 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 6, No. 4, Dec, 2006, pp. 207-214 Postpartum major depression at six weeks in primary health care: prevalence and associated factors. Juliet. E.M. Nakku1, Grace Nakasi1, Florence Mirembe2 1 Department of Psychiatry,Faculty of Medicine, Makerere University2 Department of Obstetrics & Gynaecology,Faculty of Medicine, Makerere University Code Number: hs06047 Abstract Background: Major depression is a common and disabling complication of the postpartum period in women. It is thought to occur three times more commonly in the developing than in developed countries. Objectives: The objectives of this study were to determine the prevalence of and factors associated with major depression among women attending a peri-urban primary health care unit in Kampala, Uganda, at six weeks postpartum. Introduction Postpartum psychiatric disorders refer to those mental disturbances, which occur in women of childbearing age within four weeks of childbirth 1. Postpartum psychiatric illness can cause considerable family vulnerability and distress and impairs a woman’s ability to carry out her normal tasks and cope with the care of her baby 2, 3. Postpartum depression, which is often not recognized by primary health care providers, has been associated with disturbances in the mother-infant relationship and bonding 4 and in the child’s cognitive and emotional development 5, 6, 7. Prevalence rates for postpartum major depression vary widely from place to place. Studies in the Western countries report prevalence rates of 10% or more for postpartum major depression34. In Non-Western countries the figures are variable. The disorder is thought to occur three times more commonly in the developing than in developed countries 8 and to represent a considerable public health problem affecting women and their families 2, 8, 9. In China, Lee et al found major depression to occur in 5.5% of women six weeks postpartum using the structured clinical interview for DSM-111 R33. In a peri-urban population of Khayelitsha, Cape town in South Africa on the other hand, the prevalence rate of DSM-IV major depression was reported to be 34.7% at two months postpartum8. Other African studies that have looked at postpartum women have dealt with the prevalence of psychological distress in general rather than focused on major depresion31,32 . These studies have also used screening instruments that do not give strict diagnostic categorization of major depression but rather measure individual symptoms. Few studies in Uganda have looked at depression in postpartum women. In Uganda, Assael et al 10 found 16% of a sample of semi rural women in a small village of Kasangati, to be depressed after delivery. Cox 11 in a similar population found 10% of his sample to have depression following delivery. These studies in Uganda had a more rural setting and were done more than two decades ago. Although earlier writers suggested a greater likelihood of postpartum depression among deprived, particularly inner city dwellers, not much work has been done on this subject in urban settings in Africa. Multiple risk factors for postpartum depressionhave been suggested to be associated with postpartum psychiatric illnesses. Personal vulnerability, personality traits 12 and social factors such as unplanned pregnancy, occupational instability, unemployment of the woman or her partner and low income 6, 13, 14, 15, 16, have been cited. Other workers have reported family factors such as single parenthood, marital discord, divorce and polygamy 13, 14, 17. Life events, particularly those that have occurred in the year immediately before the birth, and those that were undesirable or had a negative impact have also been cited 3, 14, 17. Other social factors suggested include poor social support, from the father of the child or the woman’s own mother 6, 14. The African extended family system with its prescribed protection of the new mother has been reported to be preventive of postpartum psychiatric disorders especially depression 18. In their study, O’Hara & Swain 14 found that the availability of a housemaid to the puerperal woman was also associated with low rates of puerperal depression. Other factors thought to put women at risk of depression in the postpartum period include hormonal factors and baby factors such as low birth weight 16, 19 , infant ill health, birth abnormalities 17, female sex 20, and absence of breast-feeding 13. While prime-gravidity has been strongly associated with postpartum depression by some researchers 13, 17, others have found women in their third pregnancy to be more likely to become depressed 2, 20.This was attributed to the cumulative strain of bringing up young children particularly if the mother should be unwell or predisposed to mental illness. It is evident therefore that little attention has been paid to severe depression in the postpartum period in Africa and Uganda in Particular. Recent studies on postpartum depression in Uganda are lacking and the current situation in our rapidly changing society is unknown. OBJECTIVES:
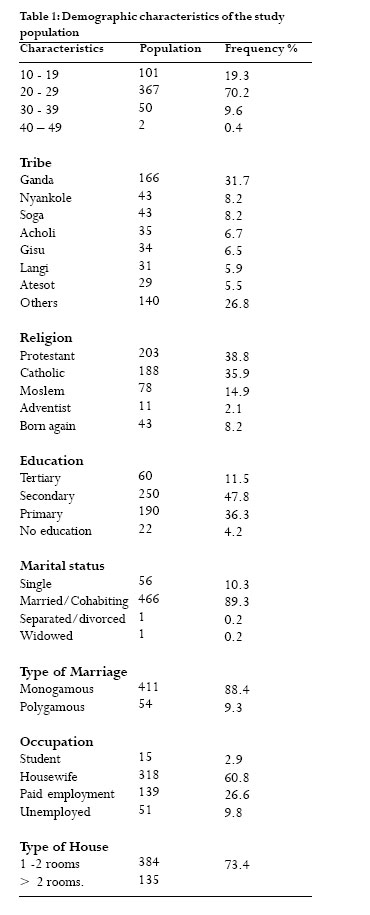
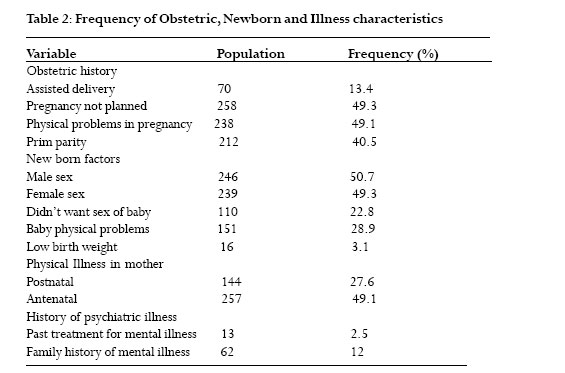
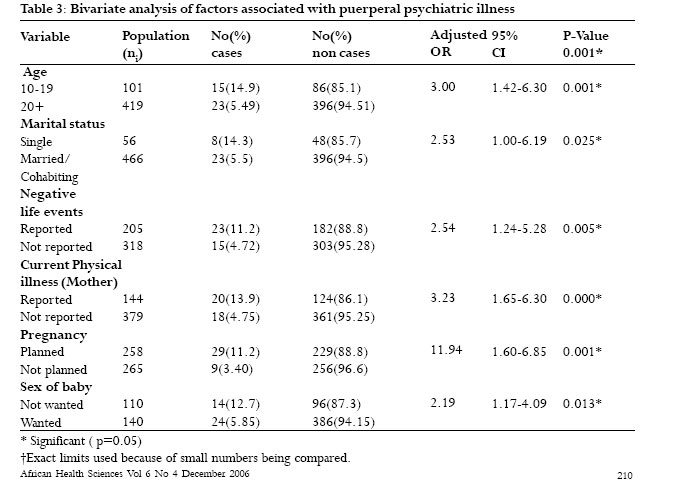
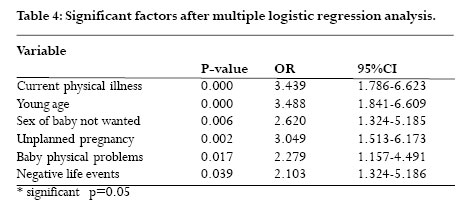
Method A cross sectional descriptive and analytical study was carried out in a peri-urban primary health care center in the outskirts of Kampala, the capital city of Uganda.This is a mini hospital with antenatal and postnatal services as well as a theater. The center is run by a consultant obstetrician and a number of nurses and mid wives. Women attending for out patient postnatal services were consecutively recruited between September 2002 and January 2003. Only those women who had delivered 6 weeks previously and gave informed consent were included in the study. Before questionnaires were administered to any eligible woman the later was provided with a consent form to sign or thumbprint after the study was explained to them in detail by the research assistant. Non-consent or a choice to withdraw from the study would not deter any participant from accessing needed medical or psychological care.All study participants that were found to have depression had a detailed assessment by a psychiatrist (one of the authors) and were offered free appropriate intervention. Instruments The instruments used included a social demographic, a screening (25-item Self reporting questionnaire- SRQ25), and a diagnostic (Mini International Neuropsychiatric Interview – MINI) questionnaire.The SRQ25 has been validated in a primary health care setting in Nigeria, where a cut off of 5/6 was established21. It screens for psychological distress. This instrument was selected because of its ease of use and its previous use in similar settings to those in this study. The MINI is a diagnostic instrument based on the Diagnostic and Statistical Manual of mental disorders1. It gives a set of criteria on which to base a psychiatric diagnostic category and is easy to administer even by non-psychiatric interviewers.The major depression module was used. All questionnaires had been independently translated and back translated to and from Luganda, the language commonly spoken in the area of study, by two bilingual clinical psychologists in the Makerere University’s Department of Psychiatry. All questionnaires were pre-tested in a week long intensive training of the research assistant and revisions made as necessary to improve on contextual validity. Permission had been obtained from the Faculty of medicine and district review boards prior to carrying out this study. Measurements The social demographic questionnaire was administered consecutively to women attending the postnatal service. In addition to social demographic characteristics, this questionnaire asked about negative life events in the previous 12 months, obstetric factors, physical illness and medications taken during pregnancy and after delivery. Other variables included past individual and family history of psychiatric illness, substance dependence, respondents’ relationship with father of child and with their own mother.The sex and health of the newborn baby was also asked about.All respondents were then screened for psychological distress using the SRQ-25 and also had a full general physical examination by the research assistant (a doctor). Any respondents in this study who scored above a cut off of five were taken as having probable psychiatric disorder and was subjected to the major depression module of the M.I.N.I to confirm major depression. Interviewer administered questionnaires were used to cater for those women with minimal education as well. The research assistant who administered the questionnaires had been a junior house officer on the psychiatry ward and had significant experience in psychiatry.All questionnaires were checked at the end of each day by the principal investigator for missing or wrong data before being locked up in a secure cupboard and later processed. Data was entered into Epi-Info version 6.0 and transferred to SPSS version 10 for cleaning and analysis. Frequencies were generated, variables were compared and tests of significance carried out using chi-square for categorical variables.A multivariate analysis was done to find correlation between the outcome variable of puerperal depression and the independent variables. A p-value of 0.05 was taken as significant. Results Sample Characteristics Five hundred and fourty four women were included in the study and the response rate was 100 percent. Only 523 women were included in the analysis. Twenty one were excluded because of incomplete data. The social demographic characteristics of the study population are shown in Table 1.The mean age of the sample was 23.4 years (SD+/- 4.76). Most women had at least some secondary education (n=310, 59.4%). The size of house lived in by the women and their families was used as a proxy measure of their social economic status, rated as low if the house was one to two rooms and high if it was three rooms or more. Table 2 shows the obstetric, newborn and illness characteristics of the population. Less than half (n=212, 40.5%) were primi-parous. Multi- parous was taken to mean having had two or more pregnancies ending in a live birth after 28 weeks gestation. Previous treatment for any mental illness was reported in 2.5 % while family history of mental illness was reported in 12.2 % of the study subjects. Prevalence Of the 523 women studied 38 (7.3%) were found to have SRQ score of >5 signifying psychiatric distress or possible psychiatric disorder. All the 38 women completed the M.I.N.I. for diagnosis of major depressive disorder. Thirty two of these women met criteria for major depressive episode constituting a prevalence rate of 6.1% for major depression at six weeks postpartum. Of those women with major depression seven (18.4%) had suicidal thoughts. Two of them had previous history of suicide attempt and were rated as high risk while 5 had suicide ideation without previous history of attempts and were rated as low risk. Correlates of postpartum major depression A bivariate analysis (Table 3) showed that being aged 10- 19 years (p<0.001; OR=3.0; 95% CI=1.42-6.30), being single (p<0.025; OR=2.53; 95%CI=1.00-6.19) and having had an unplanned pregnancy (p<0.001; OR=0.3; 95% CI=0.15-0.63), were significantly associated with postpartum major depression. Other significant correlates included undesired gender of baby (p=0.05; OR=0.41; 95% CI=0.19-0.88) physical problems in the baby (p<0.01; OR=2.69; 95%CI=1.29-5.63 and in the mother (p<0.001; OR=3.23; 95% CI=1.65- 6.30), and having had an adverse life event in the year prior to having a baby (p<0.01; OR=2.54; 95% CI=1.24-5.28). Further analysis however, using Multiple logistic regression (Table 4) excluded being single as a significant factor but physical problems in the mother and newborn as well as unwanted pregnancy, adverse life events and being aged 10-19 years remained significantly associated with postpartum depression. Discussion This study found the prevalence of major depressive disorder at six weeks postpartum to be 6.1% a figure lower than the 10% quoted by previous studies in Uganda6,11. Our figure is also very far below the 34.7% prevalence reported in a South African peri-urban population of postpartum women The reasons for these differences may be methodological due to different study designs and instruments used, but most important is that they measure different parameters. Some studies have included women up to 3 months postpartum using ratings of individual symptoms6, 11 rather than requiring the presence of the whole clinical syndrome of depression as laid out in DSM IV.This study established major depressive disorder among women in the early postpartum period (6 weeks) that met five or more DSM IV diagnostic criteria for the disorder. The instrument used in this study (M.I.N.I) was more stringent and may not have been sensitive to the milder forms of depression, described by less than five of the nine symptoms that characterize depression in DSM-IV. The result obtained are similar to the prevalence of 5.5% obtained by Lee et al33 that looked at depression among Chinese women using the DSM III R. Although up to three quarters of the women with postpartum depression will have an onset within 4 weeks 24 after delivery, many women not identified as ill in our Ugandan study could have had evolving symptoms, which would be picked up if interviewed weeks later. Depression after childbirth has been found to peak around the third month 16. Further still the prevalence obtained in this study could be an under estimate since 9 in 10 women in Uganda have been found not to attend postnatal clinics particularly if they are young, single or uneducated7. Correlates of postpartum major depression Social demographics All participants belonged to the peri-urban community living around the study site.That the Ganda tribe formed the largest group of respondents was expected since the study site is situated in Buganda region where the Ganda are the indigenous and the majority. The percentage of the respondents who attended at least some secondary school (59.4%) reflects the relatively high female literacy level in Uganda rated at 53% 25.The low social economic status found in the majority of respondents (73.4%) only reflected the type of population found in Kampala’s peri– urban population. Despite previous belief that social adversity particularly in inner city dwellers is associated with puerperal mental illness, low social economic status in this study was not significantly associated with major postpartum depression. There may have been a disproportionate selection of low social class respondents because they are more likely to use the free public health facilities than their counterparts who can pay for private facilities. Over 80% of the study population were married which is not unexpected in the Ugandan population where women are expected to marry early, usually in their teens or early adulthood As other studies have suggested, those women who had psychiatric disorder were significantly younger and more likely to be adolescents15. Being young and having to meet with the demands of a new mother is likely to be associated with significant stress owing to poorly developed coping mechanisms and to lead to mental ill health. Life Events Negative life events were significantly associated with major postpartum depression in this study. Death, particularly in the immediate family is the event that was mentioned most frequently (49.5%). Negative life events that occurred in the previous one year have been associated with post partum depression by a number of researchers. 26, 27, 28 . In fact Paykel et al 3 found life events to be the most powerful predictor of puerperal psychiatric illness and other factors like marital problems to be significant only in the presence of other significant life events. Earlier researchers on life events proposed that losses were more significantly associated with psychiatric illness especially depression 29. The loss of a job did not feature very frequently among the life events because many women were housewives and not in paid employment. In the African setting often women are expected to stay at home. Sickness in the family was reported in about a quarter of the respondents (26.5%). In a population where women are the primary careers for the sick and dying, the stress associated with this long term responsibility together with looking after a new born may be the cause of a feeling of entrapment and partly responsible for psychiatric disorder in the study group.That bereavement was reported in about half the respondents is not surprising in an era in Uganda where nearly every family has experienced death of at least one relative due to the Human Immuno-deficiency Virus (HIV). The significance of illness or death in the family specifically due to HIV/AIDS as the cause of postpartum major depression was not the focus of this study, but would be interesting to examine in a follow-up study. These findings support the idea that psychosocial factors particularly bereavement may have a big role to play in the causation of postpartum major depression. Obstetric and newborn factors Previous researchers have not reached consensus on whether obstetric factors are correlated with puerperal psychiatric morbidity or not 26, 27 30. This study showed no correlation between postpartum major depression and obstetric complications. However, unplanned pregnancy and baby characteristics were significantly associated with postpartum depression. Women whose newborn babies had physical illness were more likely to be depressed than not. This could be due to the uncertainty about the survival of the newborn and doubts about ones capacity to cope with the care of an abnormal or ill newborn child. It is important to note that depressed or anxious women may have exaggerated pessimistic concern about the health of their newborn compared with those women who are psychologically well. This might be the case in this study where it was found that the children reported to be ill had mild forms of illness such as cough and cold that were not sufficient to explain the mother’s clinical psychiatric illness. There was no statistically significant difference between women who had male and female babies when those who reported ‘unwanted sex’ of baby were compared.The reasons therefore, for this response was not clear from this study although one would have expected overall preference of the male child in this patrilineal society where the issue of an heir is considered of great importance. Physical illness in the woman at six weeks was found to be positively associated with postpartum major depression.The illness, however was mostly of a minor and transient nature, which even though could have caused a dysphoric mood would not be deemed sufficient to cause full blown clinical psychiatric disorders. It might be considered that an already existing depression or anxiety may have increased the woman’s sensitivity to physical discomfort compared with her counterpart without psychiatric disorder. In an earlier Ugandan study on postpartum depression among rural women11, unplanned pregnancy did not featured as an important factor. It was believed then that this might be because in African cultures child bearing was so widely desirable that issues of whether a baby was wanted never arose. This peri-urban study however shows a trend similar to that shown in the Peri-Urban settlement in South Africa8 in which there was association between unplanned pregnancy and postpartum major depression. This may suggest that the meaning of pregnancy to an urban and rural woman in Uganda may be different. The study was not without limitations.The fact that it was health center based may have determined a highly selected group of respondents. It may therefore be difficult to generalize the findings to the total Ugandan population of childbearing women. The crossectional design may have eliminated respondents that would otherwise be picked up in a prospective study, more so since most women in Uganda do not attend postnatal clinics. The crossectional design of this study further makes it impossible to prove the causal relationship between major puerperal depression and the factors found to be correlated with it. Bigger numbers of respondents would have improved the statistical significance of the results. Conclusion The prevalence of postpartum major depression was found to be 6.1 % in a peri-urban primary care center population of childbearing women in Uganda. Social factors predominated in being correlated with puerperal psychiatric disorder.These included young age especially adolescence, being single, having unwanted pregnancy and having had a negative life event in the year prior to childbirth. Physical illness, even minor illness in the newborn and in the mother at six weeks postpartum may also make a woman more vulnerable to depression. This study has both clinical and research implications. Clinically, the highlighted importance of psychosocial factors and social support to a new mother calls for consideration of these factors during the designing of antenatal and postnatal care plans. Also the role of domiciliary visits to new mothers cannot be over emphasized especially in a setting where most women will not or cannot attend the regular antenatal or post natal clinics even within their community. The findings of this study may form the basis for screening women for risk of psychiatric disorder in the postpartum period to prevent disabling morbidity and suicide in young mothers. For this research, there is need for a prospective study to establish the actual prevalence of postpartum major depression in the general population of childbearing women in Uganda. The study would also further analyze the relationship between postpartum major depression and the various factors within the woman’s environment.The role of HIV/AIDS infection in the postpartum woman or her close family in the incidence of postpartum major depression needs to be studied as well. Acknowledgements We acknowledge Dr. Joshua Tugumisirize and Dr. Seggane Musisi of the Department of Psychiatry, Makerere University Medical School, Kampala, Uganda and Dr. Nick Kates of the McMaster University, Ontario, Canada for the valuable comments on this paper during its preparation.We thank our anonymous reviewers for their time and comments. We thank Mr. Albert Maganda of the Case Western Reserve University for his help with the statistics and Ms Gertrude Nansimbe for typing the initial draft of this paper. Our thanks also go to the management and staff of Naguru health center for allowing this study to take place and for supporting the data collection. Our special thanks go to the management of the Health Sector Strategic Plan Project of the Ministry of Health for funding the study. References
Copyright © 2006 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs06047t1.jpg] [hs06047t3.jpg] [hs06047t2.jpg] [hs06047t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}