 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
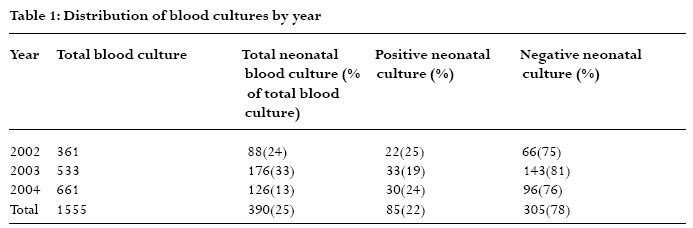
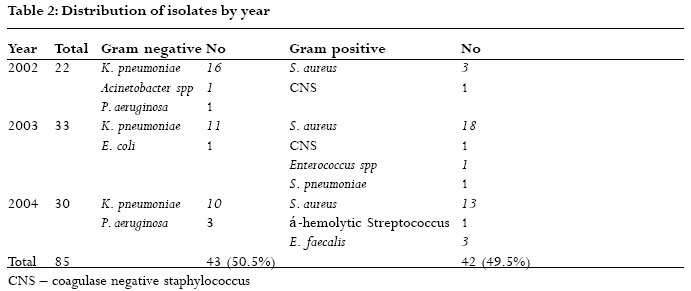
African Health Sciences, Vol. 6, No. 3, Sept, 2006, pp. 151-154 Bacteriological profile of neonatal septicaemia in a tertiary hospital in Nigeria Kenneth C. Iregbu1, OlufumilayoY. Elegba2, Iretiola B. Babaniyi3 1 Department of Clinical Microbiology & Parasitology, National Hospital, Plot 132 Central Business District,P.M.B. 425 Garki,Abuja, Nigeria. Corresponding Author: Kenneth C. Iregbu Department of Clinical Microbiology & Parasitology, National Hospital, Plot 132 Central Business District P.M.B. 425 Garki, Abuja, Nigeria. 900001 Email: keniregbu@yahoo.co.uk Phone: 234 805 493 2992, 804 410 6878 Code Number: hs06034 Abstract Background: Neonatal septicaemia is an important cause of morbidity and mortality. Knowledge of the bacteriological profile of the aetiologic agents is very important and helps to reduce the associated mortality in neonatal septicaemia. Key words: Neonates, Septicaemia,Antibiotic susceptibility, Nigeria Introduction Neonatal septicaemia describes any systemic bacterial infection in neonates documented by a positive blood culture 1. It is an important cause of morbidity and mortality among neonates generally1,2,3,4. Neonatal blood culture positive rates ranging from 25 – 54% in previous studies carried out within and outside Nigeria have been documented3,4,5,6. The gold standard for diagnosis of septicaemia is the isolation of the bacterial agent from a blood culture5. Both gram negative and positive bacteria have been isolated from blood, and predominance of one type over the other varies from place to place and even in the same place over time1-7. Bacteria commonly isolated in the samples included Klebsiella pneumoniae, Escherichia coli, Enterobacter species, Pseudomonas aeruginosa andStaphylococcus aureus. Similarly the studies showed that the susceptibility of the isolates to the different antibiotics varied from one place to another and over time in the same place. As neonatal septicaemia is a life threatening emergency and delays in diagnosis and treatment with appropriate antibiotics may have devastating consequences, surveillance is needed to identify the common pathogens of the disease as well as the antibiotic susceptibility profile of the pathogens in a particular area. This study was designed to evaluate the common pathogens associated with neonatal septicemia seen in our hospital and their antibiotic susceptibility pattern over a 3-year period covering 2002 – 2004. The result of the study is expected to guide therapy and also influence infection control practices and rational antibiotics use. Methods This is a retrospective review of the report of all neonatal (28 days and below) blood cultures carried out in the Department of Clinical Microbiology & Parasitology laboratory of the National Hospital,Abuja, Nigeria from January 2002 to December 2004. The clinical impression or suspicion of neonatal septicaemia was made by the caring Paediatricians. Blood culture samples were aseptically collected by the doctors into the Oxoid signal blood culture broth (Oxoid. Basingstoke UK). These were sent to the laboratory where they were handled according to the manufacturers specifications. Bottles showing evidence of growth after incubation at 37oC were promptly sub-cultured into MacConkey, Blood and chocolate agar media and incubated in appropriate temperature and atmospheres according to established methods [8,9] The aerobic isolates were identified by Gram’s staining, colony characteristics and biochemical properties as previously established [8,9]. No anaerobes were isolated. The antibiotic sensitivity tests were carried out by disk diffusion method in accordance with NCCLS criteria and similarly interpreted [10,11]. Escherichia coli ATTC 25922, Staphylococcus aureus ATTC 25923 Pseudomonas aeruginosa ATTC 27853, Enterococcus faecalis ATTC 2921 and Streptococcus pneumoniae ATTC 49619 were used as controls. Results There were a total of 390 neonatal blood cultures out of the 1,555 received in the laboratory during the reviewed period. This constituted 25% of all blood cultures. Of the neonatal blood cultures 85 (22%) were positive for bacterial growth while 305 (78%) yielded no growth (Table 1). It is shown in Table 2 that 43 (50.5%) of the 85 bacterial growths were gram negative bacilli (GNB) while 42 (49.5%) were gram positive cocci (GPC). 86% of the GNB were Klebsiella pneumoniae thus making it the predominant GNB. Pseudomonas aeruginosa constituted only 9% while Escherichia coli and Acinetobacter species made up 2.5% each of the GNB. Staphylococcus aureus made up 34 (81%) of the GPC while Enterococcus faecalis, coagulase negative staphylococcus (CNS) and Streptococcus pneumoniae constituted 9.5%, 4.7% and 2.4% respectively. Eighty nine percent of the Staphylococcus aureus were sensitive to amoxicillin-clavulanic acid while 85%, 45%, 71% and 64% were sensitive to cefuroxime, ciprofloxacin, chloramphenicol and erythromycin respectively (Table 3). The only three isolates tested against tetracycline were all susceptible to the drug. Penicillin resistance was 90%. Resistance to ceftazidime, ceftriaxone and gentamicin were 71%, 64% and 60% respectively. The resistance of the isolated Klebsiella pneumoniae to ceftazidime, ceftriaxone and cefotaxime were 85%, 87.5% and 94% respectively (Table 3). Resistance to amoxicillin and ampicillin-sulbactam was 100%, and 85% for amoxicillin-clavulanic acid. All (100%) of the Klebsiella pneumoniae isolates tested against imipenem were susceptible while 75% were susceptible to amikacin. Also all the isolates tested against ofloxacin and norfloxacin were sensitive but the number of isolates were small. Discussion The proportion of positive blood cultures in the study is slightly lower than the lower range recorded in previous studies3-5. This could be as a result of good infection control practices or the common habit of collecting blood samples after antimicrobials have been commenced contrary to established standards for blood culture12. Records showed that 19% of the neonates had been on antibiotics before blood sample were taken for cultures. Over dilution of the little blood from neonates in the large adult broth bottles may also have hindered some growths. Although previous studies have found the predominance of either GNB or GPC over the other we found these two groups of bacteria isolated in almost equal proportions in our hospital. Klebsiella pneumoniae and Staphylococcus aureus were the predominant GNB and GPC respectively. These findings have implications for therapy and infection control. Empiric therapy for suspected neonatal septicaemia must therefore cover both GPC and GNB particularly Klebsiella pneumoniae and Staphylococcus aureus. Klebsiella pneumoniae and Pseudomonas aeruginosa (both making up 95% of all GNB) and S. aureus can survive in the environment for a relatively long time and fairly widely distributed in the hospital environment, and therefore have the potential for being transmitted from the environment to the patients through practices that breach infection control measures. This emphasises the need for the establishment of effective and functional infection control programmes in hospitals. The most worrisome and significant finding of this study was that 50-100% of the Klebsiella pneumoniae isolates were resistant to commonly used antibiotics especially gentamicin and the second and third generation cephalosporins. Though not tested routinely in our laboratory it is obvious from their resistance pattern to the third generation cephalosporins that the Klebsiella pneumoniae isolates were mostly extended spectrum betalactamase (ESBL) producers. It would therefore appear that the choice of drug for empiric treatment of suspected neonatal septicaemia is likely to be difficult particularly in the presence of ESBL producers which often fail to achieve therapeutic goals even after showing in vitro susceptibility.The solution will lie with institutionalization of sustainable antibiotic susceptibility surveillance and routine testing for ESBL production in isolates known to elaborate the enzyme especially Klebsiella pneumoniae and Escherichiacoli [13].The 100% sensitivity of Klebsiella pneumoniae to imipenem obviously indicates the absence of selective pressure since the drug is rarely prescribed, and even at that can only be dispensed on the approval of the Clinical Microbiology Department based on laboratory evidence. However, based on the result of this study imipenem (which is also effective against S. aureus, though not routinely tested in our laboratory) may be recommended in the absence of less toxic drugs as first choice drug for the empiric treatment of neonatal septicaemia in the neonatal unit.Therapy will need to be modified appropriately as soon the result of sensitivity testing is available.The number of Pseudomonas aeruginosa isolates tested against gentamicin, ciprofloxacin and ceftazidime is too small to warrant any reasonable conclusion. A well designed surveillance study is required to determine the true susceptibility profile of Pseudomonas aeruginosa and other GNB. Between 71% and 89% of the entire isolated S. aureus were sensitive to chloramphenicol, ciprofloxacin, cefuroxime and amoxicillin-clavulanic acid, implying that none of these drugs is absolutely suitable for empiric therapy. Similarly gentamicin which is routinely used synergistically with a beta-lactam for therapy in cases of Staphylococcus blood stream infection (BSI) has high resistance profile to Staphylococcus aureus. This will certainly pose a management dilemma for clinicians as well as a challenge to Clinical Microbiologists to determine other therapeutic options especially in environments where vancomycin and other novel anti-staphylococcus drugs are unavailable.Tetracycline is one of the drugs almost declared ineffective against Staphylococcus aureus, but the sensitivity of the three isolates tested probably indicates a renewed sensitivity and will need to be well evaluated in a further study. Most of the neonatal infections seen in this study were hospital acquired.The result of an outbreak of Klebsiella pneumonia septicaemia in the hospital in 2002 (unpublished) revealed that the hands of staff were the major routes of spread.We therefore, conclude that an effective infection control programme which will among others ensure good and effective hand washing, regular antibiotic susceptibility surveillance and evaluation, and the enforcement and periodic review of the antibiotic policy of the hospital as well as the encouragement of rational antibiotic use will reduce the rates of acquiring nosocomial infections and development of bacterial resistance. References
Copyright © 2006 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs06034t1.jpg] [hs06034t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}