 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 6, No. 2, June, 2006, pp. 104-107 Trauma at a Nigerian teaching hospital: pattern and documentation of presentation L.O.A. Thanni1 O.A. Kehinde2 1. Dept of Orthopaedics & Traumatology, College of Health Sciences, Olabisi
Onabanjo University, Sagamu, Ogun State, Nigeria. Code Number: hs06024 Summary Background and Objectives:This study is aimed at identifying the characteristics
of injuries and determining the efficiency of documentation of patients’records
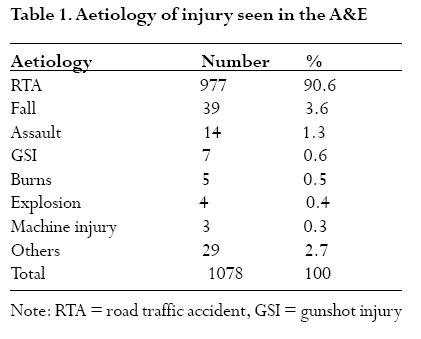
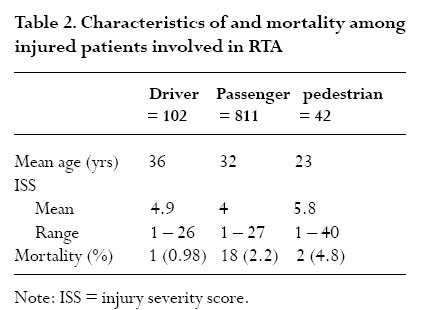
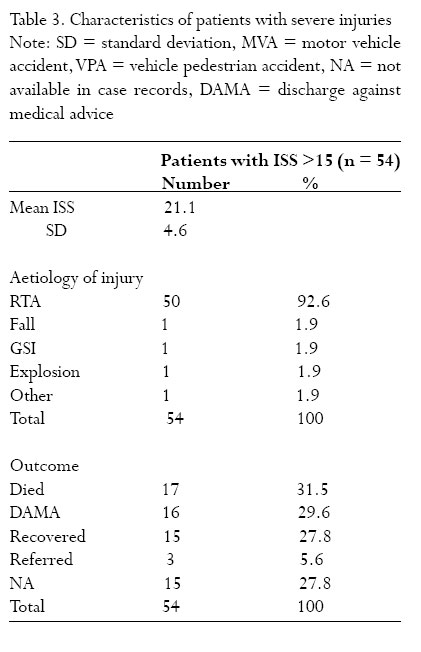
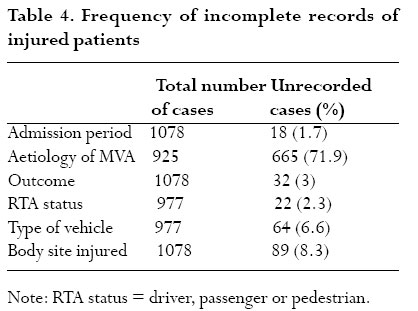
in a tertiary hospital where there is no trauma registry. Key words: trauma; injury; road traffic accident; mortality; injury severity score, pidemiology. Introduction Trauma care research in Nigeria is still in the developmental stages with relatively few published data. There are no trauma registries, thus making documentation of injuries inadequate and accessing these data problematic. However, road traffic injuries have been shown to be the most frequently encountered injuries seen in hospitals while population based studies are non existent1, 2 . Apart from funding, specific limitations to trauma research have not been documented. The World Health Organisation’s World Health Day for 2004 was dedicated to road safety. This level of attention to road safety underscores the global burden of road traffic injuries and the need for public health concern towards reducing this epidemic. According to the WHO, worldwide each year, 1.2 million people are killed and 50 million are injured in road traffic accidents. The cost to low income countries is approximately 1% of their gross national product, more than the total development aid received by these countries3 . Road traffic injuries are ranked ninth among global causes of disability-adjusted life years lost and developing countries account for over 80% of deaths globally due to road traffic accidents3 . The morbidity and mortality burden in developing countries is rising due to a combination of factors, including rapid motorisation, poor road and traffic infrastructure as well as the behaviour of road users4 . This contrasts with technologically advanced countries where the indices are reducing5, 6 . Effective policies on road safety can only be developed when based on the evidence of local research and designed for target demographic, economic and political environments. Successful interventions in developed countries cannot simply be adopted but rather adapted because of differences in the behaviour of road users, quality of vehicles and the environment 4, 7 . Adaptation of intervention strategies and technology requires research to document peculiar local injury pattern, circumstances of occurrence and outcome of management. This study was designed to identify the characteristics of injuries as seen in a Nigerian center and identify areas of development to enhance trauma research, an important adjunct to effective policy formulation and implementation Patients and methods Olabisi Onabanjo University Teaching Hospital is located in Sagamu close to two major highways connecting the Southwest of Nigeria to the Northern and Eastern regions of the country. The case records of patients seen with injuries at the Accident and Emergency (A&E) unit were reviewed for the period from January to December 2003. The A&E receives all paediatric and adult surgical emergencies in the hospital. Personal data, type of injuries sustained, causes and circumstances of injuries as well as outcome of treatment were extracted from the case files and entered onto a computerized questionnaire designed for the purpose.To assess the severity of the injuries sustained, injury severity score (ISS) was computed for each patient from the file record of injuries sustained. Data extraction was manually done by reviewing each case file since there was no purpose designed computerized trauma registry. Analysis of data was done using Epi info 2002 (Centres for Disease Control, USA), generating simple frequencies for non numeric variables and simple averages for numeric variables. Chi Square was used to compare the difference in mortality among patient groups. Results During the 12 month study period, 1078 injured patients were seen in the Accident and Emergency unit. The mean age of all patients was 31 years (range 3 months to 85 years). There were 664 male (61.6%) and 414 (38.4%) female patients. Analysis of the frequency of injury to different anatomical areas of the body showed that multiple body sites were injured in 20.8% of patients while the lower limb alone was involved in 22.2%, the head (including the scalp and face) 20.8% and the upper limbs 18.8%. Lacerations (n = 408) and fractures (n = 266) were the most frequently seen injuries accounting for 62.5% of all injuries. Table 1 outlines the aetiology of injuries. Road traffic accident was the most common cause of injuries, being responsible for 90.6% (n = 977) of patients’ injuries. Burns 0.5% and gunshot injuries 0.6% were uncommon. Victims of road traffic injuries (RTI) included 102 drivers, 811 passengers and 42 pedestrians while 22 patients had no record of their status in the accidents. As shown in table 2, the average age of the drivers was 36.1 years (range 13 – 84 years) while that of the passengers was 31.9 years (range 3 months –80 years) and pedestrians 22.8 years (range 2 –72 years). The aetiology of RTA was mostly motor vehicle accidents (MVA), in 94.7% of cases. Other causes included vehicle pedestrian accident (VPA) 4.1%, armed attack 0.4% and others 0.8%.The recorded causes of motor vehicle accidents were burst tyre, collision and loss of control. Records of the causes of motor vehicle crashes were however not available in 71.9% of cases. A minibus, a popular mode of commercial transportation, figure, was involved in 63.9% of RTAs, while cars were involved in 14.8% of cases. Motorcycles and pedal bicycles were involved in 6.2% and 0.6% of cases respectively while lorries and trailers were involved in 1.1% of cases each. The overall injury severity score (ISS) ranged from 1 – 40 (mean 4.1). Table 2 indicates that for patients involved in RTA, the mean ISS for drivers was 4.9 (range 1 – 26), passengers 4 (range 1 – 27) and pedestrians 5.8 (range 1 – 40). As shown in table 3, severe injuries, ISS >15, occurred in 54 patients, with a mean ISS of 21.1 (range 16 –40). Multiple injuries occurred in 59.3% of these patients while head injury occurred in 9.3%.Table 3 also shows that RTA was responsible for 92.6% of severe injuries of which 90% were due to MVA and VPA 8%. Overall mortality in the study population was 2.1% (23 of 1078 patients) and all resulted from road traffic injuries. Deaths were associated with multiple injuries in 60.9% (14/23) of cases while 30.4% (7/23) were associated with head injury. Mortality from severe injuries (ISS > 15) occurred in 31.5% (17/54) of patients in this subgroup, representing 73.9% (17/23) of all deaths in the A&E. There was no significant difference in the number of deaths among drivers, passengers and pedestrian victims of RTA (÷2 = 1.88, df = 2, p = 0.34). Several parameters were not recorded in some patients’ case records.These include time of injury, 100% (not recorded for all patients studied), aetiology of motor vehicle accidents, 71.9%, type of vehicle, 6.6%, body area injured, 5.5%, outcome of treatment, 3%, status of patient in accident, 2.3% and time of arrival in hospital, 1.7%, Table 4. Discussion Our results show that RTA is the preeminent cause of injuries seen in our center.The high prevalence of RTA, 90.6%, is noteworthy as it has implications for the provision of adequate facilities for managing road traffic injuries (RTI) among other injuries. This high rate is probably because of the location of the study center, close to two major interstate highways. Solagberu et al8 has previously reported 62.3% prevalence of RTA in their trauma series from Nigeria but this is the highest prevalence rate so far reported from West Africa. This rate is high compared with 19% reported from the Netherlands5, 18% to 31% from Kenya9, 10 and 20% from the West Indies11. Motor vehicle crashes were responsible for over 90% of RTIs in this report unlike in China where pedal cycles are involved in 70% of cases12. The use of alcohol was not included in our analysis as the data was unavailable.Alcohol use is involved in up to 70% of road crashes in the US13 but as low as <2% in China12. These are indicative of local and regional differences in road accidents epidemiology. Soft tissue injuries and fractures were the most common injuries. This is consistent with previous observations from Nigerian centers although prevalence varies8, 14. Pedestrians and passengers have been reported to be the common victims of RTA in developing countries4, 8. This report shows that while passengers were disproportionately affected, drivers were more than twice as many as pedestrians. The disproportionate number of passengers is due to the involvement of the commercial minibus (figure) in over 60% of the RTA. Users of this mode of transportation are compelled to use this ubiquitous vehicle of intra and intercity transportation because it is relatively cheaper than cars and more commonly available4. Its use results in a high rate of injuries per crash. Severity of injury was however greater among pedestrians than among the others. Pedestrians are vulnerable road users. In motorized countries, pedestrian deaths have been declining probably because of a decline in foot trips6. For motorizing countries where a lot of foot trips are made, it is important for vehicles to have pedestrian friendly fronts, among other measures to reduce pedestrian morbidity and mortality. Mortality in this report was 2%. This is within the reported range of 0.5% and 6% worldwide. However, as in other reports, head injury and multiple injuries were mostly responsible1, 15, 16. These patients accounted for about 60% of those severely injured that died. Improving the quality of acute care in the A&E should target the needs of these patients, including fluid, blood and oxygen therapy.These are oftentimes in short supply. RTI were responsible for all mortality and over 90% of all severe injuries.The role of prehospital care and the interval between injury and admission into the A&E could not be studied, as the data was unavailable. However, both are known to be important factors in determining outcome. Stewart17 has observed that further reduction in injury mortality is obtainable through injury prevention rather than injury therapy but this may only be true of technologically advanced countries where advances have been made in both areas. Developing countries like Nigeria need as much improvement in therapy as in prevention. The limitation of trauma case analysis by incomplete data is obvious from this report where only 39.5% case records of patients were found for analysis. Even the central records were deficient for the total number of surgical cases or the various types. To strengthen trauma research, computerized trauma registries should be established in all major trauma centers as well as having regional registries.This will ensure the availability of complete patient records for auditing.Audit reports such as ours will therefore be more accurate thus enhancing policy making for injury prevention and improving the quality of trauma care. Acknowledgement The authors gratefully acknowledge the contributions of Q.A. Allinson, the entire staff of the medical records dept of the study center and all the House Officers that assisted with data collection. References
Copyright © 2006 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs06024t4.jpg] [hs06024t2.jpg] [hs06024t1.jpg] [hs06024t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}