 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
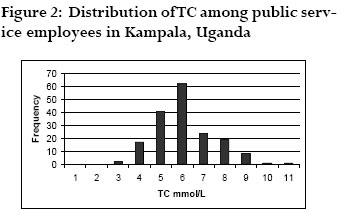
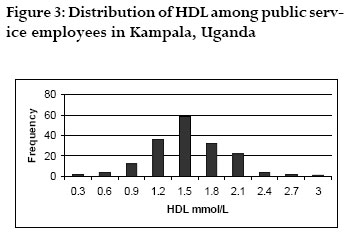
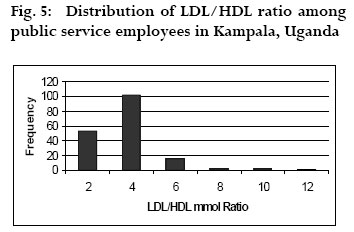
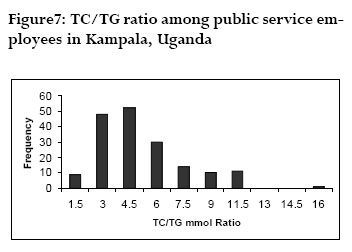
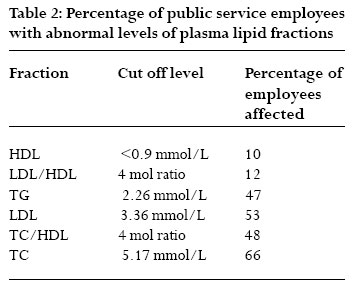
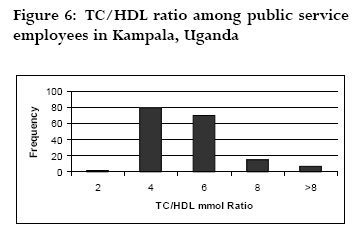
African Health Sciences, Vol. 6, No. 3, Sept, 2006, pp. 139-144 Plasma cholesterol and related lipid levels of seemingly healthy public service employees in Kampala, Uganda. Bimenya G. S. 1, Okot J. K. 2, Nangosa H. 2,Anguma S.A.2 and Byarugaba W. 1 1 Pathology Department, Faculty of Medicine, Makerere University, P. O. Box 7072, Kampala-Uganda Correspondence Author G. S. Bimenya Makerere University, Pathology Department, Faculty of Medicine, P. O. Box 7072, Kampala-Uganda Code Number: hs06032 Abstract Background: As Uganda’s economy improves, many people tend to adopt western diets and sedentary life styles that predispose tocardiovascular diseases including hypertension. These may be in silent danger without any typical symptoms to send early warningsignals. In Uganda, cardiovascular diseases (CVD) and diabetes mellitus are rapidly emerging as major causes of morbidity and mortality. Introduction Many epidemiological studies indicate that the incidence of coronary artery disease (CAD) is correlated positively with plasma concentration of TC, LDL, TG and negatively with high HDL 1, 2. Recent clinical trials repeatedly indicate that lowering of cholesterol reduces CAD3,4 risk in hypercholesterolaemic patients with and without CAD. Subsequently, guidelines for management of hypercholesterolaemia have been proposed in the US, Europe, Australia and Japan wherein patients are classified into lipid level strata for management 5. The World Health Organization (WHO) and the American National Cholesterol Education Programme recommended blood lipid and glucose concentrations shown in table 1 as cut-off points for patient management 6. As Uganda’s economy improves, many people adopt western diet and sedentary life styles that facilitate fat accumulation in blood predisposing to CVD. These people include middle and high-class managers in public service. As CVD may have no overt signs and symptoms, it was deemed important to spot check plasma lipid levels in blood samples from seemingly health public service employees in Kampala, Uganda to predict timely intervention. Methods The major expert panel on cholesterol education recommended testing for the total lipoprotein profile including HDL, LDL, and TG instead of merely measuring TC as the latter alone misses specific lipids and blood proteins that are becoming increasingly important in determining an individual’s particular risk for heart disease7 . Additionally, plasma lipid parameters must be evaluated not only for their absolute values as stratified in table 1, but also for their mutual ratios as expression of plasma lipid homeostasis8 One hundred and seventy four executives (85 males and 89 females) employed in public service in Kampala, Uganda, were investigated for plasma lipid levels after over night fasting. An explanation of the potential effects of dyslipidaemia was given to each participant who also consented that the biodata obtained be used for personal check up and educational purposes provided that the identities of individual and the employment firm were not divulged. It was also agreed that individuals found with risky results would be referred to appropriate physicians for treatment and management. Therefore the sampled executives were studied with their informed consent. The repertoire of lipids analyzed included TG,TC, HDL, and LDL. In the analytical procedures the substrate TG9, TC10, HDL11 or LDL12 is made to react under suitable conditions to produce hydrogen peroxide which when combined with a chromogen, a dye is produced. This dye absorbs photons at a given wave length in proportion to the concentration of the substrate13,14. From these measurements, the following molar ratios were derived: LDL/HDL, TC/HDL, and TC/TG. The results obtained were plotted in histograms and either parametric or nonparametric summary statistics were derived depending on the pattern of distribution15. Results This study therefore reports on lipoprotein profile embedded in TC, HDL, LDL and TG and in their mutual rations of LDL/HDL, TC/HDL, TG/HDL and TG/ HDL. (a) Triacylglycerols The distribution of TG concentration among the executives ranged from 0.38 to 5.62 mmol/L. The distribution was expectedly leptokurtic and positively skewed as shown in figure 1. Non parametric summary statistics were derived in mmol/L as median 1.42 and mode 0.73mmol/L giving a central 95th percentile range of 0.30 to 5.40 mmol/ L. (b) Total cholesterol The spread of TC portrayed in fig. 2 shows the typical near-Gaussian distribution which is slightly positively skewed. Summary parametric statistics in mmol/L include mean (SD) of 5.57 (1.33) and mean + 2SD range of 2.91-8.23 (c) High density lipoprotein cholesterol The distribution of HDL shown in figure 3 The distribution is near Gaussian with summary parametric statistics that include mean (SD) of 1.32 (0.43) and a range of mean +2SD of 0.51 to 2.23 mmol/ L. (d) Low density lipoprotein cholesterol The distribution of LDL ranged from 1.06 to 7.40 mmol/L as shown in figure 4. The distribution is near Gaussian. Hence, summary parametric statistics include mean (SD) of 3.38(1.16) and mean+2SD range of 1.06-5.7 mmol/L. (e) LDL/HDL ratio The distribution of LDL/HDL ratio ranged from 0.7 to 10.8 as displayed in fig. 5. The distribution of TC/HDL mol ratio is positively skewed with non parametric summary statistics of mode 3.06 and median of 4.17 . (g) TC/TG ratio The distribution of TC/TG ratio is shown in fig. 7 The distribution appears unimodal and positively skewed with mode of 3.15 and median of 4.01 ratio Summary of findings The percentages of public service employees with abnormal levels of plasma lipid fractions are summarized in table 2. (Figure 6) Discussion This work provides preliminary data on public service employees as a group in Kampala, Uganda, to help make recommendations to the government and the public concerning preventive approaches to CVD. High Density Lipoprotein Cholesterol HDL is the smallest lipoprotein that transports cholesterol from extrahepatic tissues to the liver for excretion. This process is thought to be anti-athero genic and elevated HDL levels have been shown to confer a decreased risk of coronary heart disease on an individual. In this regard HDL is often referred to as the “Good Cholesterol”, and the higher the level of it, the better for the individual. Conversely, low levels of HDL are associated with higher incidence of CHD 16 Levels of HDL below 0.91 mmol/L are considered a major risk factor for CHD17. In this study 10% of the executives are at risk on account of low levels of HDL alone(table 1). Increased concentration of LDL are atherogenic18 whereas increased HDL is cardioprotective19. LDL/HDL ratio, like that of TC/ HDL, is a better predictor of CVD than any other single lipid marker 20 The best ratio of LDL/HDL is a value below 3 internationally21 but in this work 12% of our sample 21/174 have a ratio above 4 thereby disposing to CVD . Triacylglycerols, TG According to international classification of lipid and glucose profile shown in table 2, the desirable levels of TG are those below 2.26 mmol/L. In that case then 47% of our sample haveTG levels in the danger zone associated with heart disease, insulin resistance and diabetes. Evidence suggests that TG may be a major trouble maker for the heart because TG react with HDL in such a way that HDL levels fall as TG levels rise and it is well known that low levels of HDL are harmful to the heart. Besides, high TG levels pose other dangers regardless of cholesterol levels: TG may be responsible for blood clots that form and block arteries and high levels of TG are associated with the inflammatory response that can cause considerable damage to cells and tissues including the arteries7 Low density lipoprotein cholesterol (LDL) The primary villain in the cholesterol saga is LDL, the bad cholesterol, which transports about 75% of the body’s cholesterol to the body cells. It is normally harmless but when it is oxidized it penetrates and interacts with the walls of the artery, producing a harmful inflammatory response including plaques that lead to coronary artery occlusion. Oxidized LDL also reduces nitric oxide a chemical that relaxes blood vessels7. On international scene, LDL levels above 3.36 mmol/ L are a risk for CVD and in this regard 48% of subjects in this study risk CVD on account of high levels of LDL alone. Total cholesterol,TC Studies consistently report a higher risk for death from heart disease with high TC levels, the higher the greater risk, and in general every time a person’s TC level drops by a point, the risk of heart disease drops by 2% 7. The TC/HDL ratio is a better predictor of atherosclerosis and CVD than any other single lipid 20. People with increased TC/HDL ratio were shown to exhibit resistance to insulin stimulated disposal and to have higher blood pressure, increased TG concentration and hyperinsulinaemia: each of these factors being a part of the metabolic syndrome is an independent risk factor for CVD 22 As shown in table 2, the recommended levels of TC are those below 5.17 mmol/L which puts 66% of our subjects in danger zone. In combination with HDL, the effects TC get ameliorated and therefore a high TC/ HDL ratio spells danger for the individual. Internationally the aim is to keep TC/HDL less than 4 in which case only 47% of our sample 81/174 have desirable ratio of TC/HDL. Conversely, 53% of the public service-employees in this work risk CVD on account of high ratio of TC/HDL 22 TG/HDL ratio In line with Friedwald algorithm23, the TG/HDL ratio indicates the relative size of the LDL particles and their atherogenic potential in which low TG/HDL ratio indicates primarily large, non atherogenic particles whereas high TG/HDL ratio indicates a greater population of small, dense, pro-atherogenic LDL particles with which prospective studies indicate that TG/HDL ratio highly correlates with reduction in developing CVD. In addition,TG/HDL ratio positively correlates with insulin resistance and is used as a surrogate measure7. In this work as many as 68% of the executives have levels of TG/HDL ratio above 2 which is not only a risk factor for CVD but also a surrogate measure of insulin resistance, a harbinger to diabetes mellitus. High levels of TC and other lipid disorders can be genetic or associated with fatty diets, diseases such as hypothyroidism, Cushing’s syndrome or kidney failure, certain medications including contraceptive pills, corticosteriods, certain diuretics or beta-blockers and life style factors including habitual, excessive alcohol use and lack of exercise, leading to obesity7. The results obtained in this work are not surprising because of sedentary life style and western dietary habits adopted by well-earning executives. These habits are spreading in Africa and rising trends of CVD have been correspondingly reported in South Africa 24, in Tanzania 25and in Kenya 26 Steps that every one can take to improve cholesterol levels and help prevent heart disease and heart attack include: foods low in saturated fat, exercising regularly, losing weight if one is over weight, and routine health check-ups including cholesterol screening. Many drugs such as statins, acid resins, fibrates and nicotinic acid are available to help lower blood cholesterol levels. They work in different ways with some better at lowering the bad cholesterol, LDL, some better at lowering TG , and yet others help raise the good cholesterol, HDL. None the less, it is important to emphasize that cholesterol-lowering medications are used along with healthy style habits. Drugs are not a substitute for healhy diet and life syle7 Therefore, urgent intervention measures targeting diet and lifestyles are required by the individuals and the government. In other countries like Japan, the United Kingdom,Australia and USA national cholesterol awareness programs are in place and involve routine body exercise, selective diets and lipid lowering drugs to the effect that CVD death rates have decreased as much as 60%27,8 Conclusion In all the 7 cut off points used, each analyte had a significant percentage of public service employees at risk of CVD. It is therefore concluded that hypercholesterolemia and other dyslipidemias exist among urban, seemingly healthy, Ugandan public service employees and this urgently needs intervention at the individual and national level. Recommendation Further studies depicting larger scope of the population, detailed holistic and stratified designs are needed. Preventive and corrective intervention involving reformed diets, physical activity life style, sports and appropriate drug use should be instituted. National cholesterol awareness programmes should be effected. References
Copyright © 2006 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs06032f7.jpg] [hs06032f6.jpg] [hs06032f3.jpg] [hs06032t2.jpg] [hs06032f5.jpg] [hs06032f4.jpg] [hs06032t1.jpg] [hs06032f1.jpg] [hs06032f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}