 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
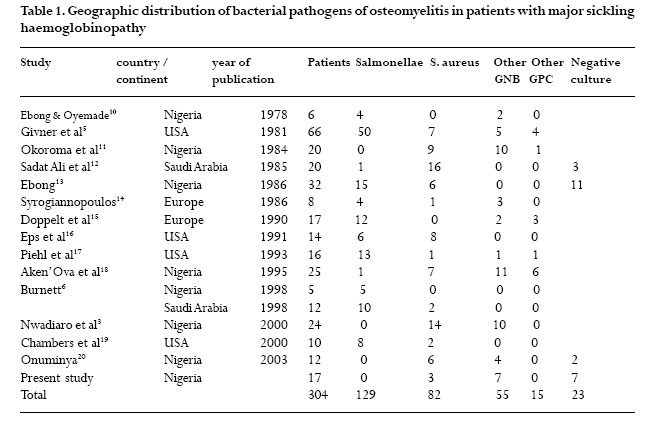
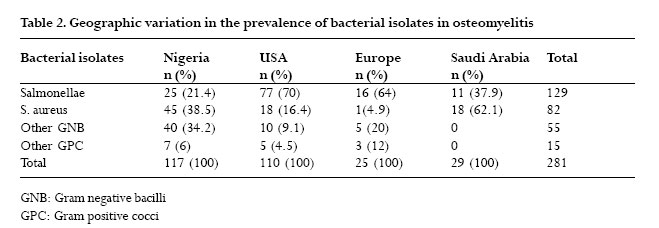
African Health Sciences, Vol. 6, No. 4, Dec, 2006, pp. 236-239 Bacterial osteomyelitis in major sickling haemoglobinopathies: geographic difference in pathogen prevalence L.O.A. Thanni Dept of Orthopaedics and Traumatology, College of Health Sciences, Olabisi Onabanjo University, Sagamu Ogun State, Nigeria Correspondence: L.O.A. Thanni. Dept of Orthopaedics and Traumatology College of Health Sciences Olabisi Onabanjo University, P.M.B. 2022 Sagamu Ogun State, NIGERIA E-mail: loathanni@yahoo.com Code Number: hs06051 Abstract Background: Controversy exists about the bacterial pathogen that is most often associated with osteomyelitis in major sickling haemoglobinopathies, that is, HbSS, HbSC, and HbSthalassemia. Key words: haemoglobinopathy, osteomyelitis, sickle cell disease, bacteria, salmonella, staphylococcus aureus. Introduction It is generally accepted that Staphylococcus aureus (S. aureus) is the most common organism associated with osteomyelitis1. However, controversy has existed for decades about the most prevalent bacterial pathogens associated with osteomyelitis in patients with major sickling haemoglobinopathies2,3,4. Givner et al5 attempted to resolve the controversy by studying a patient population derived from 8 published articles on the subject and concluded that salmonellae are the most common pathogens. All the patients in his series were from the USA. A similar review by Burnett et al6 showed that salmonella is the most common pathogen in patients with sickle cell disease (SCD) in both developing and in developed countries. Recent series found S. aureus to be the most common pathogen in osteomyelitis in SCD. Apparently, the controversy persists. This study is aimed at identifying regional or continental variations, if any, in the prevalence of bacterial pathogens in osteomyelitis in patients with major sickling haemoglobinopathies and also to identify any change in the worldwide prevalence. Methods The data on all patients with osteomyelitis in our hospital between January 1994 and December 2004 were reviewed and information information extracted from their case records. These informations include haemoglobin genotype, isolated bacterial pathogen, and source of specimen for microbiologic studies. This database was then searched for those with major sickling haemoglobinopathies that is, HbSthalassemia, HbSS, HbSC, and confirmed with electrophoresis. Published articles on the subject were also identified and reviewed using Pubmed (online version of Medline) and Ajol (African Journals Online) as well as local library collection of journals. Pubmed and Ajol were searched in February 2005 using the key words haemoglobinopathy and osteomyelitis, sickle cell disease and osteomyelitis, haemoglobin genotype and osteomyelitis. Abstracted data include the study population size, age range, hemoglobin genotypes, isolated bacterial pathogen and the source of specimen for bacteriology. All included published articles were on osteomyelitis and included data on the bacteriology of the disease in major sickling haemoglobinopathies. Inclusion criteria All published articles on the subject were eligible for inclusion. However, articles with patient selection bias, for example, reports of Salmonella osteomyelitis without including the incidence of other organisms as well as isolated single case reports were excluded. Results Our hospital data revealed 17 patients with major sickling haemoglobinopathies over an 11 year period.All of them had HbSS. Out of ten positive cultures, S. aureus was isolated from three of them and Gram negative bacilli from seven others. The latter include three klebsiella species, two proteus and pseudomonas species each. Fourteen other studies were eligible for study and were included in the analysis. They were all retrospective studies. As indicated in table 1, there are reports from Nigeria, USA, Europe and Saudi Arabia, involving a total of 304 patients and two hundred and eighty one isolates.There were 129 (45.9%) salmonellae and 82 (29.2%) S. aureus while other Gram negative bacilli (GNB) and other Gram positive cocci (GPC) accounted for 55 (19.6%) and 15 (5.3%) of the isolates respectively. Out of 117 isolates in the studies from Nigeria, salmonellae accounted for 25 (21.4%), S. aureus 45 (38.5%), other GNB and GPC were 40 (34.2%) and 7 (6%) respectively. In contrast, out of 110 isolates in the studies from the USA, there were 77 salmonellae (70%), 18 S. aureus (16.4%), 10 other GNB (9.1%) and 5 other GPC (4.5%). Reports from Saudi Arabia include11 (37.9%) salmonellae and 18 (62.1%) S. aureus isolates while those from Europe include 16 (64%) salmonellae and 1 (4.9%) S. aureus, table 2.The ratio of salmonellae to S. aureus is 1:1.8 in the Nigerian reports, 4.3:1 in the US reports, 1:1.6 in the Saudi and 16:1 in the European series. Discussion The results indicate that in Nigeria, S. aureus is the most common pathogen in osteomyelitis in patients with major sickling haemoglobinopathy. The prevalence of S. aureus in this country, 38.5%, is more than two times that in the reports from the USA (16.4%). However, the prevalence of salmonella in the USA reports, 70%, contrasts sharply (more than three times) with 21.4% in the Nigerian studies. Also, the prevalence of GNB is greater in the reports from USA than those from Nigeria and the other study regions. The prevalence pattern of salmonella and S. aureus is similar in Nigeria and Saudi Arabia, while the pattern in Europe is similar to that in USA but different from the other regions. The reasons for susceptibility to staphylococcal bone infection in general1 and salmonella infection in haemoglobinopathy7 have been previously discussed. The overall ratio of salmonella to S. aureus osteomyelitis in SCD in this report is 1.6:1. Compared with a ratio of 2.2:1 in the review of Burnett6 in 1998, there is a reduction in the relative prevalence of salmonella which was rather high in the 1981 review of Givner5 of 7.1:1. The overall worldwide trend may be that of a declining relative prevalence of salmonella while that of S. aureus may be increasing in osteomyelitis in patients with SCD. This however requires confirmation with carefully designed studies. It can be concluded that there are geographical differences in the prevalence of bacterial pathogens associated with osteomyelitis in patients with major sickling haemoglobinopathies. Salmonellae are the most common pathogens of osteomyelitis in major sickling haemoglobinopathies in the USA whereas S. aureus is the most common pathogen in Nigeria and the Middle East. These differences cannot be readily explained. However, salmonella infections in general are not uncommon in the USA and Europe, arising from consumption of raw food and use of animal waste in food production8,9. In Nigeria, boiling of food before eating is a common practice that may control the transmission of salmonella which may contaminate food. In addition, availability of antibiotics as over the counter drugs in many Nigerian cities may have resulted in abuse that could have controlled endemicity of salmonella infections thereby reducing its association with osteomyelitis in this region. Acknowledgement The contribution of Dr C.O. Alebiosu with data search and filtering, Resident doctors and Interns with case file extraction is gratefully acknowledged. References
Copyright © 2006 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs06051t1.jpg] [hs06051t2.jpg] |
| |||||||||

{kind=link}
{kind=link}