 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
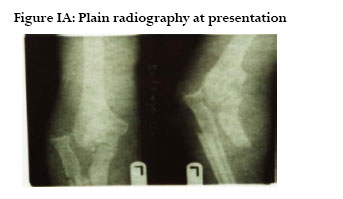
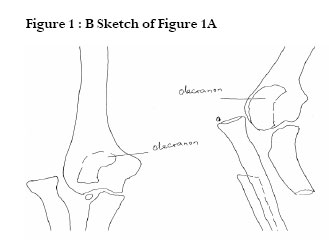
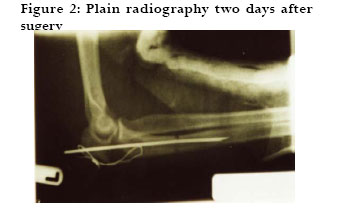
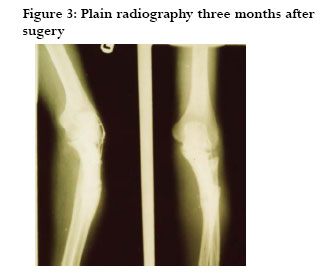
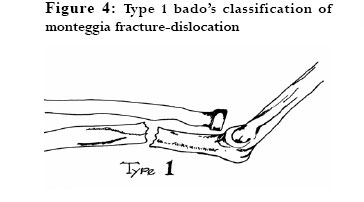
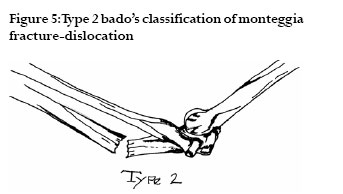
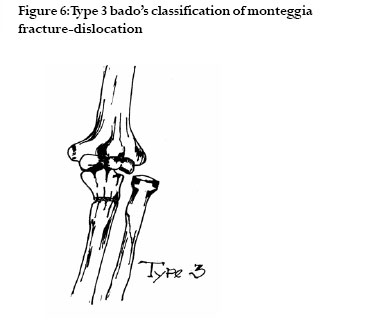
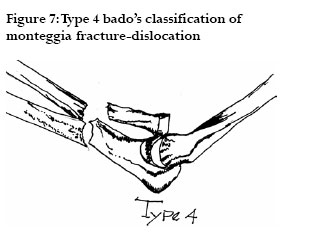
African Health Sciences, Vol. 6, No. 4, Dec, 2006, pp. 252-254 CASE REPORT Monteggia fracture-dislocation: a case report, its’ initial management and review of bado’s classification Abdullahi Agaba-Idu Musa Department of Surgery, Usmanu Danfodiyo University,Teaching, Hospital, Pmb 2370, SokotoNigeria, E-mail agabamusa@yahoo.com Code Number: hs06054 Abstract Fracture of proximal ulna and dislocation of the proximal radio-ulna joint in the same arm is called Monteggia fracture- dislocation. Four clinical variants of this fracture- dislocation have been described in literature.This is a report and description of initial management of a fracture- dislocation, which was consequent to a sideswipe injury and consisted of a combination of the following injuries; lateral dislocation of the radial head, fractures of the olecranon and proximal ulna in the left forearm.The radial head dislocation and fracture of the olecranon were open.The head of the radius was exposed through the same wound.This fracture-dislocation resembled type 3 Bado’s classification of Monteggia fracture-dislocation because of fracture of the olecranon close to the coronoid process and lateral dislocation of the head of radius. Key words: Monteggia fracture- dislocation; initial management; Bado’s classification. Introduction Sideswipe injuries (SI)1 are consequent to objects striking an elbow on the window ledge of a moving vehicle. The striking force can be another moving vehicle or objects protruding from it. A sideswipe injury usually consists of multiple. and a combination of fractures1,2 . They are often open fractures with wounds distal to the olecranon. Fracture of proximal ulna and dislocation of the proximal radio-ulna joint in the same arm is called Monteggia fracture- dislocation and can be caused by a sideswipe. This is a report and description of the initial management of a case of this type of fracture-dislocation, which consisted of a combination of the following injuries; open fractures of the olecranon, open lateral dislocation of the radial head, and fracture of the proximal one third of the left ulna. Case report MY, 35-year old, male, Nigerian, professional driver presented at the Accident and emergency Department of Usmanu Danfodiyo University Teaching Hospital Sokoto, Nigeria six hours after a road traffic accident, in which his left elbow was struck by a log of wood which projected from a vehicle that was coming from the opposite direction. On examination he was not pale but in distress due to pain. The left upper limb was flexed at the elbow and immobilized in a sling. Removal of the blood stained bandage around the elbow exposed the olecranon, head of the radius and the trochlea. Plain radiography of the left elbow revealed the radial head dislocation, fracture of the olecranon and proximal left ulna1,2 (figures1A and 1B).Wound swab was taken for microscopy, culture and sensitivity. Packed cell volume was 38%. Random blood sugar level was 6mmol/L. Initial management of the injury He had surgery the same day. Access to the fractures during surgery was gained through the existent wound. The radial head dislocation was reduced by traction. There was lost of bone from the olecranon. Intramedullary nailing aligned all the fragments of the ulna. Stainless steel wire was used to maintain the reduction of the olecranon. The wire fixation and initial intramedullary nailing were not rigid enough. For this reason the whole arm was immobilized in a plaster-of-Paris cast (figure 2). Result After two days, the wound culture revealed staphylococcus. The ciprofloxacin was prescribed for him on the basis of the sensitivity pattern3.The same day check plain radiography was done and it showed alignment of the fragments. At this time also a window was opened at the elbow for wound dressing, on alternate days with hydrogen peroxide and pure, natural, bee honey4 and the intramedullary nail was removed under anaesthesia. Six weeks after surgery the wound had contracted significantly and another check plain radiography revealed callus formation at the fracture sites.After three months the wound and fracture had healed completely (figure3).The cast and wire were removed. There was 1700 and 800 of active extension and flexion respectively5.The patient was planned for repeat surgery but he declined and said he was satisfied with the outcome of the initial management. He could drive and was discharged. Discussion In the literature reviewed in the internet and through colleagues, fracture-dislocation of such type was not mentioned. Management of the fractures was difficult because of the wound1.There was the risk of infection. Extensive dissection for internal fixation would have denuded the bones, caused necrosis and spread infections. Repeat surgery after the healing of the wound may have improved movement at the elbow but the patient was not interested. Bee honey4 dressing promoted wound healing. Conclusion Bado6 classified Monteggia fracture- dislocation into four types (figures 4, 5, 6 and 7):Type 1 consisted of fracture any where in the proximal two third of the ulna, anterior dislocation of the radial head and apex anterior angulation of the ulna.Type 2 consisted of fracture any where in the proximal two third of the ulna with the apex usually angulated posteriorly, posterior dislocation and often with fracture of the radial head.Type 3 consisted of ulna fracture, just distal to coronoid process and lateral dislocation of the radial head.Type 4 consisted of fracture any where in the proximal two third of the ulna, anterior dislocation of the radial head and fracture of the proximal one third of the radial below the bicipital tuberosity. This fracture-dislocation due to a sideswipe injury is rare and resembled type 3 Bado’s classification of Monteggia fracture-dislocation because of fracture of the olecranon close to the coronoid process and lateral dislocation of the head of radius. References
Copyright © 2006 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs06054f1b.jpg] [hs06054f6.jpg] [hs06054f1.jpg] [hs06054f5.jpg] [hs06054f3.jpg] [hs06054f2.jpg] [hs06054f7.jpg] [hs06054f1a.jpg] [hs06054f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}