 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
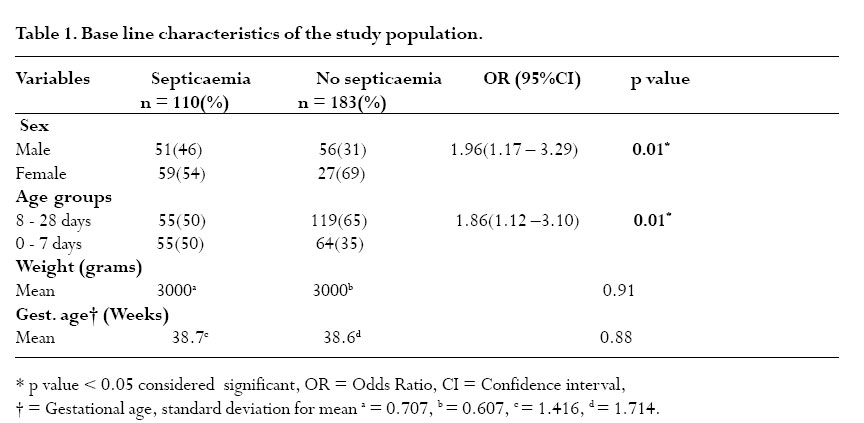
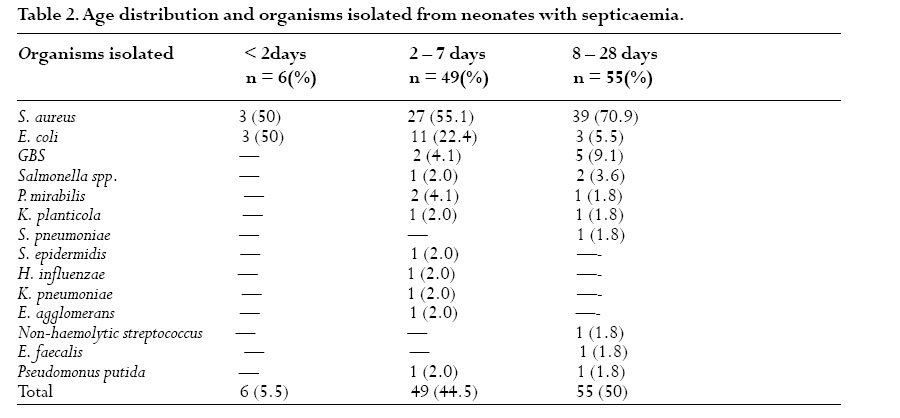
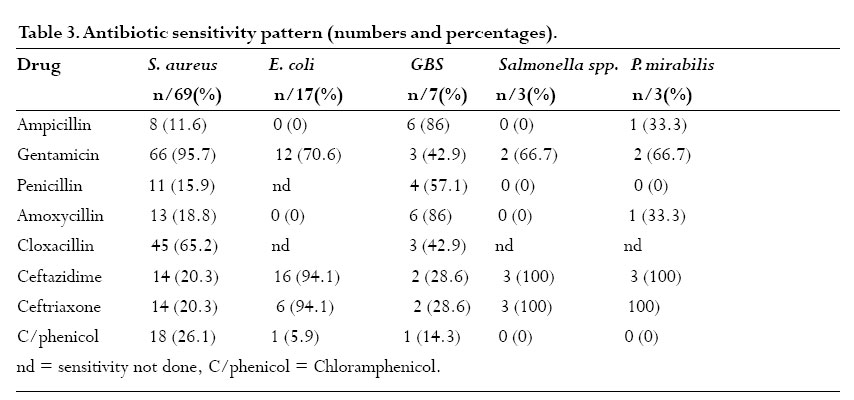
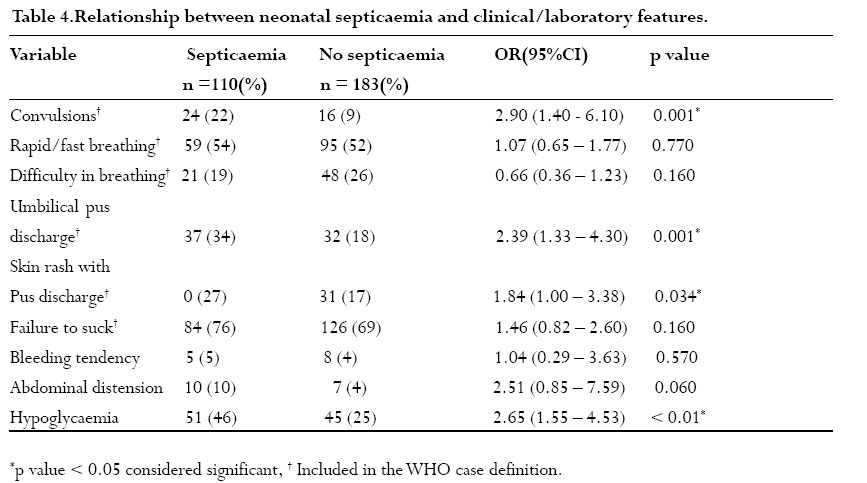
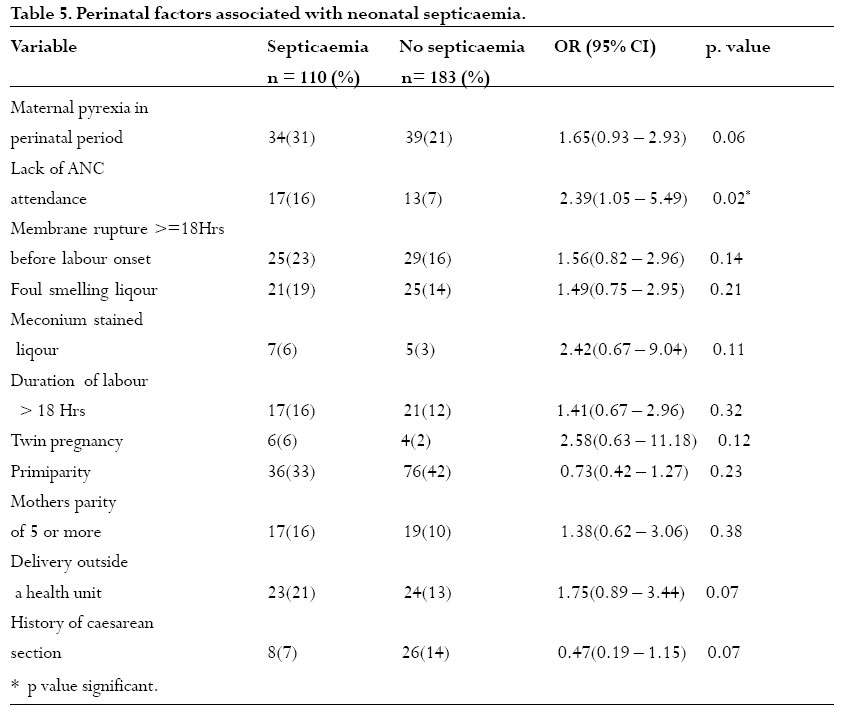
African Health Sciences, Vol. 6, No. 2, June, 2006, pp. 120-126 Aetiology, risk factors and immediate outcome of bacteriologically confirmed neonatal septicaemia in Mulago hospital, Uganda. J. Mugalu1, M.K. Nakakeeto1, S. Kiguli1, Deo H. Kaddu – Mulindwa2. 1Department of Paediatrics and Child Health, Mulago Hospital. Code Number: hs06028 Abstract Background: Neonatal septicaemia remains a major cause of morbidity and mortality.The aetiology, risk factors and outcome of this problem need to understood. Introduction The World Health Organisation (WHO) estimates that 85% of newborn deaths are due to infections including sepsis, pneumonia and tetanus. Of the infants identified with sepsis, 40% die and the biggest toll being in developing countries1 . Neonatal septicaemia continues to be a major health problem with up to 323 of every 1000 neonates seen in clinics presenting with clinical symptoms2 . Organisms isolated from the blood stream of babies with sepsis vary from area to area. There is a general trend in developing countries of isolating “new” pathogens such as Staphylococcus epidermidis3 compared to Staphylococcus aureus and Escherichia coli mostly isolated in Africa and other developing parts of the word4. Although the role of Group B Streptococcus in neonatal sepsis is well documented, high carriage rate of this organism in the genital tract of women in Africa does not correlate with an increased isolation from neonatal sepsis cases4 . There has been no documentation of the pattern of blood culture isolates in neonates in Uganda. In Uganda, the admission of neonates to the Paediatrics wards is often based on clinical grounds once a septic screen cannot be done due to inadequate laboratory facilities. It is important to establish the local sensitivity patterns and the causative pathogens of neonatal septicaemia. Risk factors associated with neonatal septicaemia would assist in planning for preventive measures. We report the results of a study conducted in Mulago Hospital, Uganda’s teaching and referral hospital. Methods Patients All neonates presenting to Mulago Hospital and whose parents/caretakers gave written informed consent and fulfilled the WHO case definition of neonatal septicaemia were enrolled. All neonates enrolled in the study had their blood drawn for culture before treatment was initiated. We excluded neonates with documented use of antibiotics at least 3 days prior to admission. The sample size was estimated at 290 using the formula by Kish and Leslie (1965) 5 assuming the prevalence of septicaemia in neonates with signs and symptoms of infection of 25.3%15. Study Site The study was conducted at Mulago hospital between July and November 2002. Mulago hospital is a national referral and teaching institution for Makerere University located in Kampala, the capital city of Uganda. Acute Care Unit is an emergency unit that admits acutely ill children 13 years and below for 24 hours management before being transferred to the general Paediatrics wards. Special Care Unit admits high-risk neonates from the labour wards of Upper and Lower Mulago hospital. SCU also receives babies referred from the neighbouring health facilities. Patients’ files and questionnaire responses were used to obtain relevant information. The WHO case definition for neonatal septicaemia used in the Integrated Management of Childhood Illnesses (IMCI) was used to select subjects for the study.A clinical diagnosis of neonatal septicaemia was made if a neonate presented with at least one of the signs in the tool. In Uganda, the tool is also used to screen neonates below one week of age and this study used the tool with the same modification. Procedures Collection and processing of samples Research staff carried out all the clinical procedures including the laboratory analysis. Approximately 2 ml venous blood was obtained after thorough cleansing of the patients’ skin for 2 minutes with povidine iodine and allowing the skin to dry before taking blood. One millilitre of blood was collected in each of two bottles containing brain heart infusion (BHI) in a ratio of blood: BHI of 1:10 and were taken to the laboratory within 30 minutes. Each bottle was incubated at 350C for 24 hours following which Gram stain was done. Subcultures were done on blood, Chocolate and MacConkey agar from those blood culture bottles that showed presence of bacteria on Gram stain. The agar plates were incubated under aerobic conditions. However, chocolate and blood agar plates were incubated in a candle jar to facilitate growth of Haemophilus influenza and Neisseria and better growth of Streptococci. Visible colonies were identified after 24 hours of incubation and a Gram stain using Preston Murrell‘s modification method was made. Standard biochemical tests were performed on pure colonies for identification of the different organisms. Blood cultures which showed no visible growth and were negative on Gram stain, subcultures were done daily up to a maximum of seven days before being discarded as negative. All culture bottles with mixed growths (defined as more than 2 types of bacteria) were discarded. The colour of each CSF sample was initially noted, a Gram stain was done, the number and cell types and the quantity of CSF protein were determined. Based on the Gram reaction, each sample was then inoculated on MacConkey, blood, chocolate and Sabouraud dextrose agar plates. The chocolate and blood agar plates were incubated under 5% carbon dioxide.All agar plates were re - incubated for another 24 hours before being declared to have no growth. Colonies of growth that occurred were identified using Gram stain, standard biochemical tests and haemolysins. Kirby - Bauer method of diffusion was used to determine antibiotic sensitivity. Blood sugar estimation was done on admission using a glucometer (Sure - StepR) and hypoglycaemia was defined as blood glucose level equal to or less than 2.5mmol/l. Approximately 1.5ml of blood collected in a sequestrene bottle was used to determine the White Blood Cell count (WBC), Erythrocyte Sedimentation Rate (ESR) and Haemoglobin (Hb) level. WBC were determined using a Coulter Counter. Results Two hundred ninety three neonates with a clinical diagnosis of septicaemia were recruited into the study. Of the 293 neonates, 201 (68.3%) were enrolled from Acute Care Unit (ACU) while 92 (31.4%) were from the Special Care Unit (SCU) a ratio of 2.2:1. Using the WHO screening tool, 55 (46%) out of 119 babies less than 8 days old and 55 (32%) out of 174 between 8 to 28 days old had bacteriological septicaemia. There were 186 females with a female to male ratio of 1.7:1.The sex, age groups, weight and gestational ages of babies are shown in Table 1. Late onset disease and male sex were significantly associated with occurrence of neonatal septicaemia as shown in table 1. The commonest isolated organism was S. aureus (62.7%) followed by E. coli (15.5%). There was a low isolation of Group B Streptococcus (6.4%). No single organism of Listeria monocytogenes was isolated as shown in table 2. (Table 3) Antibiotic sensitivity pattern Most of the organisms were sensitive to gentamicin. Generally, there was high resistance of organisms to ampicillin except for Group B Streptococcus . Factors associated with neonatal septicaemia A history of convulsions, umbilical pus discharge with a red anterior abdominal wall, skin rash with pus discharge and hypoglycaemia were significantly associated with neonatal septicaemia, table 4. The only perinatal factor associated with neonatal septicaemia was lack of antenatal care attendance by the mother (p = 0.02). On logistic regression analysis, male sex, late onset septicaemia, a history of convulsions, umbilical pus discharge with red anterior abdominal wall, hypoglycaemia and lack of antenatal care remained significantly associated with occurrence of neonatal septicaemia as shown in table 5. Outcome of neonatal septicaemia Of the 110 neonates with confirmed sepsis, 20 (18.1%) died. Of the 20 neonatal deaths, 17 (85%) died in the first 2 days of admission. Hypoglycaemia was the only factor significantly associated with occurrence of neonatal septicaemia (p < 0.01). Discussion Results of this prospective study indicate that neonatal septicaemia was confirmed in about 37% of the 293 neonates with a provisional diagnosis of the disease. This is similar to the 35% reported by Olusanya et al.7 in a Nigerian hospital and 33% reported by Mondal et al.8 in an Indian referral hospital. This prevalence however contrasts with the findings of Haque et al9 in Riyadh, Saudi Arabia and of Ako - Nai et al10 in Ile - Ife, Nigeria of 15% and 55% respectively. The latter study had a relatively small number of children who were also highly selected. In the current study, Staphylococcus aureus dominated the blood culture isolates (62.7%). Ako - Nai et al10 had similar findings in a study conducted between 1980 and 1988 in Nigeria. In Sagamu, South Western Nigeria, Olusanya et al7 cultured Gram positive organisms from 55% of neonates with sepsis, and about 35% of these were pathogenic Staphylococcus aureus. In two separate studies conducted by Antia - Obong et al11 at Calabar in South eastern Nigeria and Njokanma et al12 at Benin in mid - Western Nigeria, Gram positive organisms were implicated in cases of proven neonatal sepsis with Staphylococcus aureus as the predominant organism. In Zimbabwe4 and Saudi Arabia9, Staphylococcus aureus was found to be the predominant isolate in both early and late onset neonatal septicaemia. Dawodu et al13 and Alausa et al14 at the University College Hospital, Ibadan in Nigeria however found Escherichia coli to be the most predominantly isolated organisms followed by Staphylococcus aureus. In contrast to findings in other studies where many isolates of Staphylococcus epidermidis were reported, this was cultured only once in the current study.This indicates that it is not a common cause of neonatal septicaemia in Mulago hospital. Isolation of one organism perhaps is not significant but indicates emergency of “unusual” organisms among the aetiological causes of neonatal septicaemia. No single organism of Listeria monocytogenes15 was cultured in this study.This is not surprising since in Africa, other than in one study, this organism is not commonly isolated in neonates with septicaemia. It is however a common isolate among neonates with septicaemia in developed countries. Other organisms isolated include Salmonella spp. (2.7%), Proteus mirabilis (2.7%), Klebsiella planticola, Pseudomonas putida, Streptococcus pneumoniae (1.8%) each, Haemophilus influenzae, Klebsiella pneumoniae, Enterobacter agglomerans, non - haemolytic Streptococcus and Enterococcus faecalis.. From the results, the best antibiotic in the initial management of neonatal septicaemia is gentamicin.This is one of the first line drugs used to treat neonatal septicaemia in Mulago Hospital.Although the sensitivity to gentamicin by GBS was as that of cloxacillin, the sensitivity pattern of gentamicin to Staphlococcus aureus (95.7%) was better than the sensitivity of cloxacillin (65.2%) to the same organism. The second drug that can be used in combination with gentamicin should be able to cover GBS fairly adequately. Although ampicillin exhibited poor sensitivity patterns in this study, its coverage of GBS isolated in blood was quite good with a sensitivity of 86%. Ampicillin has two other advantages; it has a synergistic action when used together with aminoglycoside 2, 16 and is known to have 100% sensitivity for Listeria monocytogenes17 . Although no single organism of Listeria monocytogenes was isolated in this study, an antibiotic able to cover this organism should be one of the antibiotics used as empirical drugs because it is not easy to culture. Both gentamicin and ampicillin are affordable and are readily available in Uganda. Using these two antibiotics, about 5,000 Uganda Shillings (USD 2.5) is enough to treat a 3Kg. neonate with septicaemia for ten days. This study shows that ceftriaxone and ceftazidime showed high sensitivity against Gram-negative organisms like Escherichia coli, Salmonella spp. and Proteus spp. with a sensitivity of 100%. These drugs however showed low sensitivity for GBS (28.6%) and Staphlococcus aureus (20.3%). In countries where cephalosporins have been in use for a long time, similar resistance has been reported especially to organisms such as Staphylococcus aureus18; resistance occurs even faster when cephalosporins are used alone 19. Cephalosporins are also expensive; a ten day full course of ceftriaxone for a 3Kg. neonate with septicaemia costs 42,000 Uganda Shillings ( USSSD 21) which is about 8 times the cost of gentamicin/ampicillin combination. There are several factors significantly associated with occurrence of neonatal septicaemia including late onset disease, history of convulsions, history of umbilical pus discharge with reddening of the anterior abdominal wall, skin rash with pus discharge and hypoglycaemia. The association between late onset disease and neonatal septicaemia could partly be related to passive acquisition of pathogenic Staphylococcus aureus from adult carriers like health workers and relatives at home.All neonates more than 8 days old had been staying at home with the caretakers and the majority (70.9%) had Staphylococcus aureus isolated in their blood cultures.These findings are supported by results of Ako - Nai et al15 that demonstrated that carriage of pathogenic Staphylococcus aureus in the anterior nares of adult caretakers was associated with passive acquisition of the organism by the babies attended to. Contact of the brittle skin of the baby and/or the raw surface of the umbilical stump by pathogenic organisms enables access of the bacteria into the blood stream leading to septicaemia.This is possibly why these two conditions had a significant relationship with occurrence of neonatal septicaemia. In Nigeria, Ako - Nai et al10 found Staphlococcus aureus to be responsible for 71% of total isolates from skin sores in neonates with septicaemia. Hypoglycaemia was strongly associated with occurrence of neonatal septicaemia (p < 0.01). In Harare Hospital, Nathoo et al4 found hypoglycaemia to be one of the common findings in babies with sepsis. Neonates with septicaemia become hypoglycaemic because of increased metabolic demand due to the infection, inadequate breast-feeding by the affected babies and their poor glycogen stores in the liver20. A history of convulsions was significantly associated with occurrence of neonatal septicaemia (p < 0.01). Convulsions can be due to septicaemia (with consequent pyogenic meningitis) or hypoglycaemia. Nathoo et al4 found no association between convulsions and bacteriologically confirmed septicaemia but there were only 7 with seizures in her study, compared to 24 in the current study. The only perinatal factor associated with neonatal septicaemia was lack of antenatal care by the mother. Mothers who fail to attend antenatal care are not screened for infection and other risk factors that in the end affect their babies.These mothers do not get health education regarding place of delivery and how to look after their babies. The overall mortality of 18.2% was similar to that found in Western Sweden by Tessin et al21. Although lower mortality rates have been reported in some studies 2, 22 –23 other researchers have reported higher figures for example, Nathoo et al4 in Harare (28.5%), Okolo et al 24 in Nigeria (30.6%), Friedman et al25 in the UK (26%) and Vesikari et al26 (23%) in Finland. The majority of the deaths 46 (84%) occurred in the first 2 days of admission; most of the neonates who died were less than 2 days old and had negative blood cultures. Although we were unable to do post mortem examinatios on these babies, birth trauma and/or asphyxia can not be fully ruled out as possible contributors to these deaths. In Mulago Hospital, Ondoa – Onama27 reported one death out of every ten neonates with lowApgar score. It should be noted that, among neonates less than 2 days old who died, 10 (83%) had negative blood cultures and were recruited via SCU whereas 2 (16.7%) had positive cultures and were recruited via ACU. Conclusions S. aureus followed by E.coli predominate the aetiology of neonatal septicaemia in Mulago Hospital. Most deaths occur in the first 48 hours of admission and hypoglycaemia is significantly associated with death. References
Copyright © 2006 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs06028t3.jpg] [hs06028t1.jpg] [hs06028t4.jpg] [hs06028t5.jpg] [hs06028t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}