 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
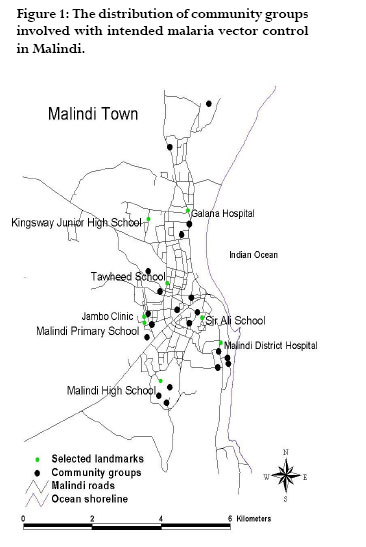
African Health Sciences, Vol. 6, No. 4, Dec, 2006, pp. 240-247 Community based vector control in Malindi, Kenya Lydiah W. Kibe1, Charles M. Mbogo1†, Joseph Keating2, Sassy Molyneux1,3, John I. Githure4 & John C. Beier 2 1Centre for Geographic Medicine Research-Coast, Kenya Medical Research Institute (KEMRI) P.O. Box 428, Kilifi, Kenya †Correspondence: Charles Mbogo, Senior Scientist, Centre for Geographic Medicine Research-Coast, Kenya Medical Research Institute (KEMRI), P.O. Box 428, Kilifi, Kenya: Tel. 254 41 22063, Fax 254 41 22390; Email: cmbogo@kilifi.mimcom.net Code Number: hs06052 Abstract Background: Community involvement has become an important component of the National Malaria Control Strategy in Kenya, resulting in the organization of groups charged with addressing mosquito and malaria-related concerns within the community. Keywords: vector control, malaria, community groups, urban, Kenya Introduction Mosquito vectors pose significant public health problems. In addition to their role in the transmission of malaria parasites, filarial worms, and arboviruses, biting mosquitoes are a nuisance and can disrupt both sleep and work. Although the vast majority of mosquitoes in urban Africa are Culex, there is substantial entomological and epidemiological evidence of malaria transmission in cities1, 2 , suggesting that Anopheles mosquitoes are ubiquitous in most African cities and thus pose a significant public health problem to populations generally lacking in natural immunity. There is a clear need to develop long-term, sustainable malaria vector management programs in urban sub-Saharan Africa (SSA)1,2. Governments and communities can play a role in the development and implementation of vector management systems. Identifying what government and communities are currently doing to protect individuals from biting mosquitoes, and what they are doing to deliver malaria control interventions, is key to the development of comprehensive, community-wide malaria control programs. In SSA, indoor spaying of insecticides, the use of insecticide-treated bed nets (ITN), and mosquito avoidance practices are widely promoted as effective ways of reducing human-mosquito contact3 . Although larval source reduction has been successful in Italy, Israel, United States, and parts of Brazil, as a tool for eliminating malaria vectors over large areas4-7 , little attention has been given to larval control and environmental management as a means of reducing mosquito vector populations, and subsequent mosquito-borne disease, in urban SSA. Funding, participation, and community perception have all been shown to affect vector control programs7 . It is widely conceived that community involvement is key to vector control, and can achieve sustainable results in a shorter time by mobilizing all segments of society to focus on awareness and the determinants of the problem.8-17 Mouchet (1982) wrote that ‘the community can no longer remain a spectator, but must either be actively involved with vector control or make a financial contribution to control’17. Agyepong (1992) also argued that the use of local community potential was paramount to sustainable vector control, and that effective control is dependent upon local governments, health institutions, and the community’s understanding of the need and rationale for vector control18. The purpose of this paper is to report on the status of community groups reportedly involved in malaria vector control in Malindi and identify major obstacles to vector control. This study was conducted to collect baseline information for an upcoming community-based vector management intervention, and to assess the potential contribution of these groups to the development of a long-term integrated vector management program in Malindi. Information about attitudes, knowledge, and practices related to mosquito vector and malaria control was collected from key informants at the Ministry of Health (MOH), community meetings, and focus group discussions during February and March of 2002. Methods Study area Keating et al. (2003) and Macintyre et al. (2002) describe the coastal urban study area19-20 . Briefly, Malindi is the tenth largest city in Kenya, with approximately 80,000 inhabitants. It is located about 120 km north of Mombasa. April to June and October to November are considered the wet seasons. The climate is considered tropical. Malindi is comprised of commercial and residential areas, agricultural and undeveloped areas, and hotels and stores along the coastal strip.Tourism, retail, fishing, and trading are the major economic activities. Anopheles gambiae s.s, An. funestus, An. merus, and An. arabiensis have been identified as important malaria vectors on the coast of Kenya 21-23. No malaria prevalence studies have been conducted in Malindi. In 2002, Malindi town was voted the cleanest Municipality in Kenya.The Municipal Council of Malindi (MCM) has created an environmental and mosquito control activity mandate under the national Primary Health Care (PHC) program. This resulted in the independent formation of community-based groups throughout the town, charged with environmental management tasks and supported in part by government funds.These groups were reported to have been key in keeping the city clean and in the implementation of many mosquito control activities. In an effort to create awareness about mosquitoes and the environment for example, an annual event known as “Mosquito Day” is observed. This event involves the clean up of trash piles, the removal of standing water, and the dissemination of media slogans such as “malaria mosquito free” and “Keep Malindi clean”. It should also be noted that although these activities were intended to reduce malaria vector habitats, it is not clear to what extent these activities targeted all mosquito species, or were effective over time. Key informant interviews Key informants were identified from within the MOH, MCM, and the Ministry of Culture and Social Service, Gender and Sports. They were asked to comment on the perceived role of community groups in malaria vector control, opportunities for furthering the control effort, and hindrances to sustainable implementation of vector control within the respective communities, from their perspective. Facilitators trained in participatory techniques conducted all interviews. Because many community groups are registered with municipal offices, key informants also assisted with community group identification, locations, and contact information. Stakeholder meeting A meeting was held with representatives of community groups, non-governmental organizations, businesses, and public offices charged with organizing vector control within Malindi. The meeting had two primary objectives. The first objective was to determine what stakeholders perceived as the priorities in vector control, and who is responsible for such control activities. This was done via a discussion of priorities and options for malaria control in general. The second objective was to identify individuals who could assist with vector control training within the community, and with the monitoring and evaluation of such control activities. Focus groups Focus group discussions were held with 8 community groups, randomly selected from a total of 19 groups identified as having a reported role in mosquito control. Simple random sampling was used to minimize the bias associated with selecting only the most organized, active, or highly funded community groups. Although in-depth focus group discussions with all community groups would have yielded more generalizable information, the community group’s time, and the funding allocated for this portion of the project were operating constraints. Questions posed as part of the discussion included: What are the roles of community groups in vector control? What are the responsibilities associated with such control activity? What are the biggest operational constraints to effective control? What are the major challenges faced when implementing, or attempting to implement a program or control strategy? What is your perception of the level of malaria transmission or mosquito life cycle knowledge within the community? Do you know where mosquito larval sites typically exist within the community and how to distinguish between mosquito larvae and larvae from other organisms? Each discussion was followed by a feedback session where the group participants, the interviewer, and the note-taker exchanged comments and questions. The issues raised from the feedback session were put into consideration in the successive interviews. Discussions were held until a point of redundancy. Data Processing and Analysis All discussions were taped using a dictaphone and handwritten notes taken during each discussion. Later information was transcribed and written down word by word each day.Textual data was explored to generate categories and explanations by use of a thematic framework [24]. Using themes and objectives as reference points, each response was grouped in accordance with these themes and all other emerging issues were handled separately. In some cases ranking was done based on the most frequent response in order to estimate the reasons for certain actions.All issues were written down in summary sheets according to the objectives and focus of the study. Consistency and validity of the data was checked through triangulation of data from different methods used in the study. Results Nineteen (55.9%) of the 34 identified groups reported some form of mosquito control with the intention of reducing malaria vector populations. Most community groups (16) reported environmental management activities such as clearing of drains and ditches, and the removal of standing water and debris. These activities were intended to eliminate aquatic breeding habitats and resting places for malaria mosquitoes. Although the frequency of the activities described above is unknown, groups reported that the regularity to which these activities are carried out had declined since 1999, following the withdrawal of municipal council’s support. The distribution of community-based groups involved with environmental management and intended vector control was such that most communities within administrative sub-locations of the town were represented by at least 1 group, although the level and extent of the catchment area overlap is unclear (Fig. 1). Community groups were primarily comprised of residents from the general geographic area and were limited to youth, women, or a combination of youth and women, depending on the nature and overall purpose of the group. It was further reported that individuals from the community provided overall leadership of the respective groups. At the community stakeholder meeting, it was determined that the MOH, MCM, and community groups have been the main organizers of intended malaria vector control activities.The MOH is responsible for malaria case management within the Municipality while vector control is mandated to the MCM. In the past, the MCM was responsible for eliminating or treating mosquito aquatic habitats. Environmental management activities such as draining or filling areas of standing water and garbage collection, as well as educating the household owners on how to keep their homestead free from mosquitoes, was also part of the overall MCM malaria control strategy. However, due to lack of funds and resources, the MCM, stopped virtually all vector control field activities. The only environmental management activity the MCM is currently responsible for is garbage collection, which is contracted to private companies and is not considered Anopheles mosquito habitat in most cases. Role of community groups in vector control activities The results from the focus group meetings indicate that the intended malaria vector control activities carried out by community groups included the treating of water bodies with used engine oil, the spraying of houses with permethrin obtained from the MCM, the sewing, dipping, and selling of insecticide treated bed nets (ITN), the removal of standing water, the organization of community clean-up days, and the development and sale of products such as neem soap, which is thought to repel mosquitoes. Intended health education activities included home visits to assist with mosquito surveillance and disseminate information about malaria treatment and prevention, and advising residents on how to reduce mosquito-human contact. Most groups reported involvement in more than one activity, and one - The Shella Women Group reported making and selling ITNs. Included among our groups was ‘The Green Town Movement’, which in addition to garbage collection, reports serving as an umbrella group for many other community groups. Group members explained that many groups, and their activities, were initiated by the Public Health Department of the MCM in response to increasing malaria and diarrhea prevalence, and decreasing water and sanitation safety. It was reported that in addition to forming many of the community groups, the MCM also provided training and information, and disseminated materials and equipment to assist with project start-up. The Shella Women’s Group for example, reported receiving netting material, sewing machines, and thread to initiate ITN development, whereby the money made from the sales would become a revolving fund for future projects and activities. The Maweni Primary Health Care Group reported that they received training, equipment, and chemicals for larviciding activity. The equipment included spray pumps, wheelbarrows, and rakes. The MCM provided monitoring, supervision, and guidance to these groups, and held monthly forums with all community groups to share and report ongoing and proposed activities. All respondents reported that the MCM and the MOH discontinued fund and equipment allocation in 1999, citing lack of funds and interest in specific communities as the primary reason. It was also reported that supervision of existing projects declined soon after. When asked what factors motivated or de-motivated groups and their members, respondents repeatedly raised continuous support and direct supervision as motivating factors. Initially, community groups’ activities were monitored by the MCM Department of Public Health. Respondents reported that this led to the recognition and appreciation of the groups’ activities by the community and their leaders. It was also noted that when community leaders, chiefs, and elders actively participated and encouraged specific events, community mobilization and active interest was much greater than events proposed and carried out under the auspices of government intervention. This was especially true of “community clean-up days” and “malaria mosquito days”. Respondents also reported that the training of group members, and the donation of tools and equipment were motivating factors, and greatly enhanced the groups desire to conduct activities. When asked about limitations on group motivation, several important and inter-related points were raised. One was the lack of sustainable income generation projects being incorporated into the groups’ activities. Members of the Shella Youth Group, for example, explained that their efforts to produce and sell ITNs were hindered by cheaper ITNs already in the market. A member explained that “a single roll of netting costs Kenya Shilling (Ksh) 9000 (USD 117.65), binding material costs Ksh 3000 (USD 39.22), and thread, needles, and insecticides cost Ksh 1000 (USD 13.07). This makes about 9 nets. We sell one net at Ksh 1500 (USD 19.61) which is considerably high compared to the Ksh 350 (USD 4.57) cost of other nets in the market.” Although many of the groups reported receiving token amounts from households for doing control activities, the amount was generally not enough to sustain the group’s activities. Reasons given for income generation activities being unsuccessful included some communities within Malindi being accustomed to receiving free or heavily subsidized products, or being unwilling to pay for activities seen as an MCM responsibility. As one group member reported:‘we lack full community support because we are seen as being employed by the municipal council.This is a drawback to our activities”. A second limiting factor commonly cited was group members’ personal financial situations. It was reported that in the absence of a sustainable income-generating project, control activity was not possible without municipal or government sponsorship because the need to cope with their own household economic situation precludes voluntary involvement, however keen they are to assist. Lack of funding, was considered an important contribution to the recent reductions in the number of active group members and the discontinuation of many mosquito control activities. A member of Shella Youth Group explained the situation in his group: “When you spend your time you expect to get something in return. Going around every house [to cut grass, drain stagnant water and put oil in pit latrines] some people used to refuse to pay Ksh 10 (USD 0.13).We got discouraged because when the evening came we wanted something to eat but there was nothing.We felt misused volunteering but we are also poor and are looking for bread.” This affected the group’s productivity potential, as almost half of the members who were initially trained on various methods of mosquito control eventually discontinued their participation. It was therefore clear that voluntarism, in the absence of direct gain and when combined with lack of community support, could not be expected from members with low household incomes. A third limitation reported was inadequate municipal support in the form of continued/effective training, equipment, supplies and visible endorsement of their role. Common comments included: “we need tools for clearing the area we live in.”“We need chemicals and ropes to clean the wells.” “We need [more] training because some of us do not know what to do or how to do it.” One group member explained, “We started with as many as 40 members but some people have left.The few of us who are left still do whatever we can [but basically our] activities were discontinued 3 years ago when we stopped receiving chemicals and equipment from the Municipal Council.” Others emphasized the lack of supervisory support on the part of the MCM: “We are not called for monthly meetings and when we invite them [pu-blic health officers] to our meeting they do not attend.” The Green Town Movement, created by the MCM and charged with coordinating all community group activities, was discussed with some suspicion and dissolution. The Green Town Movement was reported to receive substantial funds, but to use the money to clear garbage only. Participants from all groups reported that they did not really know how the money was spent or how it related to mosquito control in general, but that they were simply called on periodically by the movement for “clean-up” projects at various locations within the city. Critically, it was clear that group members themselves felt that the MCM should be responsible for vector control activities - ‘…because the MCM collects taxes and levies, they are mandated to conduct mosquito control activities” – and that this role was not being fulfilled. Knowledge and awareness of malaria and malaria vectors The term “homa” was generally used within the discussions to refer to malaria or malaria-related topics. Homa literally means hotness of the body or fever. The groups reported unanimously that homa was a big problem in the community. One focus group member was quoted as saying “ Homa is more of an enemy than the snake”. It was further reported that the symptoms of homa were easily recognized in the community, and that pregnant women and children were at a greater risk than the typical adult. Malaria treatment was often reported to be a combination of both modern and traditional methods. Depending on the stage of the illnesses and its severity, people usually started with some traditional therapy at home, followed by modern treatment in case of failure. If neither attempt succeeded, treatment was generally sought at the nearest health clinic. It is widely believed that malaria is cured with antipyretics such as paracetamol, tumbocid (anti-acid), and aspirin, which are usually bought from local shops or a chemist. Most respondents reported the regular use of traditional treatments such as the leaves and roots of the neem tree. The neem leaves or roots are reportedly boiled, and the resultant liquid drunk, bathed in, or steamed, depending on the perceived severity of the illness. Mbathe, Subili, mchuma, Zatari, Shumani, Mutsunga and Mzungi were other terms reported to describe traditional herbs used for treating homa. However, unlike biomedical drugs, the effectiveness of the herbal treatments was considered uncertain, as expressed by some of the respondents within the community groups. Most focus group participants stated that mosquitoes can cause homa. It was further stated that mosquitoes transmit the disease from a sick person to a healthy one, and also through dirty water deposits. “There are also a lot of mosquitoes here, if they bite you after biting a sick person you become sick. It is the mosquito which brings homa.” Participants also reported that the inability to afford preventive measures such as ITNs, and poor personal and environmental hygiene, as causes of malaria infection. Although most people acknowledged that mosquitoes transmit homa, there were other factors such as humidity, exposure to rain and cold, and bad wind locally known as “bad omen”, which, were cited as causative factors of homa. Although most of the respondents reported that they see organisms in the water, it was unclear if the respondents were familiar with mosquito larvae. One respondent stated: “…it is difficult to distinguish larvae from other things like eggs of frogs and other worms”. Several respondents reported seeing worms coiled like the letter ‘e’ but did not know if what they saw was related to mosquitoes. Most participants reported knowing what a typical adult mosquito looks like, although the terms used seemed to indicate an area of ambiguity (i.e. ikunua, and usugu both apparently refer to biting midges). Most groups reported that bush clearing and garbage removal were good ways to reduce mosquito populations. However, it was clear that no distinction is made between Anopheles mosquitoes and Culex mosquitoes in terms of control, as all mosquitoes are perceived as a public health problem. Discussion The results of this study indicate that the MOH, MCM and community groups previously carried out mosquito control activities aimed at reducing malaria, but currently control activities are largely limited to community-organized groups and individuals, and are extremely limited.The large proportion (56%) of community groups involved in some form of intended vector control activity suggests that these groups are interested in addressing the problem of malaria and are willing to participate. The future of these groups in relation to vector control activity is uncertain however because the MCM is no longer supervising projects, providing technical support or guidance, or funding many of the community groups. Additionally, these groups are unable to operate effectively because of limited resources and community support due to the perception that the government is responsible for malaria and mosquito control. The results of this study suggest that community groups have a strong interest in vector control activities in Malindi, but are constraints with resources such as tools, relevant knowledge, technical assistance and supervision. Furthermore, activities for reducing adult populations such as the clearing of vegetation and garbage collection, which many groups reported carrying out, have not been shown to reduce malaria vector populations in scientific studies. Similarly, the use of used engine oil by community groups as a larvicide for example, is not an environmentally sound method of controlling emerging mosquitoes. Active involvement of the community will require use of relevant information, knowledge and skills on mosquito control. In the absence of communication between all parties and appropriate levels of funding, this information will not reach community groups interested in doing vector control. Additionally, limited knowledge of mosquito life cycles indicates the need for educational programs aimed at strengthening community awareness about malaria mosquitoes specifically. These programs should be directed at increasing the awareness of the community about the role of mosquitoes in malaria transmission, and the different strategies devised to reduce mosquito abundance and human-mosquito contact. Groups are also facing difficulties in maintaining and targeting their activities because sustainable vector control activities require collaboration, partnership and communication between the scientific community, government officials, and community members. It is for this reason that developing a partnership in vector control, and identifying the roles and responsibilities of the different partners in order to maximize resources, is critical. At the community level, communities may be involved in the planning and implementation of activities, while the MMC and MOH mobilize resources and provide technical support and supervision, and the monitoring in order sustain the mosquito control operations support. As a consequence of poor management and financing, the supervisory role of vector control activities has been neglected, which has led to a decline in the number and quality of vector control activities, and a decline in community group membership. Further, community groups are becoming aware of their rights and obligations, following the change of government, and have started demanding to know the budget allocation for activities such as mosquito control. The community groups have formed an umbrella body comprising of representatives from all community groups that are involved in mosquito control activities.The group aims at overseeing and coordinating the activities of the groups, to act as a bridge between the community groups and the MMC and the MOH and to solicit for funds on behalf of the groups. Effective collaboration and communication are essential components of any serious vector or malaria control program. Additionally, the effectiveness of any vector control strategy is increased with the active and informed participation of the intended beneficiaries, and this can be enhanced if the communities have the necessary information, education and communications on a particular method12,25-27. As a follow-up to this study, we organized a ‘training of trainers’ workshop which was aimed at equipping the community groups with proper knowledge about mosquito and mosquito larvae recognition, appropriate methods of mosquito control, appropriate treatment of fever at home, and effective written communication skills for collaborating with ministry or official personnel.This ongoing activity is increasing mosquito and malaria awareness within communities, but will be meaningless in the absence of MOH, MCM and other stakeholder support.As recommended in urban malaria workshop in Pretoria, urban malaria is uniquely amenable to prevention and control if the existing health, planning, agricultural and governance structures collaborate with community 2. In conclusion, a collaborative relationship between the MOH, MCM, researchers, and community groups could lead to improved control activities in Malindi. Community groups are willing to contribute to vector control activities but are limited in terms of access to resources, scientific direction and supervision. Clear government policies, outlining the role of the government versus community members in terms of malaria control, as well as a supportive policy on incentives for participating community members and scientists, should be developed as a next step for coordinating future integrated vector management programs in Malindi. Acknowledgements We are grateful for the assistance of Dr Anisa Omar and his team at the District Ministry of Health,The Mayor of Malindi and his team, the District Officer of Malindi, and members of community organized groups who participated in this study. We would also like to thank Nellie Njoki, Samuel Kahindi, Salim Omar, and Boniface Nyaga at the Center for Geographic Medicine Research-Coast, Kilifi, Kenya for their data collection efforts.We are also grateful for the assistance of Dr Regina M Karega of Kenyatta University in editing the manuscript. NSF Grant DEB-0083602, and NIH Grants U19 AI45511 NIH, D43 TW01142, and FO6 TW05588 supported this research. This paper is published with the permission of the Director of the Kenya Medical Research Institute. References
Copyright © 2006 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs06052f1.jpg] |
| |||||||||

{kind=link}