 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
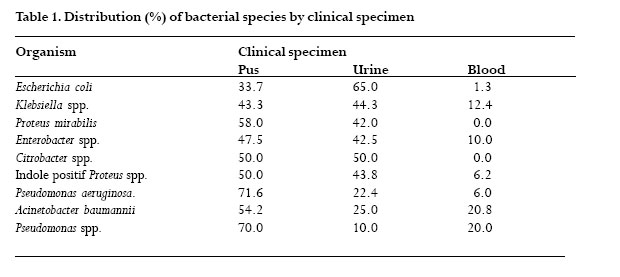
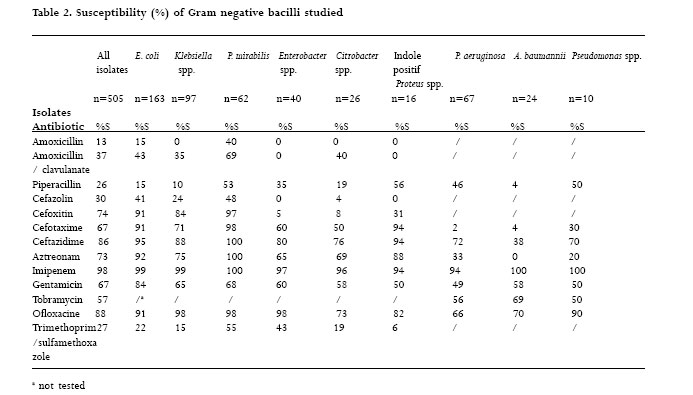
African Health Sciences, Vol. 6, No. 4, Dec, 2006, pp. 232-235 Antimicrobial activity against gram negative bacilli from Yaounde Central Hospital, Cameroon Joseph Gangoue-Pieboji1, 2*, Sinata Koulla-Shiro3, Pierre Ngassam 2, Dieudonne Adiogo3, Peter Ndumbe 3 1. - Institute of Medical Research and Medicinal Plants studies, P.O. Box 8404 Yaounde, Cameroon Corresponding author Institute of Medical Research and Medicinal plants Studies (IMPM) P. O. Box 8404 Yaounde, Cameroon Tel: 237 924 57 70 Fax: 237 222 62 62 E-mail: jgangoue@yahoo.fr Code Number: hs06050 Abstract Background:Antimicrobial resistance among bacteria pathogens is a world-wide issue.The antimicrobial susceptibility patterns of common pathogenic bacteria are essential to guide empirical and pathogen-specific therapy; unfortunately, these data are scarse in Cameroon. Key words: antimicrobial agents, resistance, Gram-negative bacilli, bacteria susceptibility testing, Cameroon. Introduction Gram-negative bacilli are the most important bacterial pathogen, and are generally resistant to antibiotics1, 2, 3 . Monitoring for antimicrobial resistance in this group is important because resistance has been reported to be associated with increased patient morbidity and mortality, and contributed to escalating healthcare cost4 . Antimicrobial resistance is increasing in many bacteria and is a worldwide problem5, 6. The antimicrobial susceptibility patterns of common pathogenic bacteria are essential to guide empirical and pathogen-specific therapy. This information is also important for rational policies against antimicrobial resistance. Unfortunately, in many developing countries, these data are scarce because of dwindling resources. In Cameroon, data on antimicrobial resistance among bacterial pathogens are sparse. In an effort to determine the extent of antimicrobial resistance amongst Gram-negative bacilli isolated in Yaounde Central Hospital Laboratory of Bacteriology, we conducted a survey of 505 Gram-negative bacilli and measured their in vitro susceptibility to antimicrobial agents. Materials and Methods Between April 1995 and March 1998, all the aerobic Gram-negative bacilli isolated in the laboratory of bacteriology of Yaounde Central Hospital were collected prospectively. The isolates studied were confined to unrelated first isolates from different patients, and did not include multiple isolates from the same patient. Isolates were recovered from urine, pus and blood cultures and identified by standard laboratory technique methods7 and confirmed by Api 20E (BioMerieux, France). The antimicrobial susceptibility test was determined by the Kirby-Bauer disk diffusion method following the National Committee of Clinical Laboratory Standards (NCCLS) for agar diffusion tests8 . The antibiotics tested were amoxicillin (30µg), amoxicillin/ clavulanate (20/10 µg), piperacillin (100 µg), imipenem (10 µg), cefazolin (30 µg), cefoxitin (30 µg), cefotaxime (30 µg), ceftazidime (30 µg), aztreonam (30 µg), gentamicin (10 µg), tobramycin (10 µg), ofloxacin (5 µg) and trimethoprim/sulfamethoxazole (1.25/23.75 µg). The following American Type Culture Collection (ATCC) microorganisms were tested each time susceptibility testing was performed: Escherichia coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853. Test results were only validated in the cases where inhibition zone diameters of the control strains were within performance ranges8 . Data were analyzed using Whonet 4 (World Health Organization, Geneva, Switzerland) and resistance included combined, intermediary and resistance results. Results A total of 505 aerobic isolates were collected, identified, and tested. Enterobacter iaceae (E. coli, Klebsiella spp., Proteus spp., Enterobacter spp., and Citrobacter spp.) represented 79.8% of the isolated strains. Non fermentative Gram negative bacilli (Pseudomonas spp. and Acinetobacter baumannii) represented 20.2%. The sources of the isolates are shown in table 1. Table 2 summarizes the results of susceptibility tests of Gram-negative bacilli studied against antimicrobial agents. Imipenem (98% susceptible (S)) was the most active agent against all pathogens tested followed by ofloxacine (88% S) and ceftazidime (86% S).Amoxicillin (13% S), piperacillin (26% S), trimethoprim/ sulfamethoxazole (27% S), cefazolin (30% S) and amoxicillin/clavulanate (37% S) were the least active agents. Against E. coli, susceptibility rates range from 15% (amoxicillin, piperacillin) to 99% (imipenem).The least active agents against Klebsiella spp. were amoxicillin (0% S) followed by piperacillin (10% S) and trimethoprim/sulfamethoxazole (15% S).The most active agents were imipenem (93% S) and ofloxacin (98% S). Proteus mirabilis was the most sensitive pathogen of all microorganisms.The susceptibility rate ranged from 40 % (amoxicillin) to 100% (imipenem, ceftazidime and aztreonam). Concerning Enterobacter spp., only two antimicrobial agents had activity rate >80% ((ofloxacin (98%) and imipenem (97%)). For Citrobacter spp. the most active agents were imipenem (96% S) followed by ceftazidime (76% S) and ofloxacin (73% S). Only 94% of P. aeruginosa isolates were susceptible to imipenem, as compared to 100% observed for A. baumannii. However, 72% of P. aeruginosa were susceptible to ceftazidime as compared to only 38 % of the A. baumannii. All the A. baumannii isolates tested were resistant to aztreonam. Discussion This study represents an extensive examination of the susceptibility patterns of Gram negative bacilli isolated in the laboratory of bacteriology of Yaounde Central Hospital. Our isolates represente both nosocomial and community acquired-pathogens, and were collected from April 1995 to March 1998.The results of this study show that in general, high rate of resistance occurs among Gram-negative bacilli to commonly used antibiotics (penicillins, first generation cephalosporin and trimethoprim/sulfamethoxazole). For E. coli and Klebsiella spp., the rate of resistance to third generation cephalosporins and other â-lactam antibiotics can be explained by the high production of penicillinase and the production of extended spectrum â-lactamase 3, 9. However, the rate of this resistance is high compared to those reported in developed countries 10, 11. Enterobacter spp. and Citrobacter spp. were highly resistant to ceftazidime, cefotaxime and aztreonam. Similar results were observed in Cairo (Egypt) by El Kholy et al., 2003 12 and in developed countries 10, 13. This resistance could be explained by the high production of cephalosporinase and the production of extended spectrum â-lactamase by these strains 3, 9. Our data showed that P. mirabilis is the most sensitive species. The susceptibility rates of this species to all antibiotics tested are compared to those observed in developed countries 10, 11. Non-â-lactam antibiotics resistance rates among the species of the Enterobacter iaceae family studied were comparable to the reported rates in other parts of developing countries 14, 15, but higher than those reported in developed countries 10, 13. The combination of trimethoprime/sulfamethoxazole is extensively used in Africa owing to its antimicrobial spectrum of activity, and its low cost 16. In addition, extended spectrum âlactamase production is usually associated with resistance to non-â-lactam antibiotics such as aminoglycosides, fluoroquinolones and trimethoprim/sulfamethoxazole17. The susceptibility rates of isolates of P. aeruginosa and A. baumannii in this study to all antibiotics tested except for imipenem, were low compared to those reported in developed countries 10, 18, 19 and similar to those observed in Egypt 12 and in West Africa 15. In conclusion, our study suggests the high rates of antimicrobial resistance among Gram-negative bacilli. The presence of E. coli and Klebsiella spp. isolates resistant to third generation cephalosporin suggests the importance of monitoring this phenotype.Particularly alarming is the appearance of low level imipenem resistance among different species of Gram negative bacilli studied. The results of this study indicate that more resources should be allocated to encourage good antibiotics utilization and practice. In addition, to provide information for choosing either empirical or direct therapy to physicians, surveillance to antimicrobial resistance is necessary. Acknowledgements We thank the Yaounde Central Hospital administration for accepting us to conduct this study in their hospital. We also thank the technicians of the Laboratory of Bacteriology of the Yaounde Central Hospital Mrs J. Mvondo, M. Tchonko, S. Ntoual, E. Dongmou, M. Wodo, M. Abiazen and M.C. Epape for their help during this work and Drs G. Kuepouo and A.Tchinda for reading the manuscript. References
Copyright © 2006 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs06050t2.jpg] [hs06050t1.jpg] |
| |||||||||

{kind=link}
{kind=link}