceptibility to seven (ampicillin, chloramphenicol, ciprofloxacin, tetracycline, nalidixic acid, cotrimoxazole and erythromycin) anti-bacterial drugs by the standard disk diffusion assay 11. Isolates were categorized as sensitive or resistant based on the standardized zones of inhibition. Results Cholera status in Hoima district We have tested 145 clinical specimens from cholera suspected cases admitted to health centers in Hoima district. After analysis, 49.6% of these samples were culture positive for V. cholerae.As shown in Table 1, the highest number of cholera suspected cases were reported in August and September coincident with the onset of El Niño rains. Subsequently, the number of cases went down and no cases were reported in December, although resurgence was noted in January. Sixty-three deaths were reported (case fatality rate 14.2%). Cholera was only reported in the three sub-counties of Kabwoya, Buseruka and Kigorobwa, which are landing sites on Lake Albert. The parishes affected were Naiwonga and Rwamutonya in Kabwoya, Chakapere, Kasenyi and Toonya in Buseruka and Kapapi, Kasenene, Kyangi and Bwiika in Kigorobwa. Serological typing identified all the isolates as V. cholerae 01, biotype El Tor, serotype Ogawa. Cholera status in Masindi District All the reported cases were from Butyaba sub-county, a fish-landing site on Lake Albert. Masindi had a stable prevalence from August to November; however, the number of cases peaked in November (Table 2).Twelve deaths were reported (case fatality rate 12.5%) during this period. Subsequently, the cases drastically declined in December and there were none reported in January as the El Niño rains were winding off.Thirty eight clinical specimens (39.6%) were analyzed and of these, 10 were culture positive for V. cholerae. As in Hoima district, serological typing identified all the isolates as V. cholerae O1, biotype EL Tor, serotype Ogawa. Cholera status in Bundibugyo district In Bundibugyo, twelve samples were analyzed and 8 were confirmed positive for cholera.All the reported cases were from Rwebisengo parish in Ntoroko sub-county. Rwebisengo is at the shores of Lake Albert and also borders the Democratic Republic of Congo. Case-fatality rate was 7.8% (Table 3). Bundibugyo had stable cholera prevalence throughout the study period with no cholera cases reported in January 2003.All cholera isolates from this district were also serologically identified as V. cholerae O1, biotype EL Tor, serotype Ogawa. Cholera status in Nebbi district During our study, 82 suspected cholera cases reported in Nebbi district. The cases came from Panyimur (Nya-ageparish) and Padyere sub-county. Panyimur is a landing site on the shores of Lake Albert and also borders the Democratic Republic of Congo. Nebbi had a stable cholera prevalence from August 2002 to December 2003, though with a peak in October. Case-fatality rate was 9.8% (Table 4).Ten out of 25 cases sampled, were culture positive. Cultural, biochemical and serological characterization, also identified the isolates as V. cholerae 01, biotype El Tor, serotype Ogawa. Cholera status in Kampala district In Kampala district, there were a total of 200 suspect cholera cases reported during the investigation. No cases were reported from August to October. However, cases emerged in November and drastically peaked in December, showing a typical epidemic curve. Because of concerted control measures, the number of cases significantly dropped to 46 in January and only 4 deaths were reported (case-fatality rate 2%) (Table 5). All deaths occurred in the community, before admission to the cholera treatment centre in Mulago. The index case was from Natete in Rubaga division; however, cholera rapidly spread to other parishes including Busega, Mutungo, Kitintale in Nakawa division, Kibuli in Makindye division, Busiga in Ndeeba parish, Kisenyi and Nabugabo in central division.We examined 168 clinical specimens and 99 were confirmed positive by culture. Isolates from this district were also identified as V. cholerae 01, biotype El Tor, serotype Ogawa. Reflections on cholera status During this study, a total of 924 suspected cholera cases were received in health centers in the five districts.There were 95 fatalities reported (case fatality rate 10.3%) and out of the 388 cases sampled, 201 were positive for cholera.At district level, our data suggest that Hoima district was the worst hit by this epidemic, as reflected by the largest number of suspected cases (48.1%) and highest case fatality rate (14.2%). Moreover 66.3% of the combined deaths occurred in this district. Interestingly, Kampala district, though second to Hoima in respect to suspected cases (21.6%), experienced the lowest case fatality rate (2.0%), suggesting disparity in magnitude of response to the epidemic in the former as opposed to the other districts. Antibiotic sensitivity patterns of the V. cholerae isolates We found that 100% of the V. cholerae isolates from all the five study districts were sensitive to ciprofloxacin, tetracycline and erythromycin. Conversely, 100% of the isolates were resistant to cotrimoxazole and chloramphenicol while 98.5% and 89.9% isolates were resistant to ampicillin and nalidixic acid, respectively. It should be noted that the sensitivity to nalidixic acid varied from district to district with 100% of the isolates from Nebbi district being sensitive. Discussion The salient finding from this present investigation is that almost all the study districts reported cholera outbreaks coincident with the rains suggesting that cholera is indeed endemic in these districts and reinforcing a link between El Niño and cholera. All the isolates were V. cholerae 01, biotype El Tor, serotype Ogawa. This latter finding is in agreement with previous studies which showed that currently, the El Tor biotype is virtually responsible for all the cholera cases through out the world 8, except in Bangladesh where the “classical”biotype is predominant 9. Just like its epidemiological influence on malaria and other insect and vector-borne diseases 4; El Niño also probably ushers in factors that trigger cholera outbreaks. V. cholerae have reputable environmental resistance, and moreover are microbial inhabitants of several water ecosystems including chitinaceous zooplankton and shellfish 2, 7.These attributes have been implicated as contributing factors in precipitating endemic occurrence in specific localities following outbreaks 2. The particular zooplankton or V. cholerae vectors in the endemic districts in Uganda, however, need to be elucidated. Arguably, EL Niño might favor the proliferation of these vectors, hence V. cholerae, and thus initiating the outbreaks. It is interesting to note that whereas cholera cases in Uganda have apparently been in the decline since 1998, with only 305 cases reported countrywide in 2001 12, our findings data show that the cholera situation in these endemic districts worsened as the number of cases shot up (924 reported cases) greatly, reversing the trend witnessed over the last three years. This change clearly points to the influence of El Niño phenomenon on cholera status in these districts. However, of perhaps more interest in this study is the observed disparity in respect to control and impact of the disease in Kampala district, as opposed to the others. Kampala district witnessed very few fatalities and the epidemic was arrested within only 3 months whereas the disease lingered for the entire study period in the other districts.What does this mean? And what can be learned from these data? It’s apparent that there was probably less effective response in the latter districts as opposed to Kampala.As the problem of cholera is not bound to go 2, programs of control could change enabling proper and effective containment and reduction or elimination of fatalities. Probably capacity should be developed in other endemic districts so that they can rapidly respond and manage any cholera situations in the future without heavily relying on the centralized system based in Kampala. Currently, with proper treatment, the case fatality rate for cholera should be less than 1% 13. Based on this, the case fatality rates for Hoima, Masindi, Nebbi and Bundibugyo, are very alarming and deserve attention. Moreover all the latter districts are bordering Lake Albert, implying that being in close proximity to this Lake is a major risk factor of cholera outbreaks in Uganda. V. cholerae isolates in the present study exhibited varying antibiotic sensitivity.The isolates were only 100% sensitive to erythromycin, ciprofloxacin and tetracycline.These results are consistent with previous studies that have reported varying sensitivity of V. cholerae isolates from different regions to the commonly used antibiotics 6, 14. In conclusion, the results have highlighted the importance of El Niño in influencing the pattern of cholera occurrence in endemic districts in Uganda and call for readiness.These data also indicate a need for urgent studies to determine the social and environmental factors associated with cholera epidemics in these endemic districts, and more so emulation of the Kampala response in other districts so as to achieve effective control in the future. Acknowledgements We thank Sandra Perez for her critical review of this manuscript and the District Directors of Health Services (DDHS), together with the district laboratory and surveillance focal persons, for facilitating the collection of samples. This work was supported by the Ministry of Health, Uganda. References
Copyright © 2006 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs06022t2.jpg] [hs06022t1.jpg] [hs06022t5.jpg] [hs06022t4.jpg] [hs06022t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}