 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
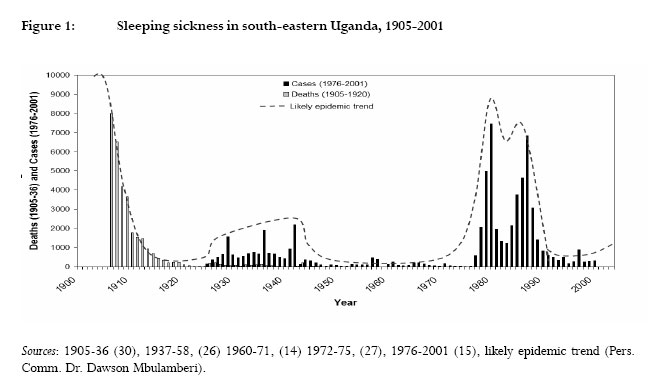
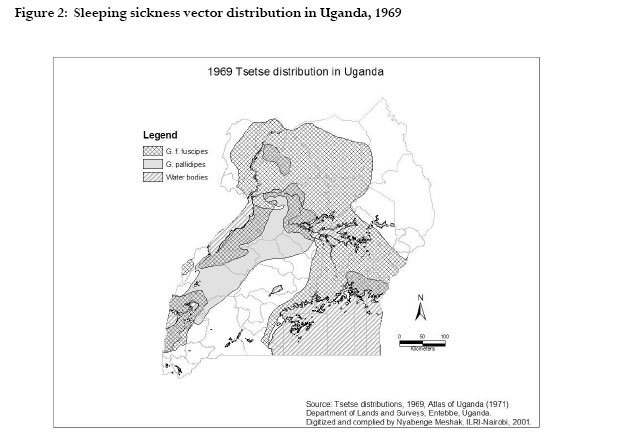
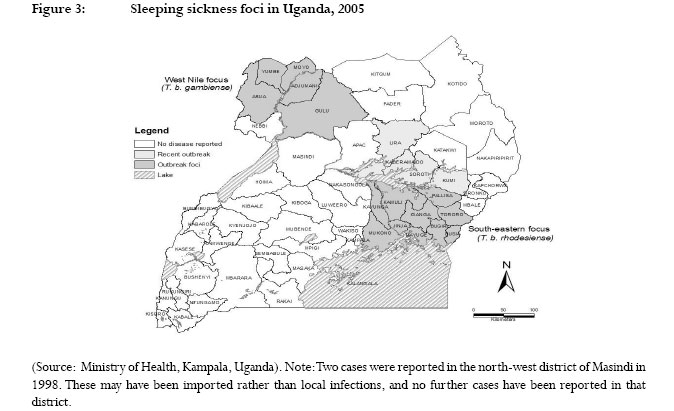
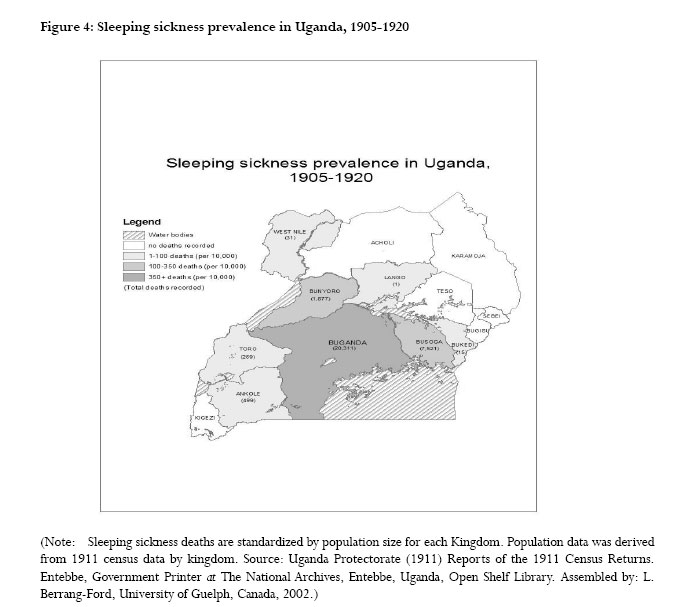
African Health Sciences, Vol. 6, No. 4, Dec, 2006, pp. 223-231 Sleeping sickness in Uganda: revisiting current and historical distributions Lea Berrang-Ford1, Martin Odiit2, Faustin Maiso3, David Waltner-Toews1, John McDermott1,4 1 Department of Population Medicine, University of Guelph, Canada, 2 Ministry of Health, Kampala, Uganda, 3 World Health Organization, Kampala, Uganda, 4 International Livestock Research Institute (ILRI), Nairobi, Kenya Correspondence Lea Berrang Ford 233 Curzon Ave. Saint Lambert, QC, J4P 2V3 Canada Email: LeaBerrang@hotmail.com Code Number: hs06049 Abstract Background: Sleeping sickness is a parasitic, vector-borne disease, carried by the tsetse fly and prevalent in sub-Saharan Africa.The disease continues to pose a public health burden in Uganda, which experienced a widespread outbreak in 1900-1920, and a more recent outbreak in 1976-1989.The disease continues to spread to uninfected districts. Introduction Sleeping sickness, or human African trypanosomiasis, is a vector-borne parasitic disease prevalent in sub-Saharan Africa. Caused by the parasite Trypanosoma brucei, and transmitted by an infected tsetse fly (Glossina spp.), trypanosomes also cause disease in livestock and other wild animals. There are two subspecies of T. brucei that cause sleeping sickness. T. b. gambiense causes a more chronic form of sleeping sickness and is prevalent predominantly in west/ central Africa and southern Sudan. T. b. rhodesiense causes a more acute form of the disease and is predominant in east and southern Africa. Sleeping sickness has continued to be a significant public health burden in Uganda since its identification in 1898.1, 2 In Uganda, both forms of sleeping sickness are present, with the chronic form, T. b. gambiense, currently found in the north-western and West Nile region, and the more acute, T. b. rhodesiense, more prevalent in the east. As such, Uganda forms the African boundary of the two forms of sleeping sickness. Recently, evidence of disease spread to districts considered to be previously uninfected3 has highlighted the need for increased understanding and implementation of disease prevention and control. The spread of disease foci is of particular concern in Uganda, where there is significant risk of the two sleeping sickness subspecies merging in the socially unstable north-central districts 4. Sleeping sickness was first identified and characterized in southern and eastern Africa in the last few years of the 19th century, a period that coincided with a widespread and severe epidemic of the disease in Uganda. This early epidemic was originally characterized as T. b. gambiense; extensive debate, however, has challenged this conclusion, arguing that the causative agent was likely T. b. rhodesience5-7 , though no clear consensus has been established8 . Between approximately 1900 and 1920, Uganda experienced one of the severest epidemics of sleeping sickness ever recorded. Focused in the Buganda region along the shores of Lake Victoria and its drainage rivers, more than 200,000 people are believed to have died before the decline of the epidemic1. The colonial government of the time responded with a massive evacuation campaign of up to 24 km from the lakeshore area1. This early epidemic has been associated with a range of causal factors, including eco-social imbalance caused by colonial disruption9, a hut-tax system resulting in widespread movements of labourers 10, and changes in livestock populations following an 1889-1892 rinderpest outbreak8. These early outbreaks are attributed to transmission by the tsetse species, G. f. fuscipes, whose predominant habitat is riverine areas and gallery forests (1). Following the decline of the 1900-1920 outbreak, sporadic cases occurred, with smaller outbreaks recorded in the 1930s and 1940s (Figure 1). These outbreaks were confirmed to have been caused by T. b. rhodesiense, which was first described in 1910 11 . The vector for these 1930s and 1940s outbreaks was concluded to be G. pallidipes, a savannah species often associated with the distribution of animal hosts 1,12 . Following this period, disease persisted at low levels, with a continued focus in the lakeside region. In 1976, collapse of prevention and control measures associated with unstable socio-political conditions and agricultural change in Uganda contributed to a major outbreak in the south-east. This outbreak, identified as being predominantly transmitted by G. f. fuscipes, the riverine tsetse fly species, spread uncontrolled until political conditions favored re-establishment of public health services and basic control measures in the early to mid 1980s. This epidemic resulted in the spread of the parasite into Tororo District, previously unaffected. The epidemic declined in the 1990s in conjunction with increased stabilization of Uganda’s economic and political situation. Persistence of cases and spread into unaffected districts, however, has resulted in continued public health concern13 . Moreover, in the early 1980s it was discovered that sleeping sickness was not restricted to the south-east. Cases of T. b. gambiense were recorded in the West Nile region in north-western Uganda, and the outbreak persists in north-western districts into 2005. This epidemic in north-western Uganda has been associated with returning Ugandan refugees who had resided temporarily in infected areas of southern Sudan14. In 1998, cases of sleeping sickness began to be recorded in the central district of Soroti. These cases were associated with transmission of T. b. rhodesiense imported from the south-east via cattle movements3 . More recent disease spread includes outbreaks in Kumi Kaberamaido, and Lira13,15 Districts in 2004 and 2005. This expansion of the disease range exacerbates concern over the potential risk of the two sleeping sickness strains, T. b. gambiense in northeast and T. b. rhodesiense in the southeast, merging in north-central Uganda4, 16. Such a concern is compounded by reports of tsetse presence, cattle movements, rebel activity, internal displacement of large portions of the population, extensive poverty and civil conflict in central districts. Recent research in 2006 by Picozzi et al. showed that while the T. b. rhodesiense and T. b. gambiense foci remain discrete, there is now only 150 km between the ranges of the foci. Areas now infected by T. b. rhodesiense also now overlap with areas previously infected by T. b. gambiense in the 1950’s . The continued spread and shifting of the sleeping sickness distribution within Uganda and the potential for sub-species overlap highlight the need for increased understanding of disease dynamics and factors driving transmission. Currently, much focus is placed on current areas of infection, including the north-western (West Nile) and eastern foci. More recently, concern for central districts has shown that control and prevention cannot focus solely on currently infected regions. Sleeping sickness occurrence has been characterized by recurrence of outbreaks in historical sleeping sickness foci17 . These foci of re-occurrence have been observed across sub-Saharan Africa1, 18, 19, 20, 21 , including a recurrent focus in south and eastern Uganda14, 22 . These concerns over re-current foci and continued disease spread highlight the absence of adequate assessment of the differences between current and historical distributions of sleeping sickness. Given evidence of historical sleeping sickness foci14, 23, the factors that have affected changes in the distribution of sleeping sickness in the past are likely to have significant potential to affect changes in the distribution of sleeping sickness in the future.Thus, historical spatial information and archival data on the distribution of disease can be important in providing information on both potential reasons for changes in the distribution of sleeping sickness as well as future sleeping sickness risk. This paper aims, therefore, to compare and discuss the distributions of sleeping in Uganda for the 1900-1920 outbreak period and current disease foci, and to highlight information gaps and implications arising for future research, prevention and control. Methods Human population and vector distribution data Population census records for 1911 were extracted from original census archives for the Ugandan Protectorate. Summaries of the total population by Kingdom were used to standardize sleeping sickness death counts into prevalence values for comparison. Census records collected during the colonial period may be subject to significant bias due to differential reliability of population counts; this is particularly likely in remote northern districts of Uganda. Vector distribution data for 1969 were extracted from the Atlas of Uganda24 , and digitized by the International Livestock Research Institute (ILRI), in Nairobi, Kenya into distribution shapefiles in ArcView (ArcView 3.2, ESRI Systems, Redlands, CA, USA). Archival sleeping sickness records Sleeping sickness records for the period 1905 to 1936 were extracted from original archival Medical and Sanitary Reports for the Ugandan Protectorate.These records were collected by the British colonial government of the time.The Principal Medical Officer (PMO) for the British Ugandan Protectorate presented summaries of returns of sleeping sickness cases; these summaries were regularly published in the Annual Medical and Sanitary Reports. Returns to the PMO were submitted by District Medical Offices, and included cases counts from hospitals, dispensaries, military reports, and sleeping sickness camps. Prior to this form of reporting, commenced around 1905, cases counts likely came from estimates provided by Ugandan chiefs: “In Busoga at that time… the chiefs were bidden to bring in to the District Commissioner a twig for the death of every one known to have succumbed to this disease in his district.” (25, p. 241) Records of sleeping sickness deaths in the Annual Medical and Sanitary Reports were available from the National Archives open shelf library for 1905-1936 by yearly totals. Counts of sleeping sickness deaths were further stratified by region (i.e. Kingdom). Spatial stratification was provided separately for 1905-1920 and 1932-1936, although nomenclature and regional designations differed significantly between the two summaries. These differences prevented accurate merging of data from the two time periods into a single 1905-1936 summary of sleeping sickness distribution by Kingdom. Data were also available by county in the district of Buganda, where the sleeping sickness outbreak was focused, for 1905-1908.The data were summarized and used to develop spatial maps of sleeping sickness distributions in Uganda. Comprehensive sleeping sickness records after 1936 were only available by national totals, although records prior to 1998 refer exclusively to disease in the south-east of Uganda. No evidence of official spatial stratification of data was found for sleeping sickness cases between 1936 and 1976; the latter date representing the proliferation of an extensive outbreak, which prompted active data collection. Case counts for the 1937-75 period were compiled from available literature resources: 1937-5826 , 1960-7114 , 1972-7527 , and 1976-200115 . Current distribution of sleeping sickness by district was acquired from the Ministry of Health, Kampala, Uganda. Total sleeping sickness deaths and cases for south-eastern Uganda were compiled and entered into Microsoft Excel.These were summarized in a time series for the period of 1905-2003. Hard copy maps of current sleeping sickness foci were reproduced by sub-county using the geographic information system, ArcMap 9 (ArcGIS 9, ESRI Systems, Redlands, CA, USA). Counts of sleeping sickness deaths by Kingdom for 1905-1920 were inputted into ArcMap with 1911 population census records for the same Kingdom areas. A map of sleeping sickness prevalence by kingdom for 1905-1920 (total deaths over period/ kingdom population) was produced. Historical distributions, based on the 19051920 Kingdom prevalence map, were compared to current disease foci to identify differences between the 1905 and 1976 outbreaks. Comparisons between historical distributions and current foci were noted and are discussed here, including a focus on the implications of these observation for the understanding of at-risk locations and risk factors for sleeping sickness in Uganda. Results Temporal trends: Figure 1 provides a temporal trend graph of sleeping sickness occurrence for south-eastern Uganda since 1905. While the outbreak at the beginning of the 20th century is likely to have started in the late 1890s and peaked in 19021 , cases were not officially recorded until 1905. It should also be noted that the graph shows deaths for the 1900-1920 outbreak, and cases for later disease occurrence. As can be inferred, the 1905 outbreak was significantly larger than the outbreak in 1976. Cases continued to occur in the south-east, with a second major sleeping sickness epidemic breaking out in 1976 (Figure 1).While the epidemic curve suggests a bi-modal epidemic, it is likely that this outbreak was a single epidemic, with reduced case detection and brief 1980 intervention measures explaining the low case rate in 1981-1985. Negligible prevalence of sporadic cases in the traditional fly belt during the years leading up to the 1976 outbreak is also likely attributable to reduced case detection resulting from poor surveillance measures in Uganda, which was subject to particularly unstable political conditions at the time22,27-29 . Tsetse distributions: Figure 2 provides a map of tsetse fly distributions in Uganda in 1969 24.The two major tsetse species acting as sleeping sickness vectors in Uganda are shown, including G. f.fuscipes and G. pallidipes. As can be seen in Figure 2, the range of the current vector, G. f. fuscipes, roughly spans a wide area surrounding Uganda’s river and lake shores. These distributions provide the most recent comprehensive information on the range of the sleeping sickness vector species at the national level in Uganda. National or regional mapping has not been carried out recently since the creation of the distributions shown in Figure 2. As such, little information is known about the spatial extent of tsetse presence or densities in districts in Uganda. Anecdotal reports suggest, however, that tsetse are likely to be present across much of Uganda. Knowledge of the traditional habitat preferences of tsetse species also provide information on potential tsetse distributions. G. f. fuscipes, the current vector of sleeping sickness, is associated with riverine areas 1; it is likely that much of Uganda’s riverine zones are infested with this vector.The potential distribution of G. pallidipes, which has been associated with the distribution of animal hosts 1, 12, is less clear.While not currently implicated in sleeping sickness transmission, G. pallidipes was reported to be the dominant vector during outbreaks in the 1930s and 1940s 28. Sleeping sickness distribution – present The current distribution of sleeping sickness can be seen in Figure 3. There are two key foci of the disease in Uganda, including a T. b. rhodesiense focus in the eastern districts, and a T. b. gambiense focus in the West Nile (north-west) region. Areas of recent disease spread are also shown, particularly spread into the district of Soroti from the southeast, where a demonstrable outbreak began in 1999. Sleeping sickness cases continue to rise in Soroti, with 129 cases recorded in 2003 15. Recent reports have identified outbreaks in Kumi, Kaberamaido and Lira in 2004-05 13, 15. Sleeping sickness distribution – past A spatial summary of sleeping sickness distribution in Uganda from 1905-1920 can be seen in Figure 4.While data are only available at the Kingdom level, the extent of the outbreak is observable. The majority of cases were recorded in the Kingdom of Buganda, where the outbreak was first observed. Prevalence can be found, however, throughout eight of the fourteen Kingdoms, including parts of south-west and central Uganda.This contrasts with current distributions, where the south-west and central districts have remained predominantly free of disease. In particular, the epidemic focus in Buganda differs significantly from the current spatial location of foci in the south-east and northwestern/ West Nile regions.The prevalence of cases in all districts bordering Buganda suggests that the distribution of cases in that district cannot be assumed to have occurred only in eastern or lake-side Buganda. Discussion The data are subject to collection and reporting bias. Colonial presence was disproportionately high in the southern population centres of Kampala and Entebbe. Reporting of sleeping sickness cases can, therefore, be expected to be higher in the south than in northern districts. In spite of this, there is no evidence to suggest that the disease was not focused along the shores of Lake Victoria, as was recorded. During the period of 1914-1918, European presence in Uganda decreased due to the military duty requirements of World War I 30. This decrease in British civil administration in Uganda may have contributed to reporting bias of sleeping sickness cases. Recorded cases of sleeping sickness may also exclude cases not reporting to a formal government facility. It is unclear whether the form of reporting by chiefs, described above, continued through to 1936; the level of non-reporter bias by Ugandans avoiding colonial authorities is unclear. Results of historical sleeping sickness distributions in Uganda for the 1900-1920 outbreak period provide a distinct contrast to current sleeping sickness foci. It is perhaps surprising that such a comparison has received negligible attention given its potential implications on current perspectives of at-risk sleeping sickness areas in the country. The map in Figure 4 suggests that sleeping sickness has occurred in regions well beyond the current north-western and south-eastern foci. In particular, disease is noted in the Kingdoms of Ankole and Toro (south-western Uganda), Lango (central Uganda), and western Buganda (south-central Uganda) during the 1900-1920 outbreak, where no disease is currently reported.These results can be interpreted to indicate that either, 1) there has been a change in the distribution of risk factors since the 1900-1920 outbreak that has created the new foci of sleeping sickness risk, or 2) much of Uganda can be considered at-risk of sleeping sickness, and given favourable transmission conditions, disease could spread into areas uninfected since the early to mid 1900s. The risk factors of sleeping sickness may have changed since the early 1900s, reducing risk in areas previously infected, and increasing risk in areas currently infected.This could be attributed to changes in land cover, cattle movements, population distributions and densities, and socio-economic conditions. Very little information and research has been conducted to assess such changes, and little evidence exists to suggest differential change that would make the south-east or north-west particularly vulnerable. In the case of the West Nile region and northwestern Ugandan districts, proliferation of sleeping sickness is attributed to refugee movements and interaction with infected regions of southern Sudan 14. Population movements, refugee camps, and unstable conditions, however, have also been present in south-western Uganda near the border with Rwanda, where significant numbers of refugees have crossed into Uganda. Until recently, no comprehensive and readily available information has been available on land use changes over time in Uganda. Land use time-series are currently being developed, however for both the south-east (Department of Population Medicine, University of Guelph, Canada) and the south-west (Centre for the Study of Institutions, Populations, and Environmental Change, Indiana University, USA), and should provide valuable insights into distribution of land cover and potential tsetse habitats in the south. Recent research has identified livestock movements as a potentially significant factor in the introduction of human-infectious trypanosomes into new regions of Uganda. Research by Fèvre et al. 3 indicates that the outbreak in Soroti District was likely triggered by re-stocking of cattle into Soroti from infected southeastern districts. Livestock re-stocking may also have played a role in triggering the widespread 1900-1920 epidemic 8. Given these results, evaluation of the potential links between livestock movements and the recent spread of sleeping sickness into Kumi, Kaberamaido and Lira Districts is a priority; such research may contribute to increasing support for control and prevention targeted at livestock reservoirs. Limited and out-dated information on distribution and density of tsetse flies in Uganda compounds challenges to prediction and management of sleeping sickness spread.The distributions of both the G. f. fuscipes and G. pallidipes vectors shown in Figure 2 are influenced by changes in land cover, development, and habitat control programs. Distribution maps from 1969 such as those shown in Figure 2 provide little guidance for public health prevention and control in the absence of up-to-date distributional information. In addition, national distribution maps do not capture the significance of local-level risk factors associated with tsetse fly presence; this is particularly important since sleeping sickness incidence is focal, predominantly occurring in localized outbreaks. Density of flies per unit area, ratio of flies to humans and livestock reservoirs, vector capacity of the tsetse, and proximity of habitat to settlement can also be significant factors driving sleeping sickness risk 17, 31, 32. FITCA, a project looking at Farming in Tsetse Controlled Areas, has collected data on localized tsetse densities, livestock densities, cattle trypanosomiasis prevalence, and sleeping sickness cases in a selection of study sites in south-eastern Uganda 33. Detailed and finished maps of these data have not yet been published, but should provide preliminary information on tsetse density and distribution of risk in the south-east.The implications of these data for areas outside current foci are limited by the absence of even crude tsetse data outside of the southeast. Results may, however, provide insights into trypanosomiasis transmission dynamics and vector ecology for G. f. fuscipes. Of particular concern is the immediate potential for spread of disease into Uganda’s north-central districts, such as has already occurred in Soroti. Research into historical drivers and triggers of the central and east African sleeping sickness outbreaks of the early 1900s have focused on civil disruption and livestock movements. Social and political instability has been associated with the 1900-1920 outbreaks in sub-Saharan Africa 8, 10, 34-36, as well as more recent disease reemergence in central Africa, including Sudan, the Democratic Republic of the Congo (DRC), and Angola 37-39. Sudan experienced rapid rises in sleeping sickness prevalence during an intensive civil war and collapse of public health infrastructure in the 1990s 38. In the DRC, suspension of the National Programme for the Fight Against Trypanosomiasis in 1993, in conjunction with prolonged civil conflict, have resulted in similarly dramatic rises in sleeping sickness incidence 37. Angola, which ended a 27-year civil war in 2002, continues to struggle with infrastructure and funds to combat the disease 39. In Uganda, the continuation of rebel activity in the north of the country has meant on-going destabilization, extensive internal displacement of Ugandans, and increased social instability. These factors, in conjunction with the likelihood of tsetse presence, historical evidence of infection, and patterns of sleeping sickness spread from both the north-western and south-eastern foci, are cause for considerable immediate concern. Sleeping sickness prevention and control in Uganda has also come under significant pressure due to lack of adequate funding at multiple levels of government, and on-going degradation of programme activities and supplies. There is significant potential for the two diseases, T. b. gambiense in the north-west and T. b. rhodesiense in the south-eastern foci, to merge in north-central Uganda, a region already burdened by political and social instability. Where such conditions of civil unrest, population displacement, and livestock movement favour introduction of the human-infectious trypanosome parasite, sleeping sickness proliferation may be considered a risk well beyond currently identified disease foci. Conclusion These observations indicate areas of Uganda previously infected with sleeping sickness that have remained without infection for several decades. In contrast, current infection is spreading into new areas with no previous evidence of infection. In some areas of east-central Uganda, current T. b. rhodesiense infection overlaps with historical T. b.gambiense infection from the 1950s. The causes of these observed processes remain unclear. Explanation and enhanced understanding of the drivers of historical sleeping sickness distributions in Uganda may have significant implications for prediction and management of current sleeping sickness spread. Given evidence of previous sleeping sickness presence in regions of Uganda not currently considered disease foci, consideration should be given to the increased potential for disease spread outside of the north-western and south-eastern regions. The causes for current absence of sleeping sickness in the historical foci of the Toro and Ankole Kingdoms and most of Buganda Kingdom need to be studied.These historical results are further compounded in their significance by increasing incidence and increasing spread of sleeping sickness in Uganda at this time. Particular concern should be placed on north-central Uganda, where disease occurred during the 1900-1920 outbreak, and where civil conflict and socio-political instability contribute to high population vulnerability. Acknowledgements This work was carried out with the aid of a grant from the International Development Research Centre (IDRC), Ottawa, Canada. Information on the Centre is available on the web at www.idrc.ca. Research was also supported by funding from the National Science and Engineering Research Council of Canada (NSERC), and the IDRC in Project 100106: ‘Links between sleeping sickness and natural resources endowments and use: what can communities do?’ Special thanks to Lubowa Abdelrahman, Makerere University, Kampala, Uganda; Dr. Mbulamberi, Ministry of Health, Uganda; Dr. Eric Fèvre, University of Edinburgh, UK; the late Dr.Thomas Gitau; and James Ford. References
Copyright © 2006 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs06049f2.jpg] [hs06049f1.jpg] [hs06049f3.jpg] [hs06049f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}