 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 6, No. 2, June, 2006, pp. 113-117 Acceptability of maxillary major connectors in removable partial dentures Abiodun Olabisi Arigbede*, Oluwole.O Dosumu*, Temitope Ayodeji Esan,** Patricia A.Akeredolu.*** * Department of Restorative Dentistry, Faculty of Dentistry, University of Ibadan. Code Number: hs06026 Abstract Background:The choice of connector lies between plate, a bar or a combination of bars, which may cross the palate in various positions. Many opinions have been expressed concerning the acceptability to the patients of the various forms of palatal connectors but there have been few investigations. Introduction Major connector is an important component of removable partial denture (RPD). It is a part of the partial denture to which all other parts are directly or indirectly attached 1, 2 . . It provides cross arch stability, which helps to resist displacement by functional stresses. It contributes to the support and bracing of a partial denture by distributing functional loads widely to the teeth, and in case of the maxilla, to the mucosa. It also provides indirect retention by contacting guide surfaces and in upper jaw the palatal mucosa2 The choice of connector lies between a plate, a bar or a combination of bars, which may cross the palate in various positions. Plates usually offer more palatal coverage than bars. Although there are controversies about what constitutes the dimensions of plates and bars in the upper arch, the difference is clear-cut in the lower arch 3 . A maxillary major connector type which one investigator calls a broad bar may be referred to as a strap, that is, a modified palatal plate by another1,2,7 . Also, the choice of the shape and location of major connectors is greater in the upper jaw because of the larger area available for coverage offered by the hard palate 2 The location and areas of tissue coverage by a major connector is of uttermost importance, as these features will affect the acceptability of the prosthesis and its eventual performance. Even though, over the years, it has been observed that patient’s tolerance of the various major connector designs was as great as the number of dentists involved in making the designs 4,5 it is still imperative to establish the most acceptable maxillary major connector design. The single palatal bar has perhaps been described as the most widely used and the most preferred maxillary major connector, while the metal plate was the least preferred of the maxillary major connector1 . Proponents of the mid-palatal bar suggest that this is a favourable position since it leaves the anterior “playground free and also the posterior region of the palate, which may be contacted by the dorsum of the tongue during speech and swallowing6 . Palatography conducted for selected consonant sounds showed that the incisal papilla and lateral aspect of the palates were the areas more frequently visited by the tongue7 . However in another study8 the mid- palatal bar was reported to be the least preferred of the major connector design because of ready detection of two prominent transverse margins by the tongue.This supports the result obtained in another study9 where metal borders parallel to the tongue were better tolerated than transverse borders. In addition, it was stated that “a middle palatal bar is usually a source of annoyance to the patient as it is positioned in an area where the tongue makes frequent contact with it during swallowing and speech”10. However amongst the transverse palatal bars that is anterior palatal bar, mid palatal bar and posterior palatal bar, the posterior palatal bar has been documented as the most suitable type of the palatal bars for the following reasons10: It is less conspicuous to the tongue than the middle or anterior bar; it often fulfils the function of an indirect retainer; and it is in an area less frequently associated with bony prominence or with thin mucosa. A palatal plate which was otherwise called a strap in a particular publication was described as the connector of choice in most instances2,11. It was however advised that the active speech area should be avoided when possible11. However in most studies, patients reported poor tolerance with speech, swallowing and comfort with this type of major connector than any other type9. The anteroposterior bar connector on the other hand has been described as a configuration that is also commonly used in cases of bilateral bounded saddles11. The anterior-posterior lengthening of the denture base provides added stability while the greater the space in between the bars the less irritating they are for the tongue6. The anteroposterior bar connector design was referred to as a ring connector by one author2 but it has been argued that the ring connector is not quite the same as a combination of anterior and posterior bars, as the palatal aspects of the teeth and their gingivae margins are covered in ring connectror11. Little has been reported about its interference with normal oral function. The ring connector is bulkier in arrangement than the anteroposterior bar system6. It has the advantage of being able to link multiple saddles together, greater stimulation of the palate and can also be used in place of a plate in case of maxillary torus. Its disadvantage is in its coverage of gingival margin and its reported interference with speech and patent’s comfort6. Though the relative advantages of metallic and acrylic resin dentures are well known, it is not clear which one will prefer. Several authorities have reported that acrylic resin may be preferred over the thinner metal base for aesthetic reasons.1,10. It has also been documented that dentures made entirely in acrylic resin are used in situations where the life of the denture is expected to be short or where alterations or relines will be needed2. Furthermore, several studies12 have concluded that dentures made of heat-cured acrylic resin were the most retentive and thus the most preferred. However, it has been reported that most metal bases are preferred to acrylic resin bases because temperature changes are transmitted through the metal base to the underlying tissues, thereby helping to maintain the health of tissues.Also the inherent cleanliness of the cast metal base and its resistance to abrasion from cleaning agents contributes to the health of oral tissues when compared with an acrylic resin base1,12. The objectives of this study were to: a. Compare subjective patients’reactions to three maxillary major connectors:
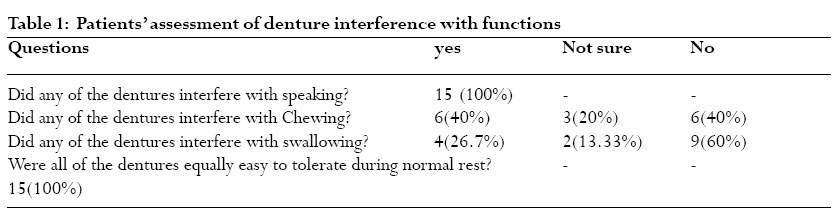
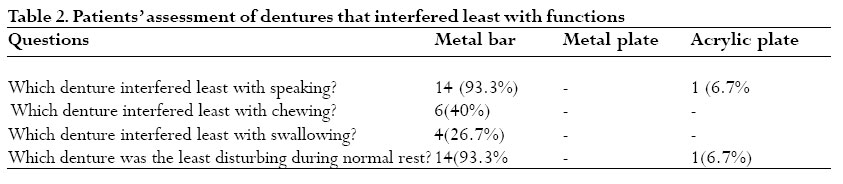
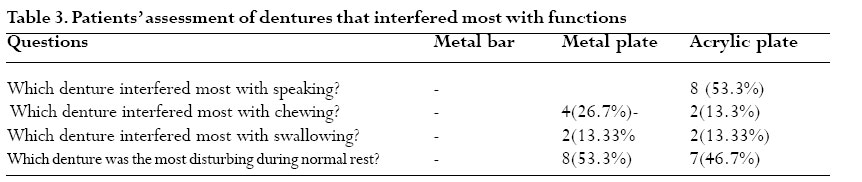
metal bar, metal plate, and acrylic connectors Material and methods Fifteen consecutive patients attending the prosthetic out– patient clinic of the Dental Center, University College Hospital, Ibadan who had never worn dentures were recruited into the study. Patients with advanced periodontal diseases and where the potential abutment teeth are restored with crown or amalgam restorations that extended below the gingival level were excluded. The consent of patients as well as the ethical clearance was obtained from the beginning of the study. The patients were given serial numbers and they were randomly divided by balloting into three groups: A, B, and C, each group having 5 patients. For each patient, three sets of dentures with the different major connectors under study that is metal palatal bar, metal palatal plate and acrylic plate were fabricated. Each denture was to be worn for five days Group A wore the dentures for the first fifteen days in the order: metal bar connector, metal plate connector and acrylic plate connector. Group B wore the dentures in the order: acrylic plate connector, metal bar connector, and metal plate connector; while Group C wore the dentures in the order: metal plate connector, acrylic plate connector and metal bar connector. After the initial fifteen days of evaluation, the patients were required to wear the dentures in the order preferred for another six days.The patients were requested to fill the questionnaire after the three – week evaluation period. Data was analysed using SPSS version 11(Inc Standard version2001). Analysis included frequencies and percentages. Results Fifteen patients who consented were recruited for the study 6(40%) were males while 9 (60%) were female. Their age ranged from 18 to 60 years. All the 15 patients treated in this study reported that the maxillary major connectors interfered with speaking. Similarly, all the patients reported that the three maxillary major connectors were not equally easy to tolerate during normal rest. Only 6 patients (40%) felt that the connectors interfered with chewing. Only 4 (26.7%) of the patients felt that the connectors interfered with swallowing (tables 1,2, 3) Fourteen patients (93.3%) reported that the palatal metal bar connector interfered least with speaking while only one patient (6.7%) felt that the maxillary major connector that interfered least with speaking was acrylic palate (table 2.) During normal rest 14 patients (93. 3%) believed that the metal bar maxillary major connector was the least disturbing while only 1(6.7%) patient believed that it was the acrylic plate connector (table 2). Eight of the subjects (53.3%) thought that the acrylic maxillary major connector interfered most with speaking while only 4 patients thought that it was the palatal metal plate connector. (table 3) Four patients (26.7%) reported that the palatal metal plate connector interfered most with chewing, while 2 patients (13.3%) believed that the acrylic plate is the connector that interfered most with chewing. (table 3) Two patients (13.3%) selected the palatal metal plate and another 2(13.3%) selected acrylic plate connectors as the connectors that interfered most with swallowing. (table 3) During normal rest however, 8 patients (53.3%) believed that the palatal metal plate was the most disturbing connector, while 7 (46.7%) believed that it was the acrylic plate connector. (table 3). Fourteen patients (93.3%) preferred the denture with metal palatal bar major connector whereas only one patient preferred the denture with acrylic plate major connector design. No patient preferred the palatal metal plate connector design. Discussion Many opinions have been expressed concerning the acceptability of major connector but such studies in Africa are very few. The dentist should select the one which will least interfere with speech, mastication, swallowing and comfort. Panagiotouni et al 13 advocated a proper selection of major connector for every case of partial denture so that the major connectors promote the acceptance of the prostheses by the patients. In our study, a majority of the patients (93.3%) reported that the denture with metal bar connector interfered least with speech. The reason for the no or little interference with speech by the bar connector may not be unconnected with the fact that the active speech areas are not covered in this connector design. Several authorities had earlier referred to the palatal aspect of the upper anterior teeth and the palatal mucosa behind them as the playground of the tongue, an area that should never be covered by a connector6. Similar results were obtained by Campbell9, Wagner and Traweek14 in their studies, where the bar connector was reported as the most acceptable maxillary major connector because it interfered least with speaking, while metal plate connector was reported as the least acceptable because it interfered most with speaking. However, they did not investigate acrylic resin plate. Eight subjects (53.3%) described the acrylic denture as the ones that interfered most with speech. The reason for the low tolerance for acrylic resin denture from speech point of view in this study may also be related to the report of Laird and Laminie3 which stated that acrylic resin denture requires a combination of thickness and broad coverage to give the necessary strength and rigidity. This combination of wide coverage and thickness of acrylic plate may be responsible for low speech intelligibility recorded with the acrylic resin maxillary major connector. Furthermore 40% of our study population felt that none of the dentures interfered with chewing while another six patients (40%) reported interference of the dentures with chewing (table 1). This is similar to the studies done by Wagner and Traweek14 where 55% reported no interference of any of the denture type with chewing. However in a recent study of denture wearers all the patients showed a reduced performance in masticatory ability15. Out of the six patients that reported interference with chewing, four (66.7%) indicated that the denture with metal plate connector interfered most with chewing, while the remaining two (33.3%) patients referred to acrylic denture as interfering most with chewing. All the six patients described metal bar connector as interfering least with chewing.These results are similar to the ones reported byWagner and Traweek14. In our study, 60% of the patients indicated that no denture interfered with swallowing. Whereas four patients (26.7%) indicated that the metal bar connector interfered most with swallowing while metal plate connector interfered least with swallowing.Two patients (13.3%) were not sure whether any of the dentures interfered with swallowing. The results were similar to those reported by Campbell9, and Wagner and Traweek14. All the patients treated in this study indicated that the dentures were not equally tolerated during normal rest. Also, all the patients except one described the denture with the metal bar connector as the least disturbing during normal rest whereas eight patients (53.3%) felt that the most disturbing major connector is the metal plate connector followed by acrylic plate (46.7%). This may also be related to the area of tissue coverage by the connector. On the overall acceptability of the types of dentures under study, only one of the subjects treated in this study (6.7%) preferred acrylic partial denture, while fourteen subjects (93.3%) preferred the denture with metal bar connector.This observation is similar to other findings3,8,9,14 which have also independently spoken favorably about the high acceptability of the maxillary metal bar major connector.Though the metal bar major connector like other major connectors has its own disadvantages which include possible accumulation of food under the connector (due to flexing) and unavoidable thickness of the connector causing tongue irritation1,10,11, these shortcomings appeared not strong enough to limit patients’ acceptance of this particular maxillary major connector design. The acrylic resin connector ranked next to metal bar connector in acceptability. Some studies1 have shown that acrylic resin denture base may be preferred to the thinner metal base to provide fullness in the buccal flange or to fill a maxillary buccal vestibule for aesthetic reason. Other studies 16 have shown an increasing popularity of upper acrylic partial denture among some groups of patients. The result of this study also identified metal plate connector as the least acceptable major connector design. This is similar to other studies9, but there are situations when dentist should insist on them for the health of tissues. These situations arise when there is insufficient tooth support available for a denture and added mucosa support is necessary6. Conclusion The result of this study show that metal bar major connector was the most acceptable maxillary major connector while acrylic resin plate was more acceptable than metal plate maxillary major connector. It also confirmed the influence of connector design on patient acceptance of removable partial denture. References.
Copyright © 2006 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs06026t2.jpg] [hs06026t3.jpg] [hs06026t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}