 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
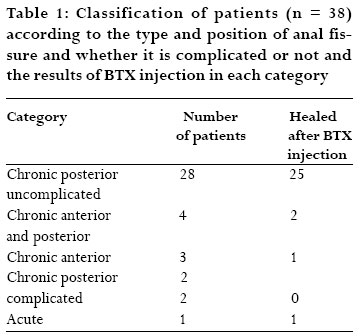
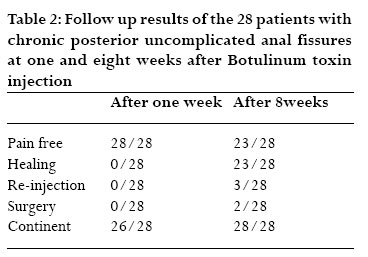
African Health Sciences, Vol. 7, No. 1, March, 2007, pp. 14-17 Botulinum toxin treatment for anal fissure Mohamed M. Radwan, Khalil Ramdan, Ismail Abu-Azab, Fikri M. Abu-Zidan 1, Department of Surgery,Al-Ain Hospital and Department of Surgery 1, Faculty of Medicine and Health Sciences, UAE University,Al-Ain, United Arab Emirates. Correspondence Fikri M.Abu-Zidan, MD, FRCS, PhD, DipApplStats, Associate Professor, Department of Surgery, Faculty of Medicine and Health Sciences, PO Box 17666,Al Ain, United Arab Emirates Fax: +971 3 7672067 E-mail: fabuzidan@uaeu.ac.ae Code Number: hs07004 Abstract Objectives: To evaluate the effectiveness of Botulinum toxin injection in the treatment of anal fissure. Key words:Anal fissure,chronic, botulinum toxin, sphincterotomy. Running title: BTX and anal fissure Introduction Anal fissure is a common disease. It causes considerable discomfort, loss of working days, and reduction in quality of life 1, 2. It was first described by Recamier in1829 who recommended stretching the anal sphincter to treat this condition.3 Anal fissure affects all age groups, particularly young adults.2 Ninety percent of all fissures occur posteriorly and 10 percent anteriorly. Less than 1 percent of patients have both anterior and posterior fissures. 3 Symptoms of anal fissure include anal pain during defecation and bleeding per anus. 4 Acute anal fissure is treated conservatively with fiber supplement, stool softeners and generous intake of water along with sitz baths and local anesthetic ointment, which usually bring about complete healing. 5 However, chronic anal fissure, does not usually respond to conservative treatment.4 The internal sphincter spasm is the main factor in the pathogenesis of chronic anal fissure.6 Therefore the treatment of this condition is aimed to reduce the internal sphincter hypertonia.4,7 Lateral internal sphicterotomy is the most frequently performed surgical procedure for treatment of chronic anal fissure which results in healing rate of 90 to 95% 3. It works by reducing the sphincter hypertonia which is the main etiological factor in the development of chronic anal fissure.6It may cause minor but permanent incontinence.8Several therapeutic alternatives were proposed to reduce anal pressure leaving the sphincter ring intact to avoid incontinence.5, 6Botulinum toxin (BTX) injection in the internal sphincter muscle has become an acceptable alternative for internal anal sphincterotomy.8-10It eliminates the spasm of the internal anal sphincter by blockage of neurotransmission without internal anal sphincter muscle disruption (chemical sphincterotomy). 10, 11We aimed in this study to evaluate the effectiveness of BTX injection in the treatment of anal fissure. Methods Thirty eight patients who have presented to Surgical Outpatient Clinic at Al-Ain Hospital, United Arab Emirates, with anal fissure in the period between June 2000 and September 2001 and treated with Botulinum toxin injection were retrospectively studied. They were 22 males and 16 females (M: F ratio is 1.4: 1) with a mean age (SD) of 33.3 (8.3) years. The patients were injected with BTX type A (Botox, Allergen). A total dose of 10-20 U was diluted in 1ml isotonic saline and injected while the patient was lying on his/her left side. An insulin syringe and a (26 G) needle were used for injection. The injection was done in the internal anal sphincter. Half of this dose was injected on both sides of the fissure in 27 cases, at 3 and 9 o’clock positions in 10 cases, and at the base and the apex of the fissure in one case. No sedation or local anesthesia was used. The patients were followed up after one week and then every two weeks until the fissure healed or surgery was required. The patients were followed up for at least 8 weeks to evaluate the effects of treatment. The patients’ records were reviewed for improvement, healing, occurrence of side effects, surgery, as well as recurrence of symptoms. Results The patients were classified depending on the location, complications and onset of the fissure (table 1). The main indication for use of BTX injection in our patients was chronic anal fissure that did not heal after 6 weeks of conservative treatment. The best results of BTX injection were achieved in patients having chronic posterior uncomplicated anal fissures. The follow up results of those patients (n = 28) after one and eight weeks of BTX injection are shown in table (2). 23/28 of these patients were cured after initial therapy. Of the five (5/28) patients whom had relapse of symptoms three (3/28) were reinjected and followed up in the same manner. The other two had surgery. Of the three reinjected patients, two had healed fissures and the other one did not come for follow up. So the total number of patients who ultimately had healing after BTX injection is 25/28 (89%). Of the 28 patients diagnosed as having chronic posterior uncomplicated anal fissure, 19 were males and 9 were females. There was no difference between genders in outcome. The two patients who underwent surgery were males (p=1, Fisher’s exact test). The 3 patients who got recurrence and were reinjected were males (p=1, Fisher’s exact test). After one week of BTX injection 2/28 patients experienced minor incontinence in the form of a fecal soiling. One was a male and the other was a female (p=0.53, Fisher’s exact test). This has disappeared later. All 28 patients remained continent after 8 weeks. No other complications have been noticed. Discussion Our present study has shown that BTX injection for treatment of chronic anal fissure is a safe effective method. The indication of BTX injection (chemical sphincterotomy) is similar to surgical lateral sphincterotomy which is chronic idiopathic anal fissure with comparable success rate in both procedures. The resting pressure in the anal canal is largely a function of the internal sphincter. The continuous partial contraction of the sphincter is due to an inherent myogenic tone and alpha adrenergic nerve mediated pathways.6 Patients with chronic anal fissure usually have a raised resting anal pressure due to hypertonicity of the internal sphincter4. This compromises perfusion of the anal mucosa as the blood vessels supplying the distal anal canal traversing the internal sphincter en route to the anal mucosa may be compressed by the hypertonic muscle leading to chronic anal fissure. This is why chronic anal fissure has been described as an ischemic ulcer.12, 13 By reducing the sphincter hypertonia, lateral internal sphincterotomy improves the perfusion of the distal anal mucosa and leads to healing of the chronic anal fissure in 90-95% of cases.3, 13 In spite of the high healing rate, internal anal sphicterotomy has drawbacks, namely: incontinence, complications related to wound healing, the need for hospitalization, and the anesthesia risk.14, 15 A large study of patients who underwent lateral sphincterotomy has shown that incontinence to flatus can reach up to 35%. 15 In another study, endoanal ultrasound has demonstrated extensive sphincter defects in patients after lateral sphincterotomy. 16 Even if the patient remains continent following sphincterotomy, muscle disruption is permanent. Patients would be at risk of incontinence in later life because resting pressure decreases with age .17 BTX blocks sympathetic nerve function and myognic tone of the internal anal sphincter (chemical sphinctrotomy), eliminating the sphincter hypertonia resulting in increase in the local tissue perfusion and healing of the chronic anal fissure.6, 13, 18 Muscle paralysis occurs within hours and the effect remains for 3-4 months.This prolonged effect allows the fissure to heal. This effect is reversible because it is followed by axonal regeneration and formation of new nerve endings which avoids the risk of permanent injury to the sphincter.4, 9, 11, 19 BTX has a direct analgesic effect causing relief before the healing of the fissure (2, 20, 21). BTX has also a good safety profile and tolerability (22). The median lethal dose of BTX (LD50) is estimated to be 3000 U for a 70- kg male (19). Only a total dose of 20U was used to produce healing of the chronic anal fissure. Other pharmacological agents affecting chemical sphincterotomy include topical glceryl trinitrate and calcium channel antagonists.23, 24, 25 BTX injection is suitable for treatment of chronic idiopathic anal fissure associated with increased anal sphincter tone and not associated or complicated by other anal diseases which require surgical treatment such as fistula in ano or hemorrhoids. BTX injection is a simple procedure, easy to learn, and can be done in the outpatient clinic without the need for sedation or local anesthesia. It is cost effective and leads to healing of the fissure avoiding surgery with its potential risk of incontinence.The site of injection in the internal sphincter ring, the gender and the age of the patient do not appear to affect the outcome of the treatment. BTX injection has no side effects apart from low incidence of minor transitory incontinence. In summary we have shown that BTX injection is a suitable first-line treatment of choice for chronic idiopathic anal fissure, which is not associated with other anal conditions. Surgery should be offered to patients who do not improve with Botulinum toxin injection and to those with complicated anal fissure. Patients presenting with chronic idiopathic anal fissure should be informed about the available treatment options as well as their risks. References
Copyright © 2007 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs07004t1.jpg] [hs07004t2.jpg] |
| |||||||||

{kind=link}
{kind=link}